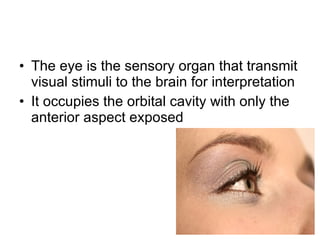
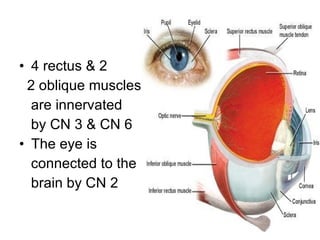
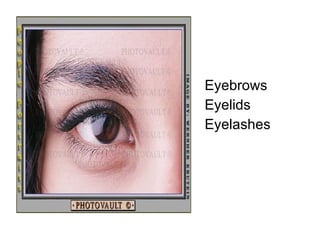
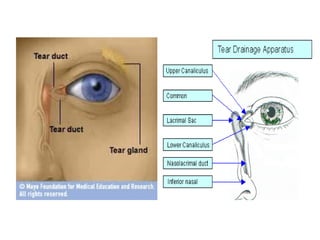
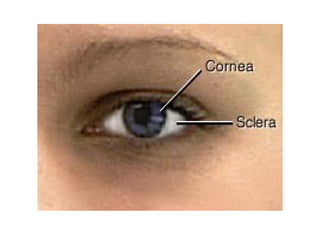
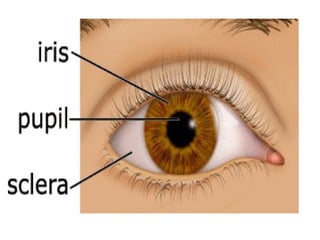
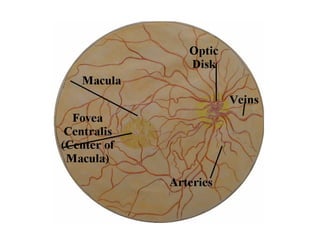
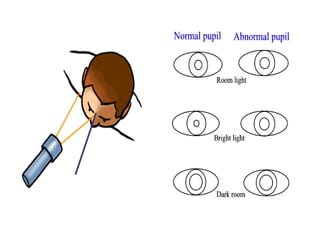
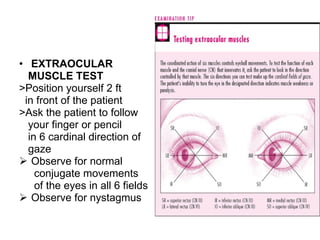
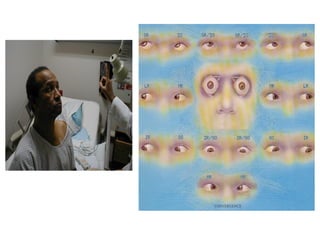
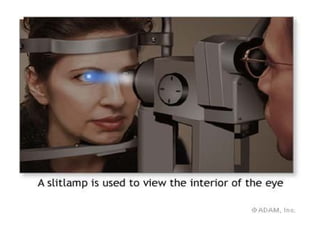
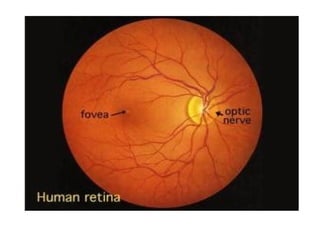
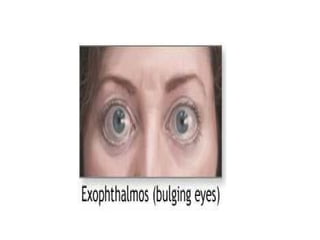
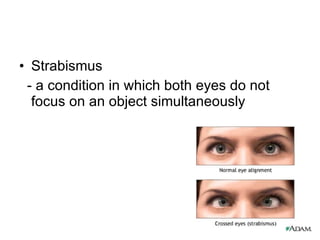
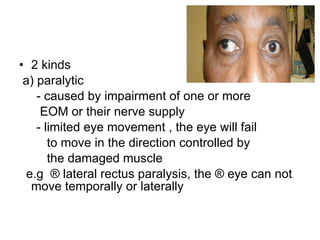
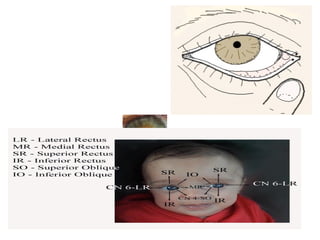
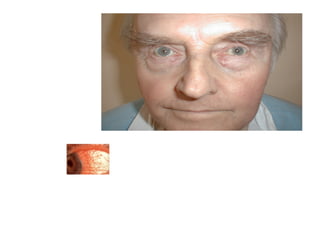
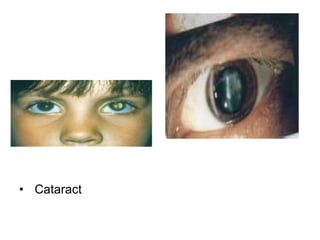
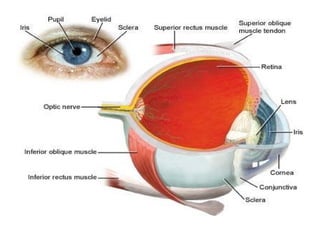
The document provides an overview of eye anatomy and examination procedures. It describes the external structures of the eye including the eyelids, muscles, and lacrimal apparatus. Internally, it outlines the three layers of the eye - sclera, choroid, and retina. Examination steps are detailed including visual acuity tests, pupil examination, eye muscle function, ophthalmoscopy, and visual field testing. Common eye signs and conditions like strabismus, cataracts, and hemorrhages are also summarized.

















































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




