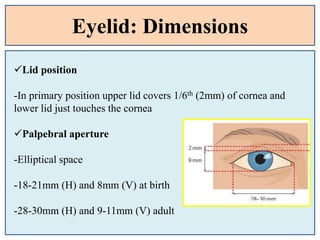
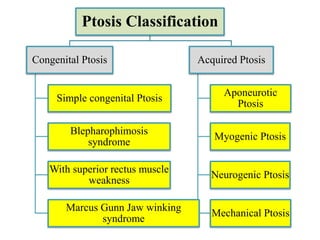
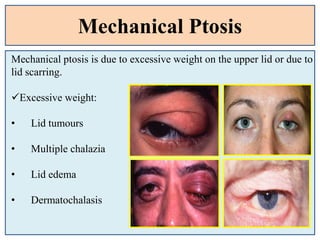
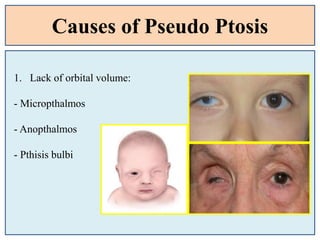
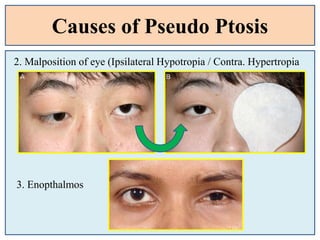
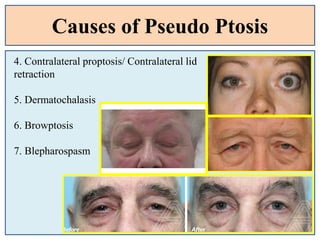
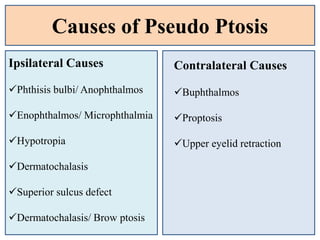
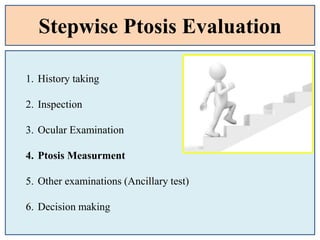

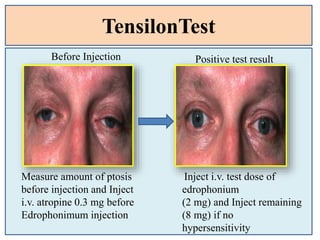
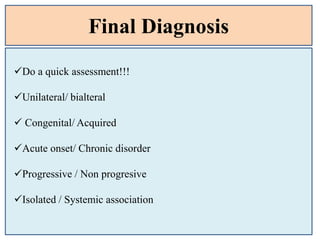
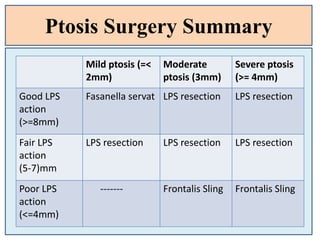
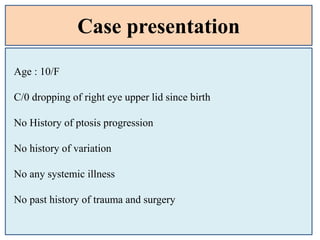
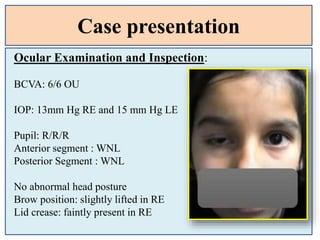
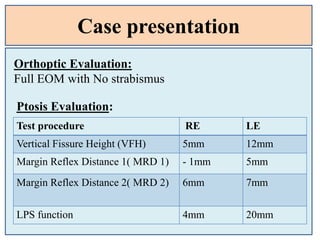
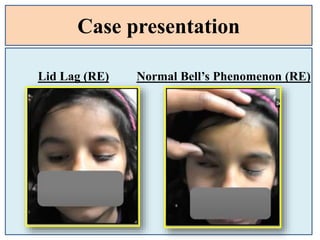


This document provides an overview of blepharoptosis (ptosis) including its classification, evaluation, and case study. It begins with an introduction to ptosis and eyelid anatomy. It then covers the types of ptosis such as congenital, acquired, and pseudo ptosis. The evaluation section details the history taking, inspection, measurements including levator function, margin reflex distance, and margin crease distance. It also discusses ancillary tests and differential diagnosis. Overall, the document serves as a guide for clinicians to classify and evaluate different types of ptosis.























































































