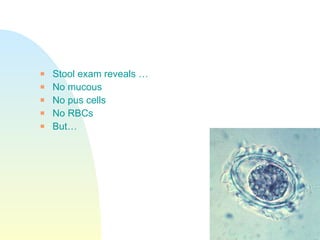
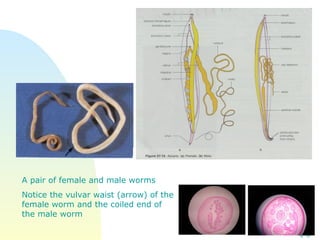
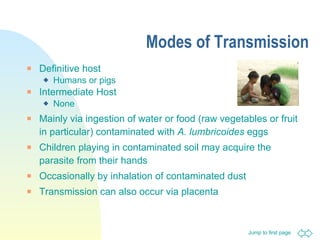
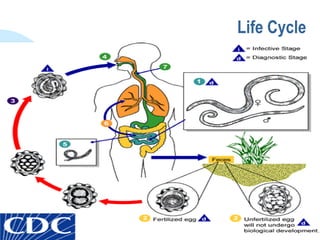
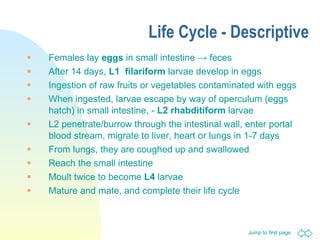

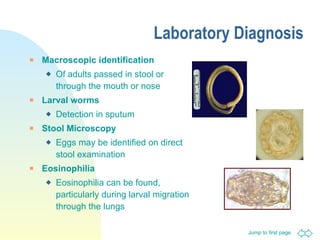
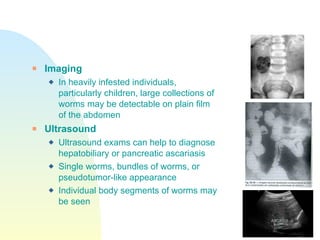

A 6-year-old girl presented with malnourishment, abdominal swelling, cough, wheeze and fever. Imaging revealed lobar pneumonia and suspicion of worms. Stool examination found Ascaris lumbricoides eggs. Ascaris lumbricoides is an intestinal roundworm that infects over 1 billion people worldwide. It is transmitted through ingestion of eggs from contaminated food, water or soil.























































































