Downloaded 693 times
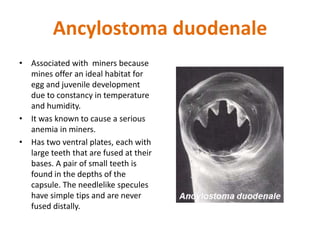

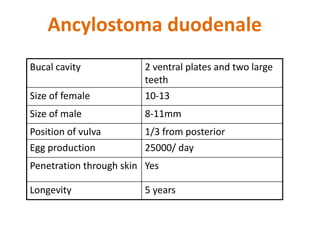
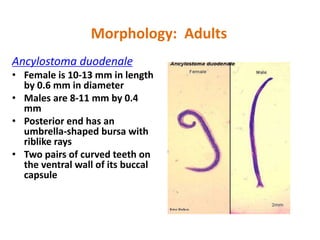
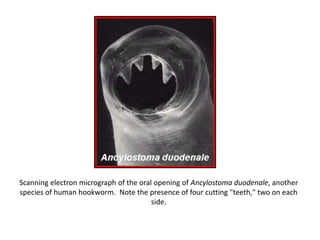
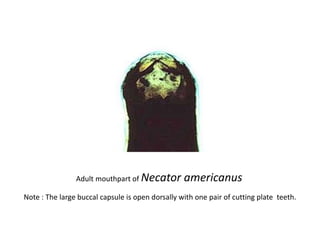
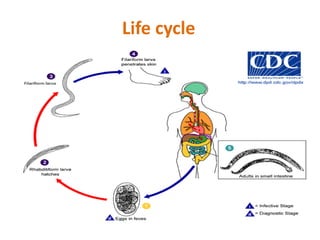
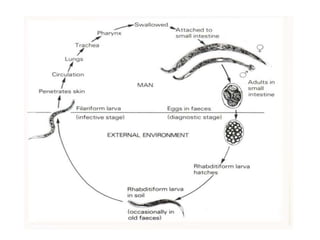
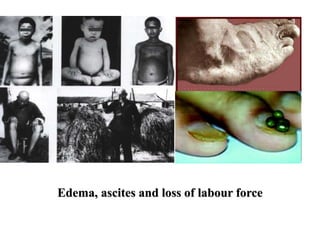
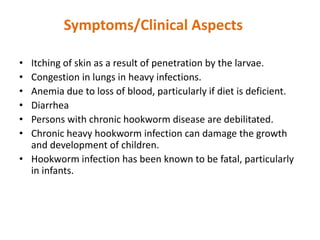
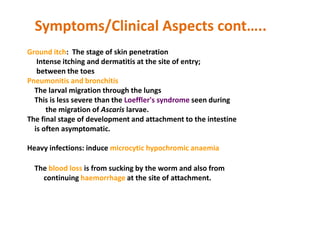

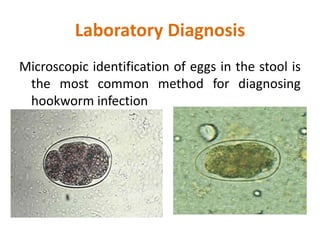
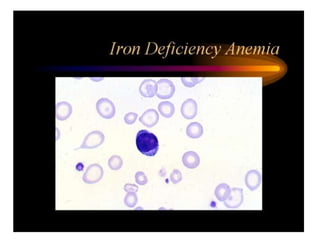
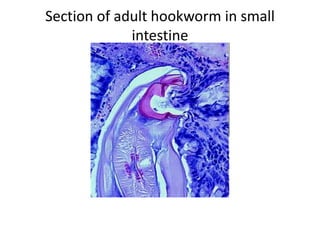


1) Hookworms are blood-feeding nematodes that infect around 900 million people worldwide, principally by the species Ancylostoma duodenale and Necator americanus. 2) A. duodenale is associated with miners due to humid conditions in mines being suitable for egg and larval development. It was known to cause severe anemia in miners. 3) The life cycle involves eggs passing in feces and hatching as larvae that penetrate skin, are carried by blood to lungs, then swallowed and mature as adults in small intestine where they feed on blood, potentially causing iron-deficiency anemia.













![Trypanosoma [1]](https://cdn.slidesharecdn.com/ss_thumbnails/trypanosomaseminar1-170312074241-thumbnail.jpg?width=640&height=640&fit=bounds)
















































































