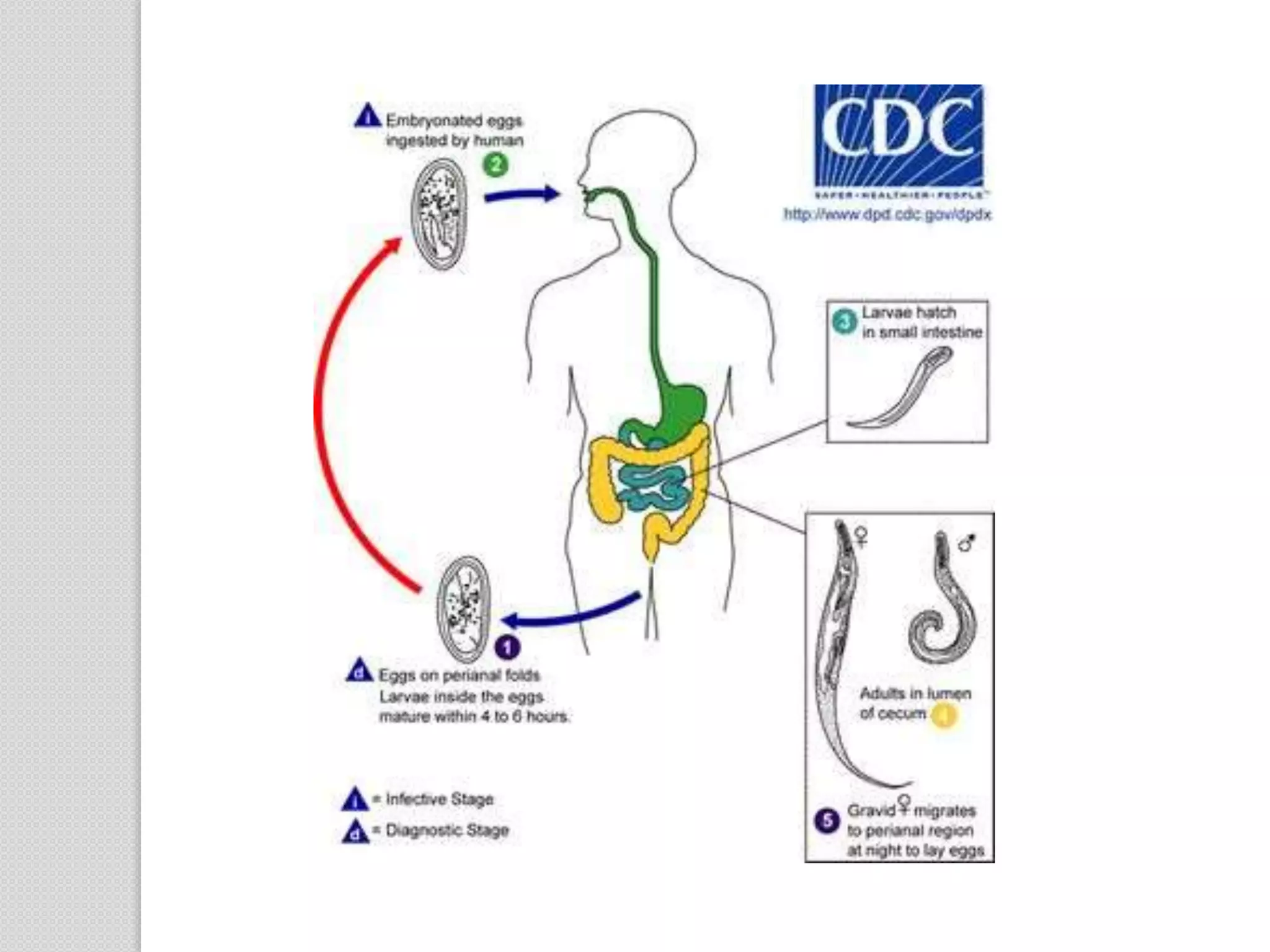
Enterobius vermicularis, commonly known as the pinworm or threadworm, is a parasitic nematode that infects the large intestine of humans. It has a worldwide distribution and is considered the most common human parasite, primarily affecting children. The adult worms live in the cecum and appendix where the female lays eggs around the anal area, causing intense itching and scratching. The eggs can hatch and reinfect the host through autoinfection or contaminate surfaces, transmitting the infection through contaminated hands, food, water, clothing or dust. Diagnosis involves microscopic examination of samples collected from the perianal area to detect eggs. Treatment involves a single dose of anthelmintic medication and repeated treatment to





















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)













