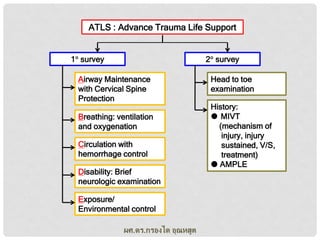
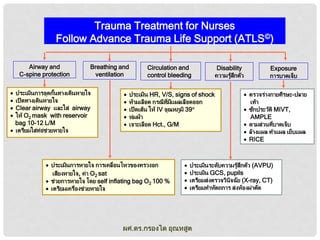
ATLS : AdvanceTrauma Life Support
1 survey
2 survey
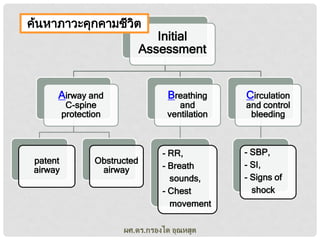
Airway Maintenance
with Cervical Spine
Protection
Breathing: ventilation
and oxygenation
Circulation with
hemorrhage control
Disability: Brief
neurologic examination
Exposure/
Environmental control
ผศ.ดร.กรองได อุณหสูต
Head to toe
examination
History:
MIVT
(mechanism of
injury, injury
sustained, V/S,
treatment)
AMPLE
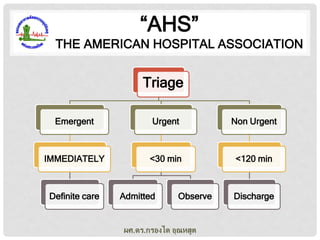
“AHS”
THE AMERICAN HOSPITALASSOCIATION
Triage
Emergent
Urgent
Non Urgent
IMMEDIATELY
<30 min
<120 min
Definite care
Admitted
Observe
ผศ.ดร.กรองได อุณหสูต
Discharge
14.
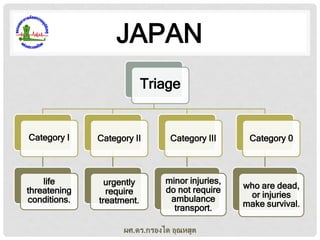
JAPAN
Triage
Category I
Category II
CategoryIII
Category 0
life
threatening
conditions.
urgently
require
treatment.
minor injuries,
do not require
ambulance
transport.
who are dead,
or injuries
make survival.
ผศ.ดร.กรองได อุณหสูต
15.
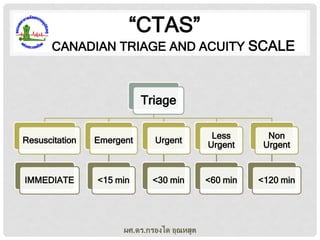
“CTAS”
CANADIAN TRIAGE ANDACUITY SCALE
Triage
Resuscitation
Emergent
Urgent
Less
Urgent
Non
Urgent
IMMEDIATE
<15 min
<30 min
<60 min
<120 min
ผศ.ดร.กรองได อุณหสูต
16.
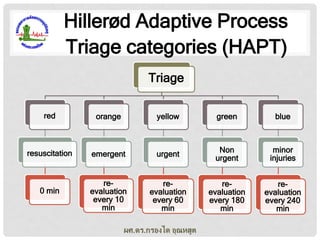
Hillerød Adaptive Process
Triagecategories (HAPT)
Triage
red
orange
yellow
green
blue
resuscitation
emergent
urgent
Non
urgent
minor
injuries
reevaluation
every 10
min
reevaluation
every 60
min
reevaluation
every 180
min
reevaluation
every 240
min
0 min
ผศ.ดร.กรองได อุณหสูต
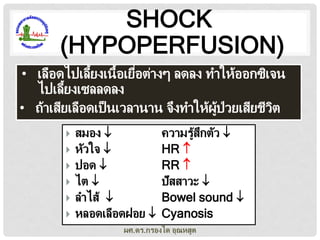
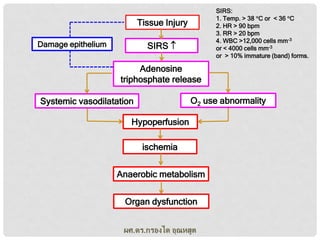
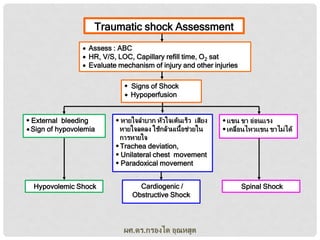
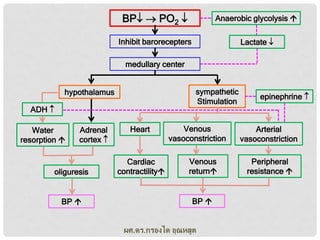
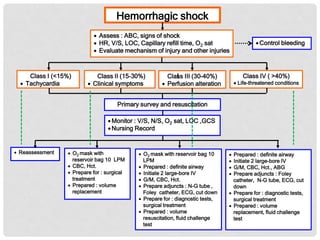
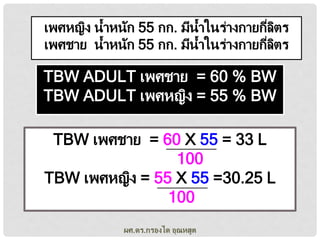
Hemorrhagic shock
Assess: ABC, signs of shock
HR, V/S, LOC, Capillary refill time, O2 sat
Evaluate mechanism of injury and other injuries
Class I (<15%)
Tachycardia
Class II (15-30%)
Clinical symptoms
Control bleeding
Class IV ( >40%)
Class III (30-40%)
Perfusion alteration
Life-threatened conditions
Primary survey and resuscitation
Monitor : V/S, N/S, O2 sat, LOC ,GCS
Nursing Record
Reassessment
O2 mask with
reservoir bag 10 LPM
CBC, Hct.
Prepare for : surgical
treatment
Prepared : volume
replacement
O2 mask with reservoir bag 10
LPM
Prepared : definite airway
Initiate 2 large-bore IV
G/M, CBC, Hct.
Prepare adjuncts : N-G tube ,
Foley catheter, ECG, cut down
Prepare for : diagnostic tests,
surgical treatment
Prepared : volume
resuscitation, fluid challenge
test
Prepared : definite airway
Initiate 2 large-bore IV
G/M, CBC, Hct., ABG
Prepare adjuncts : Foley
catheter, N-G tube, ECG, cut
down
Prepare for : diagnostic tests,
surgical treatment
Prepared : volume
replacement, fluid challenge
test
24.
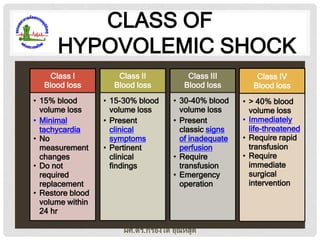
CLASS OF
HYPOVOLEMIC SHOCK
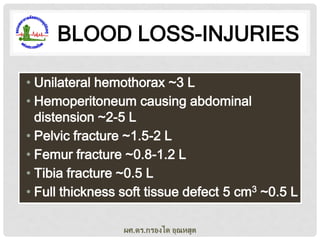
ClassI
Blood loss
Class II
Blood loss
Class III
Blood loss
Class IV
Blood loss
• 15% blood
volume loss
• Minimal
tachycardia
• No
measurement
changes
• Do not
required
replacement
• Restore blood
volume within
24 hr
• 15-30% blood
volume loss
• Present
clinical
symptoms
• Pertinent
clinical
findings
• 30-40% blood
volume loss
• Present
classic signs
of inadequate
perfusion
• Require
transfusion
• Emergency
operation
• > 40% blood
volume loss
• Immediately
life-threatened
• Require rapid
transfusion
• Require
immediate
surgical
intervention
ผศ.ดร.กรองได อุณหสูต
25.
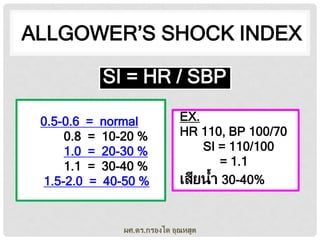
ALLGOWER’S SHOCK INDEX
SI= HR / SBP
0.5-0.6 = normal
0.8 = 10-20 %
1.0 = 20-30 %
1.1 = 30-40 %
1.5-2.0 = 40-50 %
EX.
HR 110, BP 100/70
SI = 110/100
= 1.1
เสียน้า 30-40%
ผศ.ดร.กรองได อุณหสูต
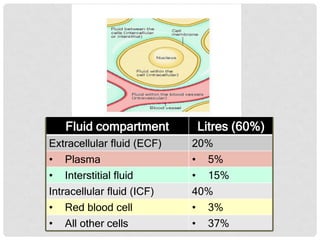
FLUID REPLACEMENT
• 2large-bore 14-16-18 gauge IV catheters
• Initial bolus of 1-2 L of RLS rapidly as possible
• Large bore, short catheter, short IV tubing,
rapid infuser device
• Isotonic solution, Electrolyte-balanced, or
Crystalloid solution before blood or colloid
• Observe SBP, HR, breath sounds response to
bolus
ผศ.ดร.กรองได อุณหสูต
29.
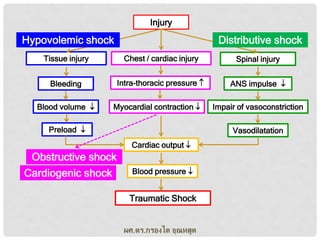
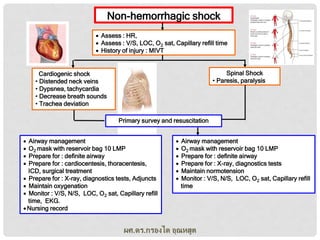
Non-hemorrhagic shock
Assess: HR,
Assess : V/S, LOC, O2 sat, Capillary refill time
History of injury : MIVT
Spinal Shock
• Paresis, paralysis
Cardiogenic shock
• Distended neck veins
• Dypsnea, tachycardia
• Decrease breath sounds
• Trachea deviation
Primary survey and resuscitation
Airway management
O2 mask with reservoir bag 10 LMP
Prepare for : definite airway
Prepare for : cardiocentesis, thoracentesis,
ICD, surgical treatment
Prepare for : X-ray, diagnostics tests, Adjuncts
Maintain oxygenation
Monitor : V/S, N/S, LOC, O2 sat, Capillary refill
time, EKG.
Nursing record
Airway management
O2 mask with reservoir bag 10 LMP
Prepare for : definite airway
Prepare for : X-ray, diagnostics tests
Maintain normotension
Monitor : V/S, N/S, LOC, O2 sat, Capillary refill
time
ผศ.ดร.กรองได อุณหสูต
30.
TREATMENT
• requires immediatetreatment,
• initial intervention includes immobilization of the
head, neck, and back, and steroid medications
to control swelling.
• immediate surgery is necessary to evaluate the
state of the spinal cord, stabilize fractured
vertebrae, release pressure from the injured
area, and treat injuries to other parts of the body.
ผศ.ดร.กรองได อุณหสูต