Download to read offline


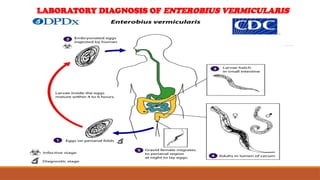

Enterobius vermicularis, commonly known as pinworm, is the world's most prevalent human parasite, predominantly affecting children in affluent regions. The worm infects humans through ingestion of eggs and can cause enterobiasis, characterized by symptoms like anal itching and abdominal pain. Diagnosis typically involves perianal scraping methods, with treatment options including pyrantel pamoate and mebendazole, alongside preventive measures like good hygiene.



































































