
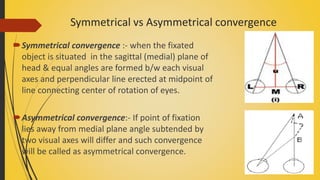
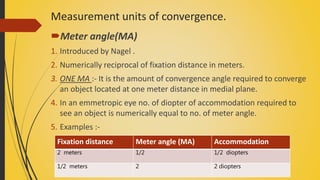
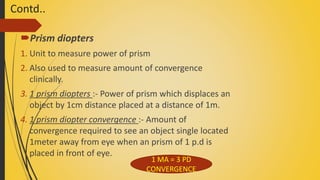


Convergence is the inward movement of the eyes to maintain single binocular vision. It can be symmetrical or asymmetrical depending on the position of the fixation point. The near point of convergence is the closest point an object can be focused on binocularly and is measured clinically. Convergence insufficiency is the most common convergence anomaly and causes eye strain. Other anomalies include convergence paralysis which is a total lack of convergence ability due to brain lesions. Convergence spasm involves intermittent periods of excessive convergence that can cause diplopia. Exercises are used to treat convergence insufficiency while prisms are used for convergence paralysis.























































































