Past history
• Underlyingdisease OA knees ปัจจุบันรักษาอยู่ที่ รพ.โนนฝรั่ง ด้วย medication ปวด
เข่าไม่บ่อย
• เคยประสบอุบัติเหตุรถชนเมื่อ 10+ ปีก่อน ทาให้ขาขวาหัก จึงต้องผ่าตัดดามเหล็กที่ขาขวา
• ไม่เคยไหล่หลุดมาก่อน
• No drug and food allergy
• Current med : Naproxen(250) 1x2 PO pc , Omeprazole(20) 1xhs
6.
Personal history
• Noalcohol drinking , not smoke
• No herbal used
• No family history of genetic disease
7.
Physical examination
• Vitalsigns – T 36.8 , PR 76 bpm , RR 18 /min , BP 161/75 mmHg
• General appearance – A Thai old woman , alert , good conscious
• HEENT - not pale conjunctivae , anicteric sclerae , no wound
• CVS – normal s1 s2 sound , no murmur
• Respiratory – Clear and equal breath sound both lung , no
adventitious sound
• Abdomen – soft , not tender
• Skin – no ecchymosis , no laceration or abrasion wound
8.
• Extremities
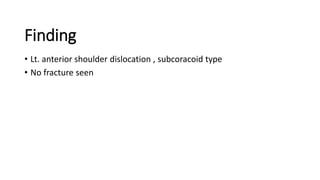
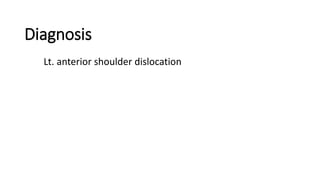
Lt.shoulder –loss of normal shoulder contour , no external wound seen
Arm position is in abduction and external rotation
Tender along shoulder , palpable head of Lt. humerus
limit ROM of shoulder joint due to pain
full ROM of elbow and wrist joint
Ruler’s test positive , Duga’s test negative (can touch)
sensory intact , radial pulse 2+
Other - WNL
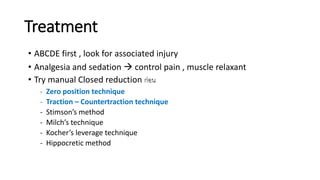
Management
• Pain control morphine 3 mg IV stat
• Sedation Diazepam 5 mg IV stat
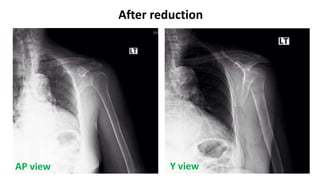
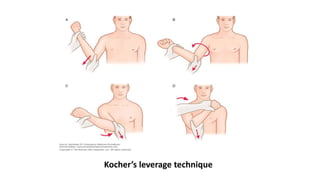
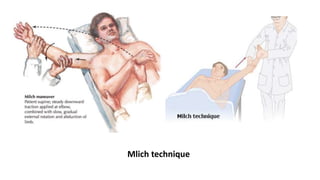
• Closed reduction then on arm sling
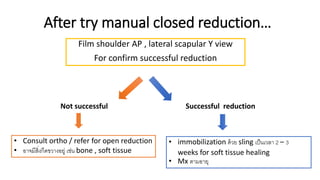
• Film Lt. shoulder AP , Lateral scapula Y view หลังจาก reduction เสร็จ
if successful plan Discharge and F/U OPD ortho 2 wks
Shoulder dislocation
• 50%of all major joint dislocations.
• Anterior dislocation is most common 95 - 97 % of cases.
Posterior dislocation 2 – 4%
Inferior dislocation 0.5 %
• high recurrence rate that correlates with age at dislocation
up to 80-90% in teenagers (90% chance for recurrence in age >20)
19.
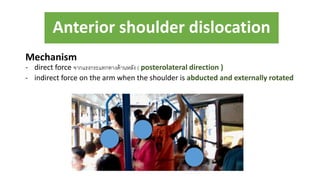
Anterior shoulder dislocation
Mechanism
-direct force จากแรงกระแทกทางด้านหลัง ( posterolateral direction )
- indirect force on the arm when the shoulder is abducted and externally rotated
20.
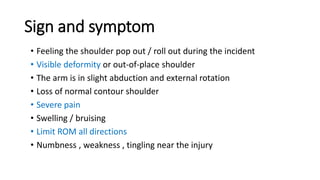
Sign and symptom
•Feeling the shoulder pop out / roll out during the incident
• Visible deformity or out-of-place shoulder
• The arm is in slight abduction and external rotation
• Loss of normal contour shoulder
• Severe pain
• Swelling / bruising
• Limit ROM all directions
• Numbness , weakness , tingling near the injury
23.
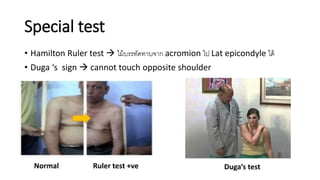
• Hamilton Rulertest ไม้บรรทัดทาบจาก acromion ไป Lat epicondyle ได้
• Duga ‘s sign cannot touch opposite shoulder
Special test
Normal Ruler test +ve Duga’s test
24.
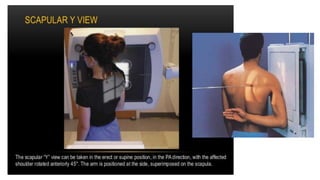
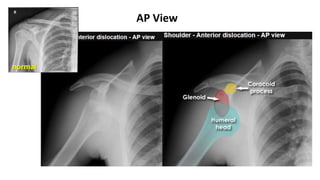
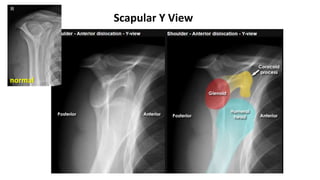
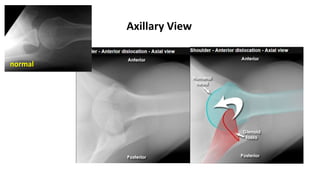
Imaging
• Plain radiographs– for diagnosis and exclude fracture
Routine films : AP view , Scapular Y view , Axillary view (ไม่นิยม)
finding : humeral head comes to lie anteromedial
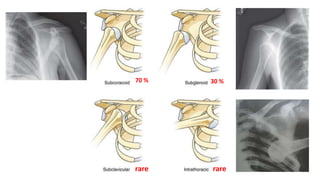
1. Subcoracoid (m/c)
2. Subglenoid
3. Subclavicular
4. Intrathoracic
4 subtype
Complication
• Recurrent shoulderdislocation (m/c complication)
- Age is the most important indicator for prognosis 90% of teenagers
• Fracture
- m/c is Hill-Sachs lesion (compression fracture of the posterior humeral head)
- proximal humerus , greater tuberosity , coracoid , acromion
• Rotator cuffs tear
- increases with age 30-35% of patients aged 40 years or older
• Nerve injury
- m/c is axillary nerve up to 33% of acute anterior dislocations
• Vascular injury
- rare , older patients
- more common with inferior dislocations , branch of axillary a.