Downloaded 317 times

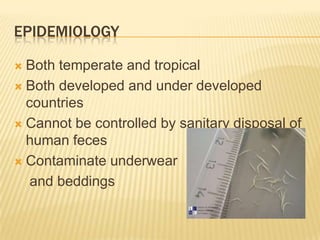


Human pinworm, or Enterobius vermicularis, is an intestinal nematode parasite that causes enterobiasis. It is not fatal but can cause irritation when the female worms migrate to the perianal region to lay eggs. The parasite has a life cycle involving eggs that are ingested and hatch in the intestines, with adult worms mating and females migrating to lay eggs again. Diagnosis is usually by microscopic examination of perianal swabs, and treatment involves anthelmintic drugs. While found worldwide, pinworm infection is especially common in children and spreads easily through contaminated clothing and bedding. Prevention focuses on personal hygiene, handwashing, and treating entire families.




















![[Micro] hymenolepis nana](https://cdn.slidesharecdn.com/ss_thumbnails/3rxjz7ekrwinb1sq3uxs-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)











































































