Downloaded 2,552 times

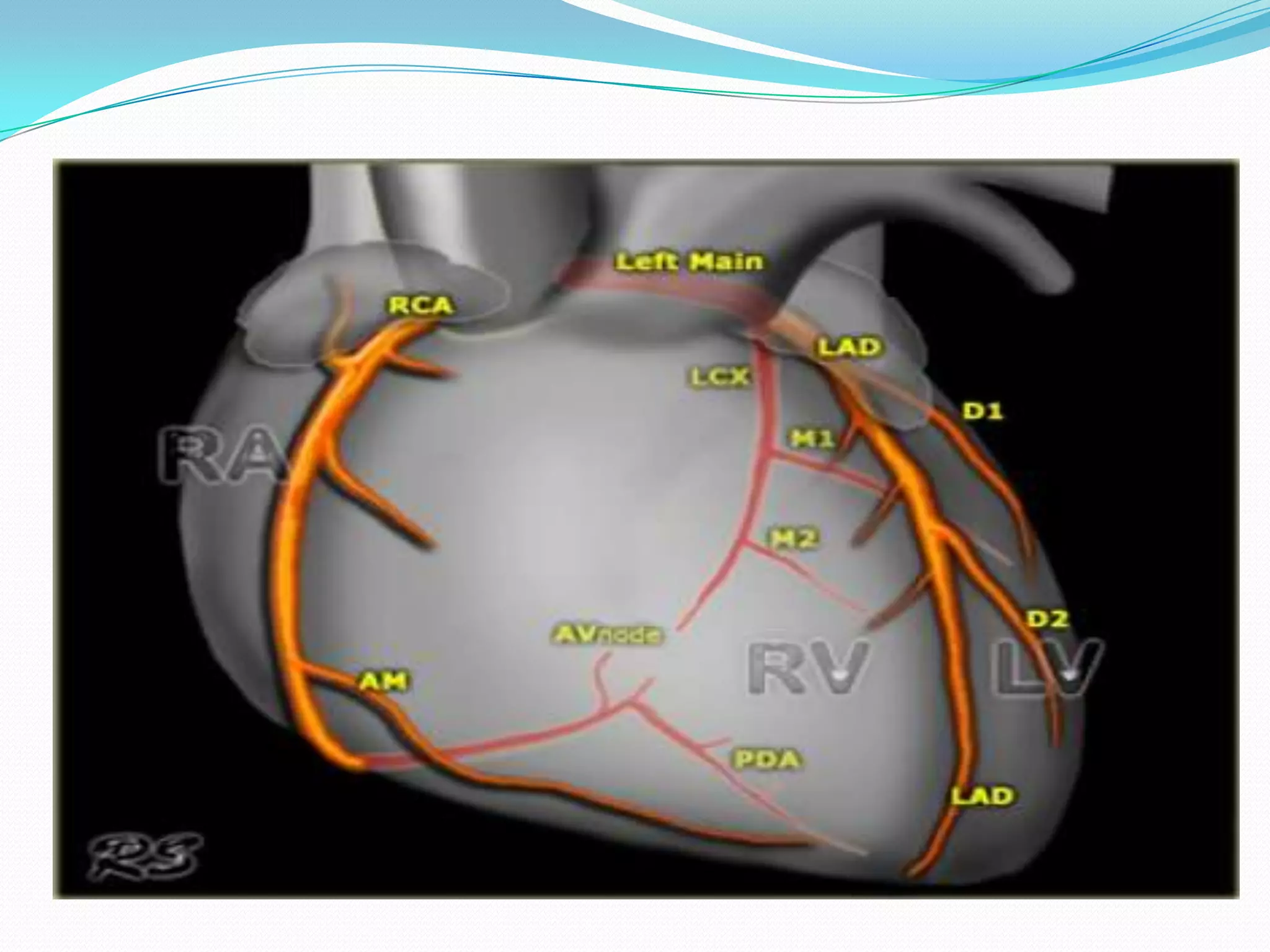
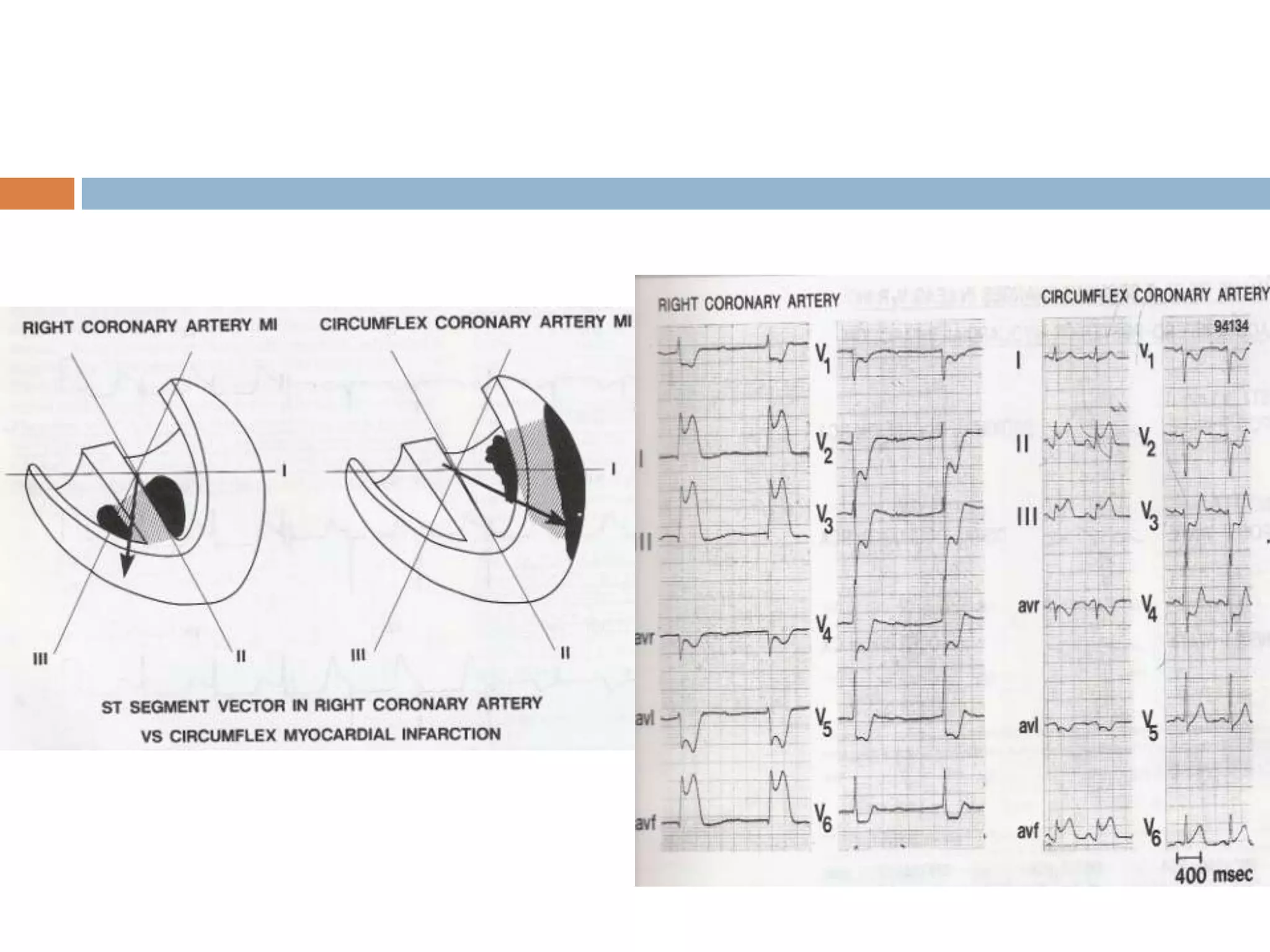
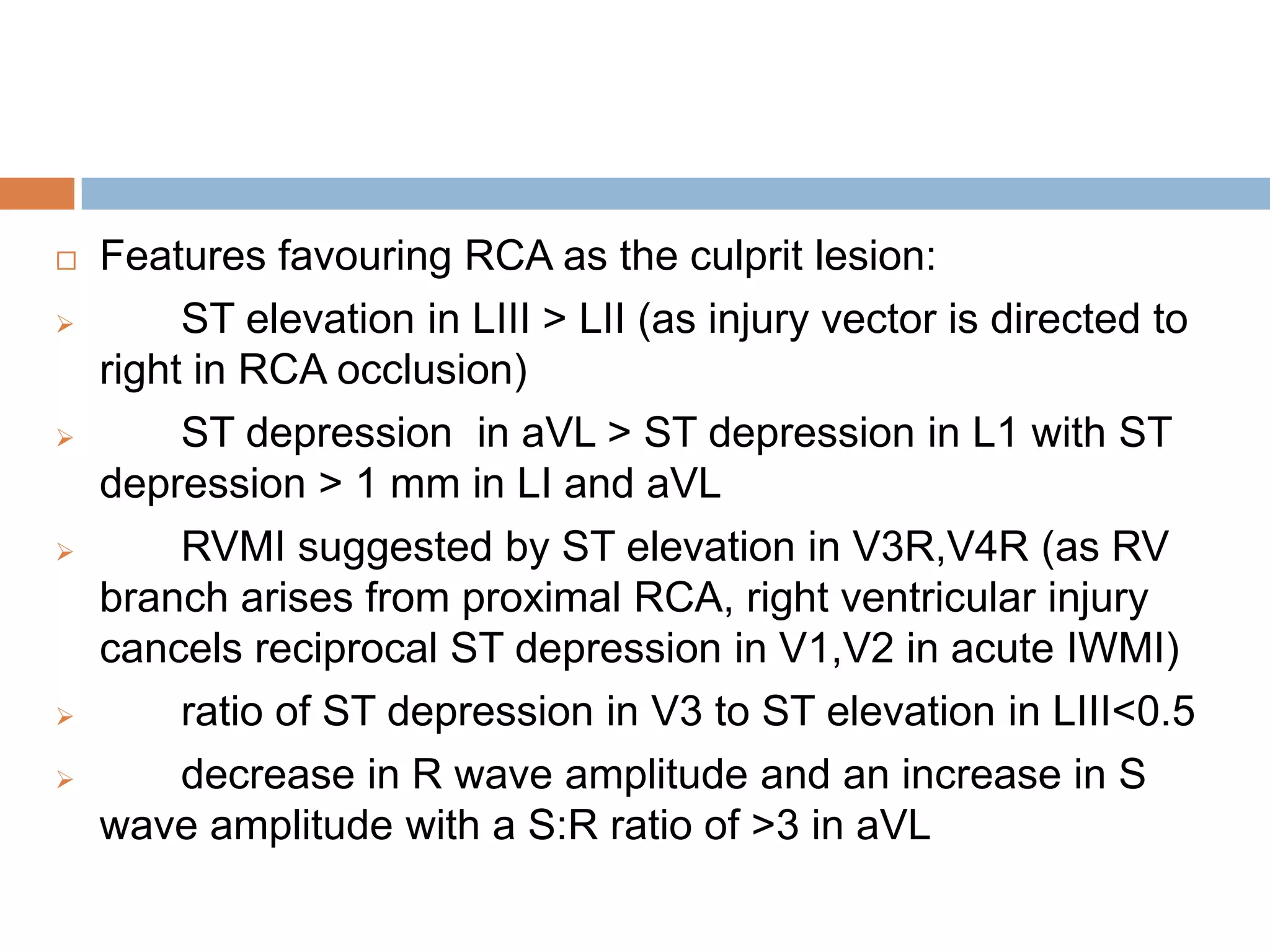
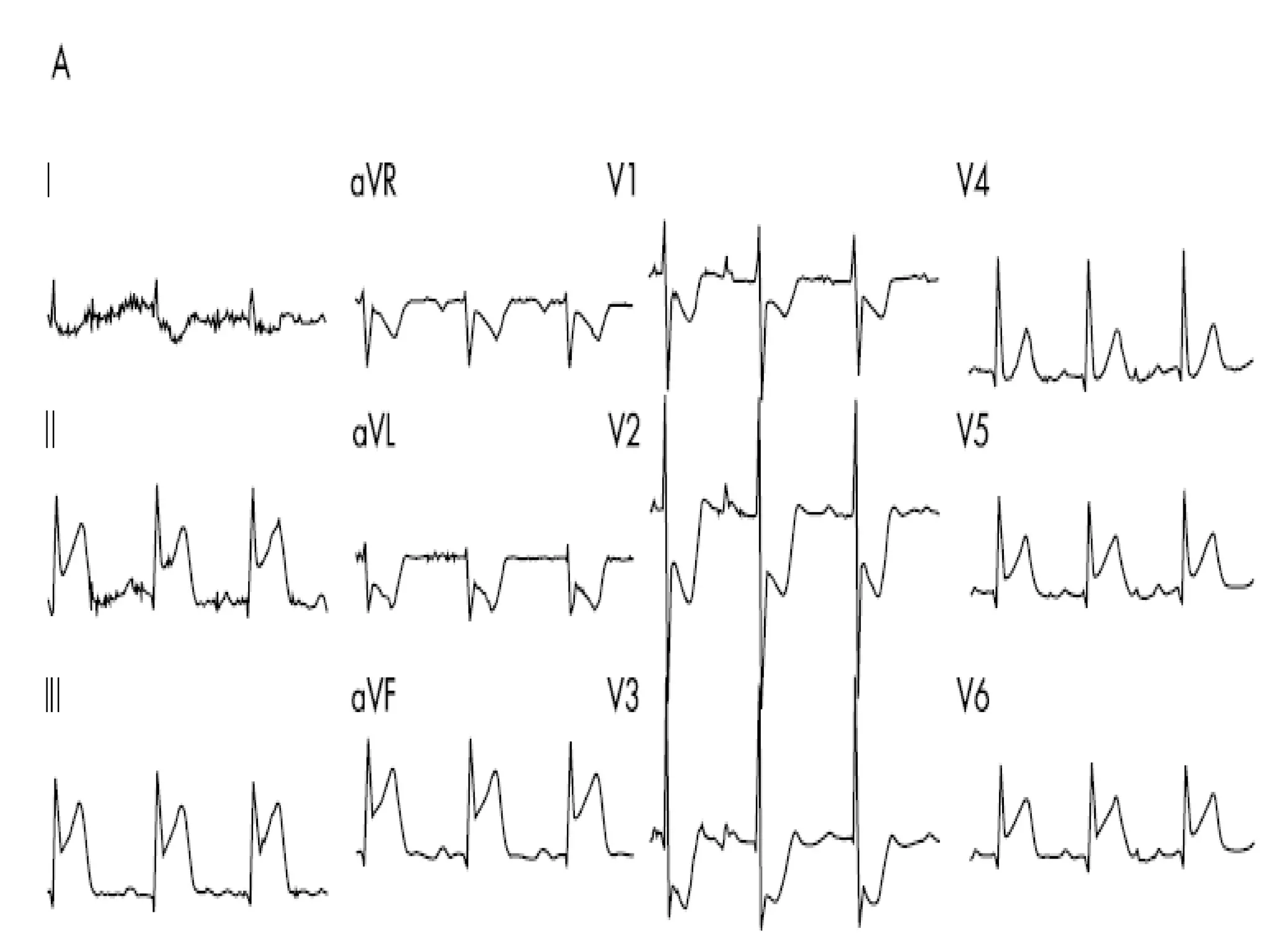
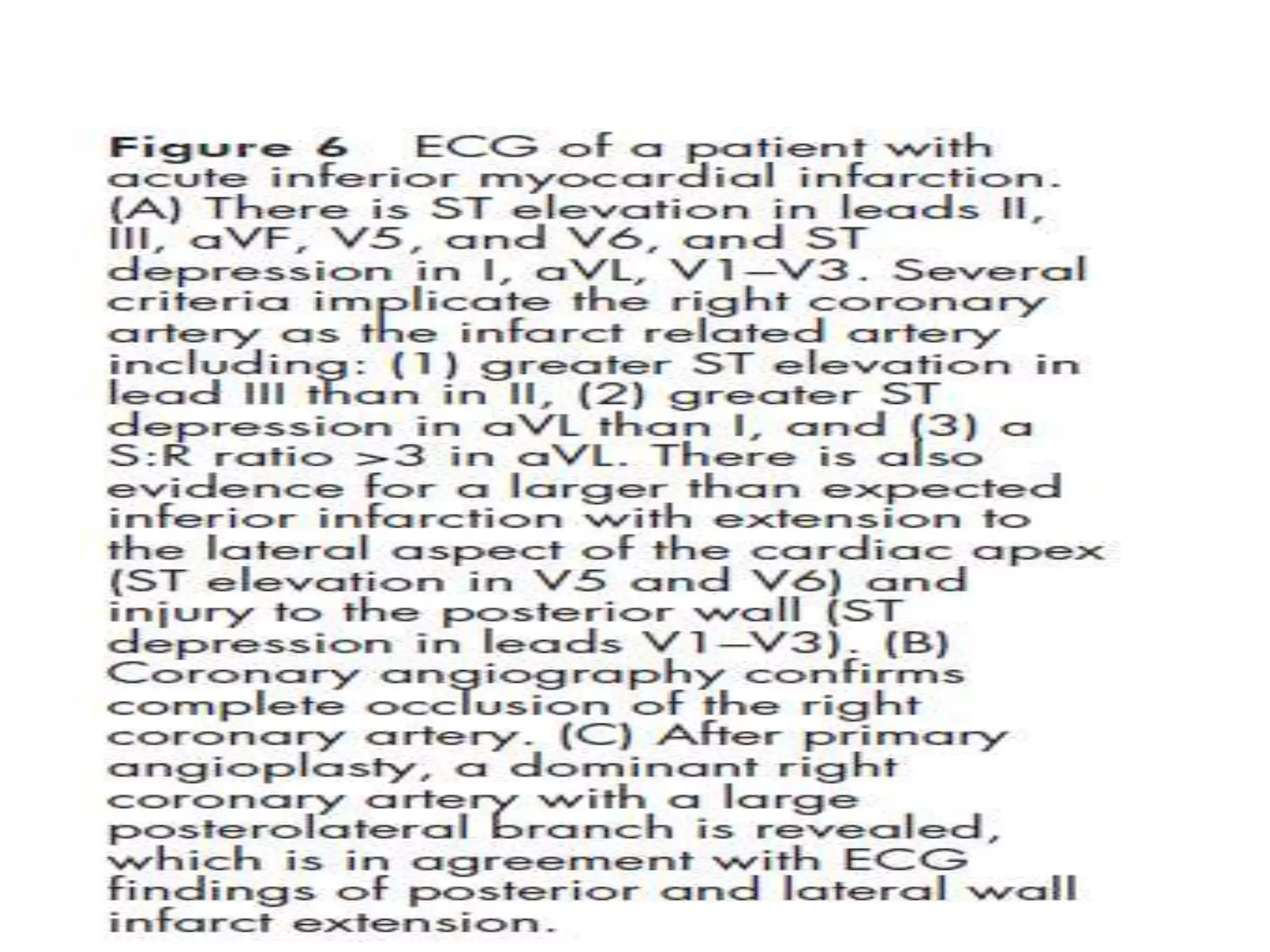
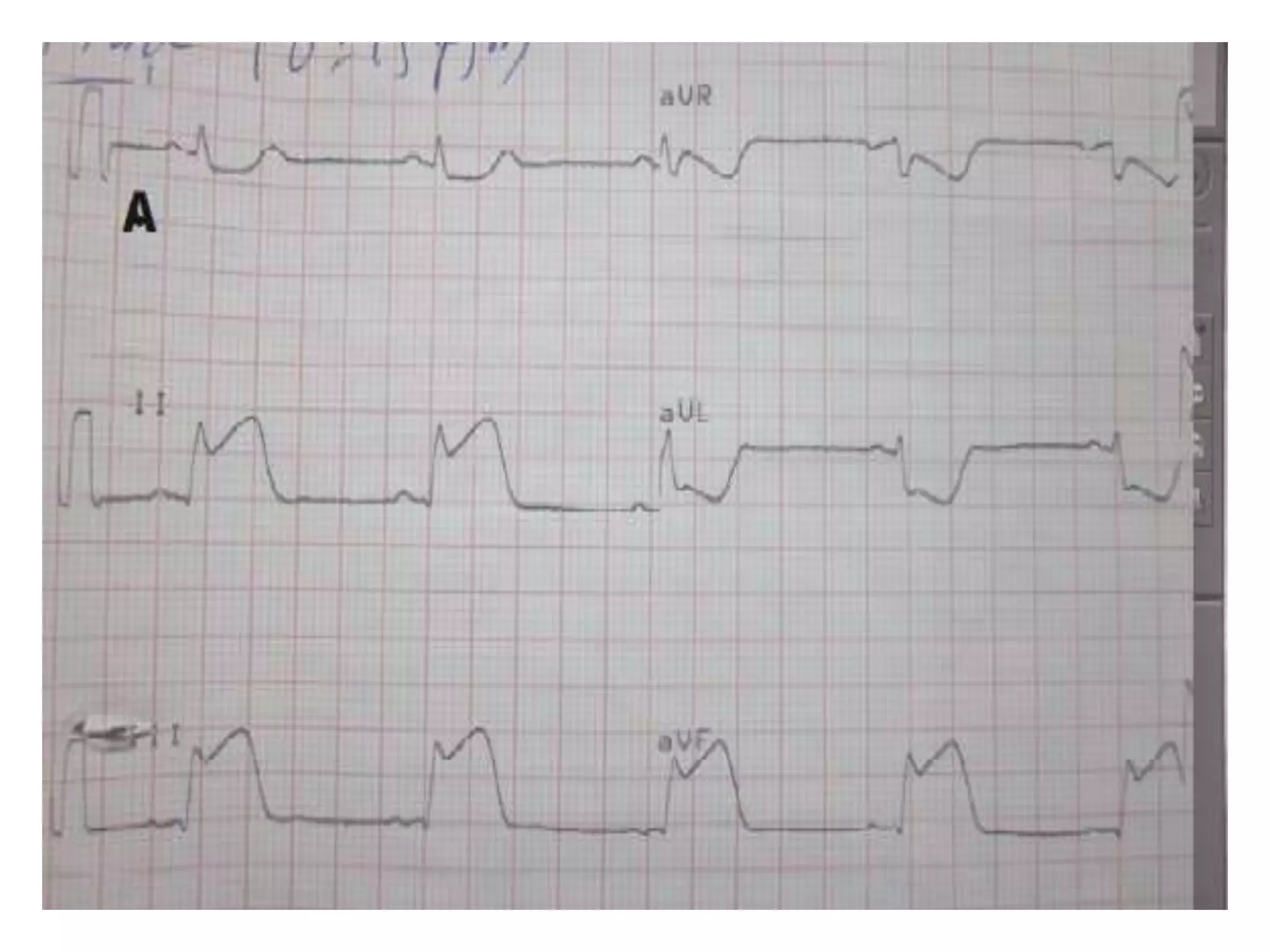
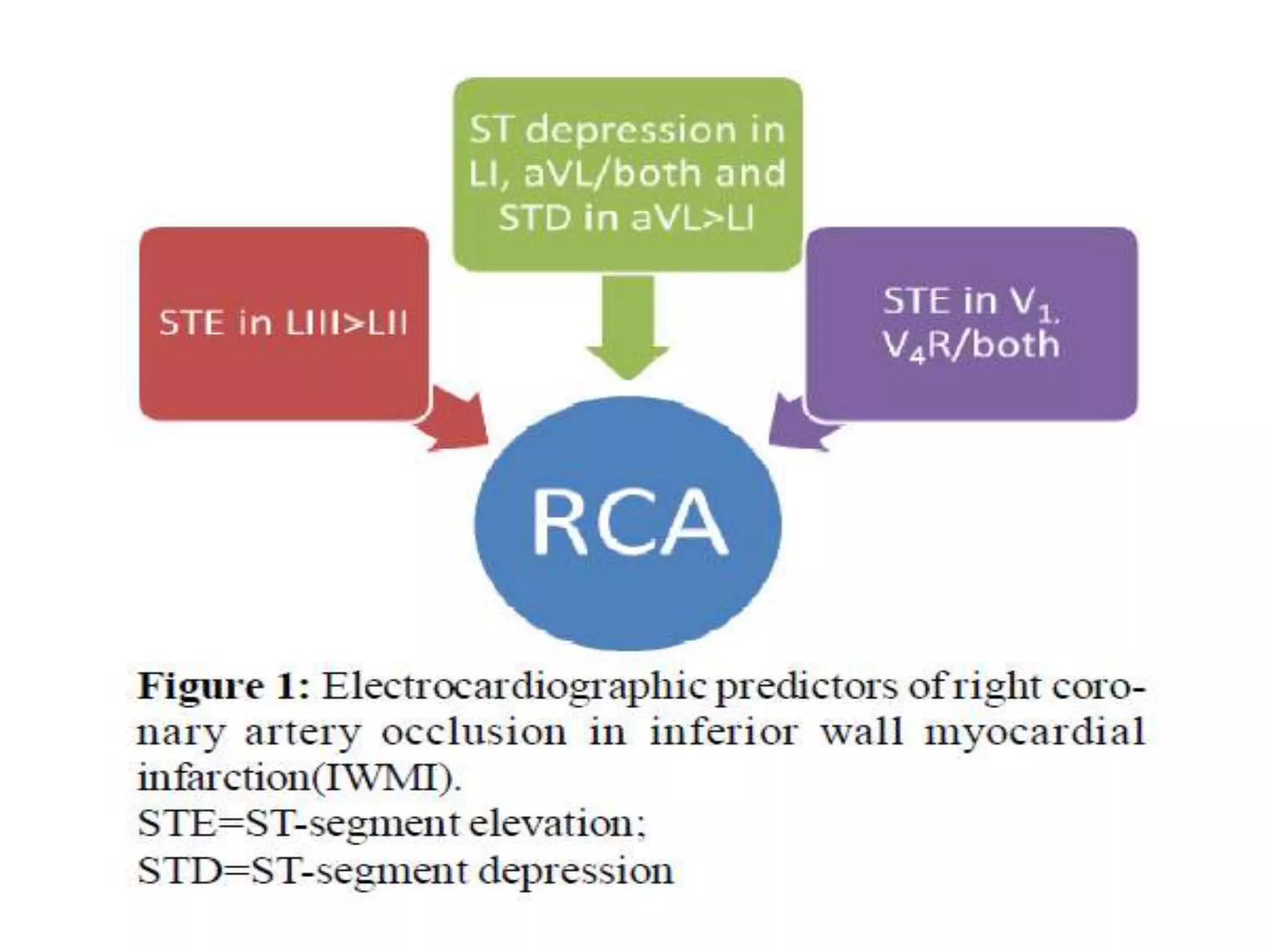
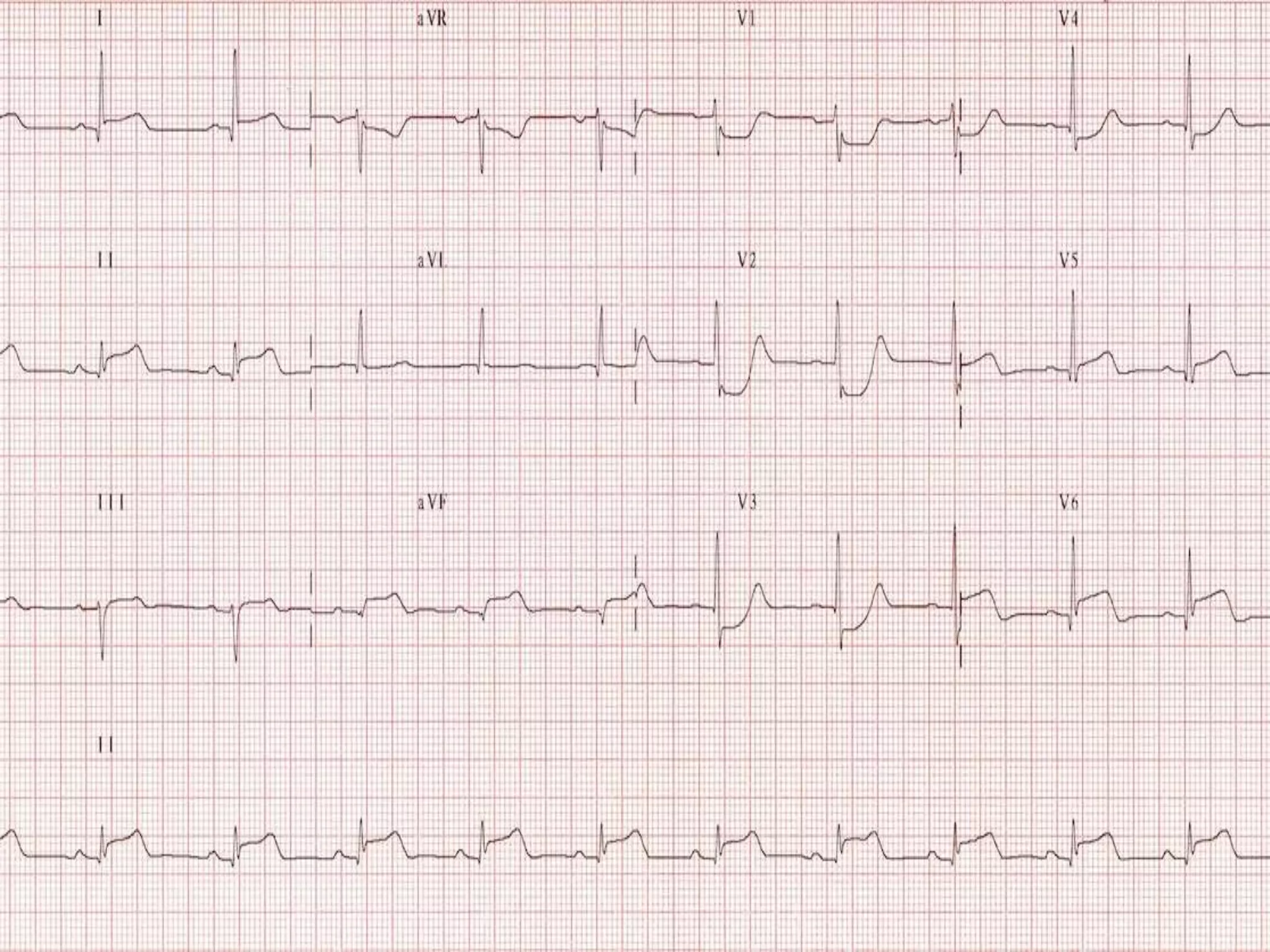
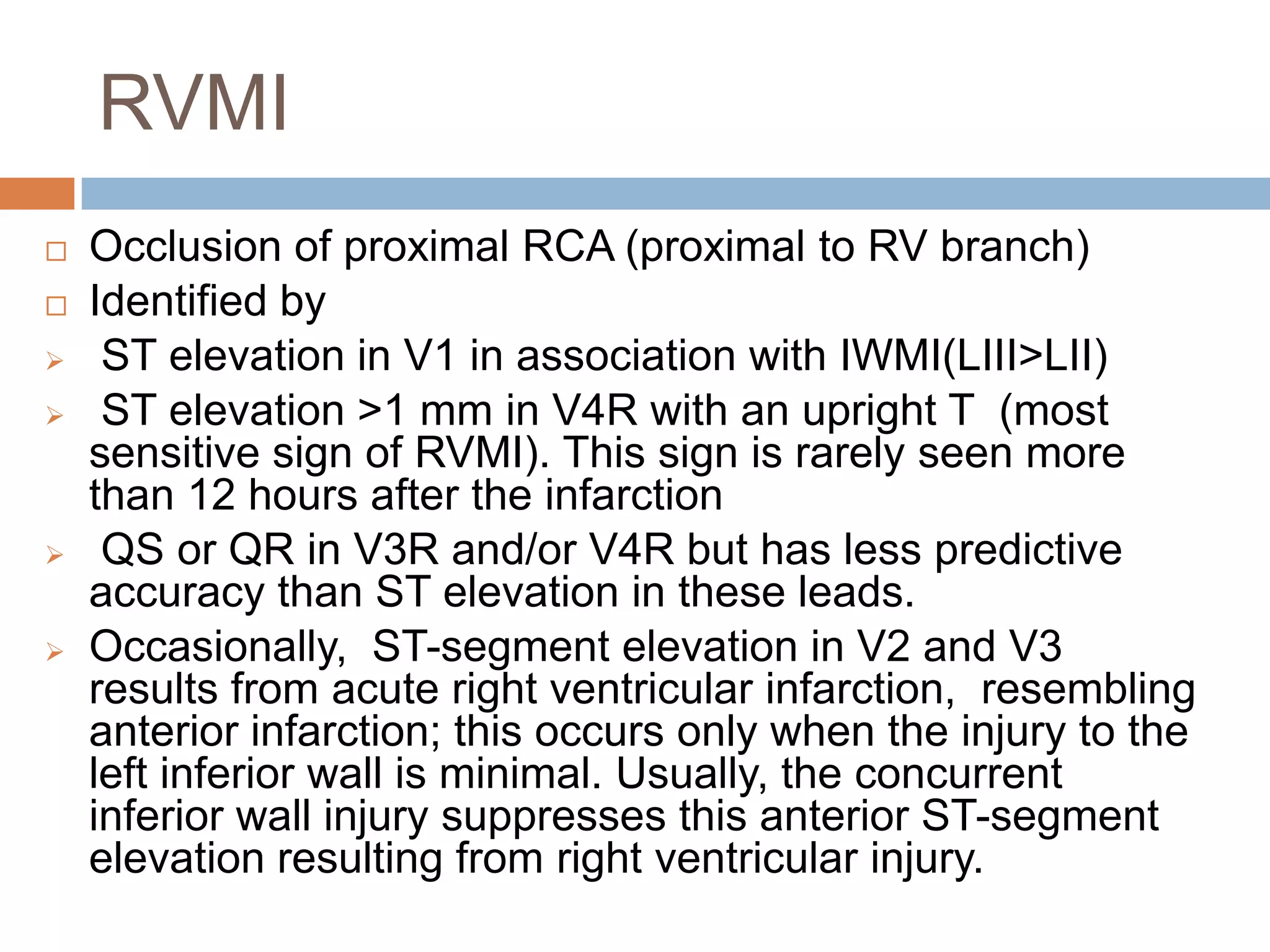
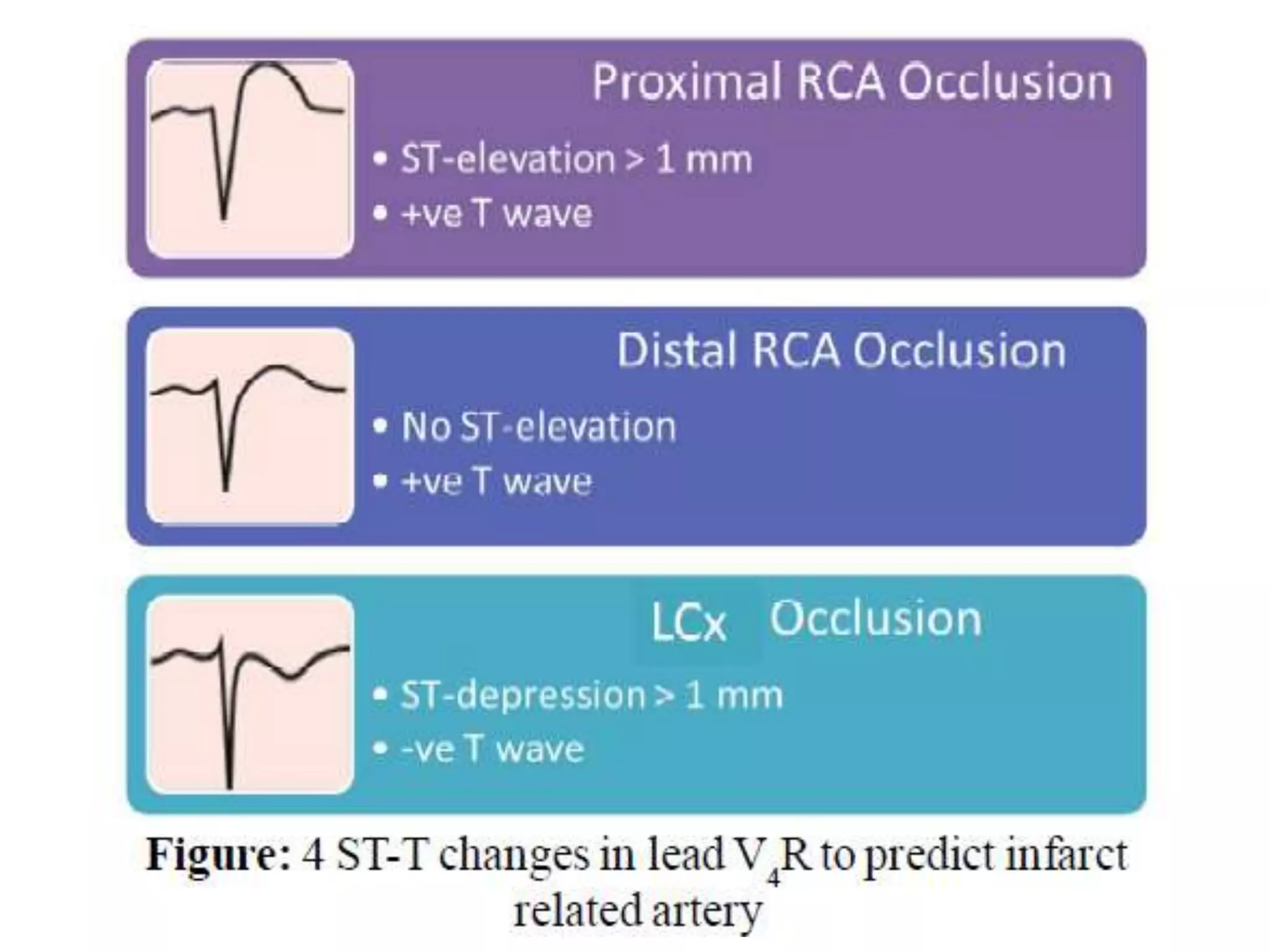
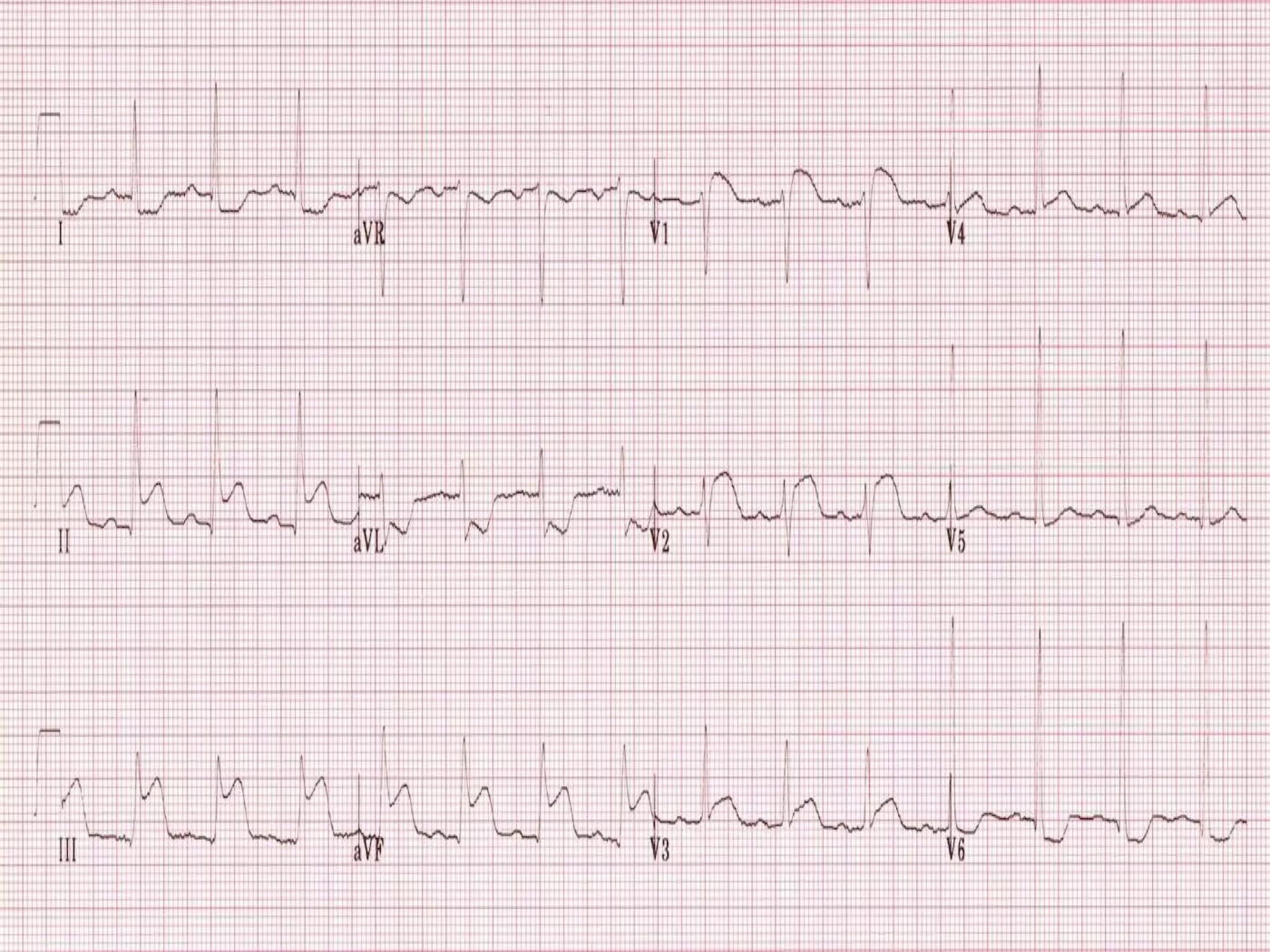
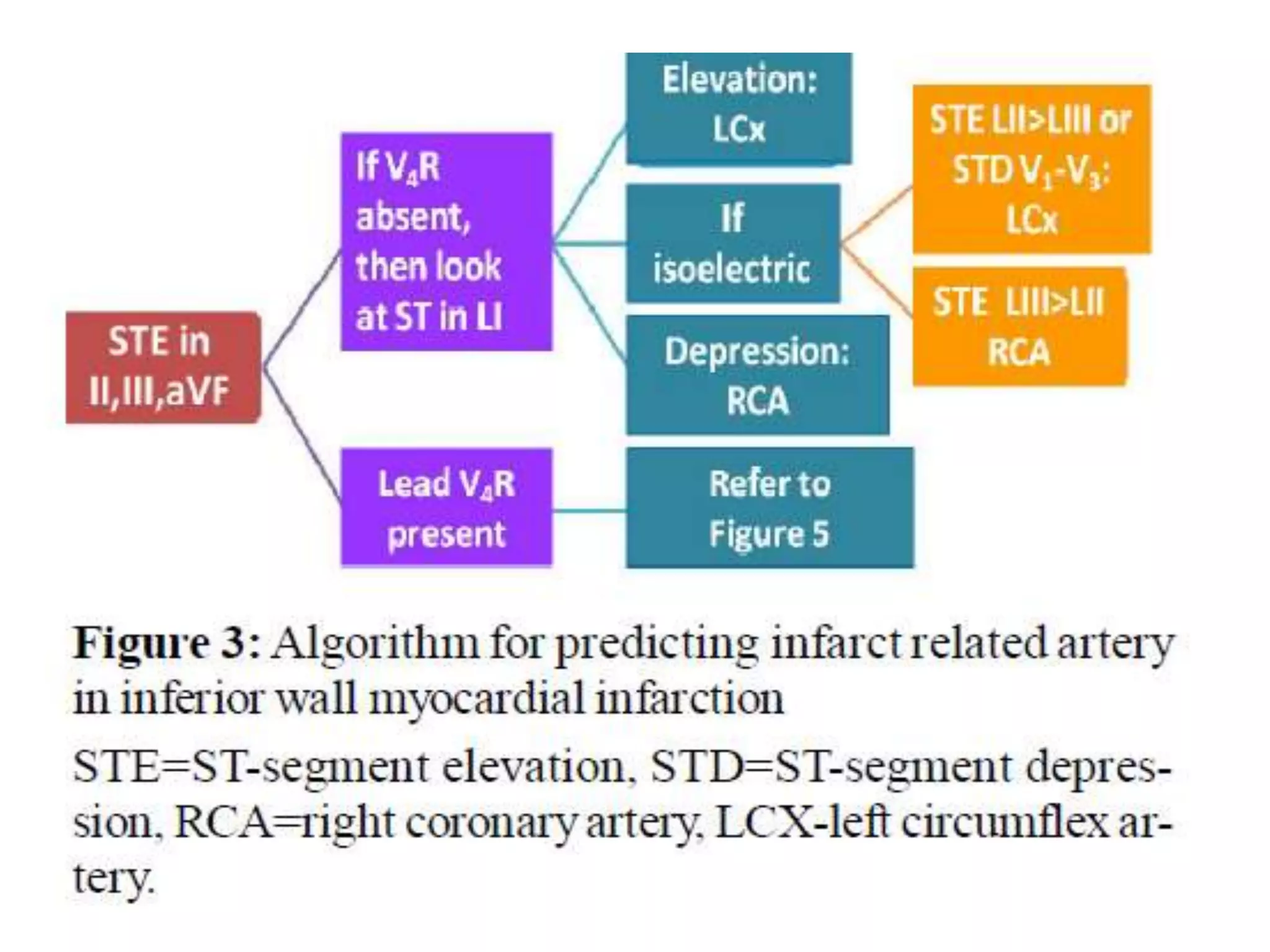
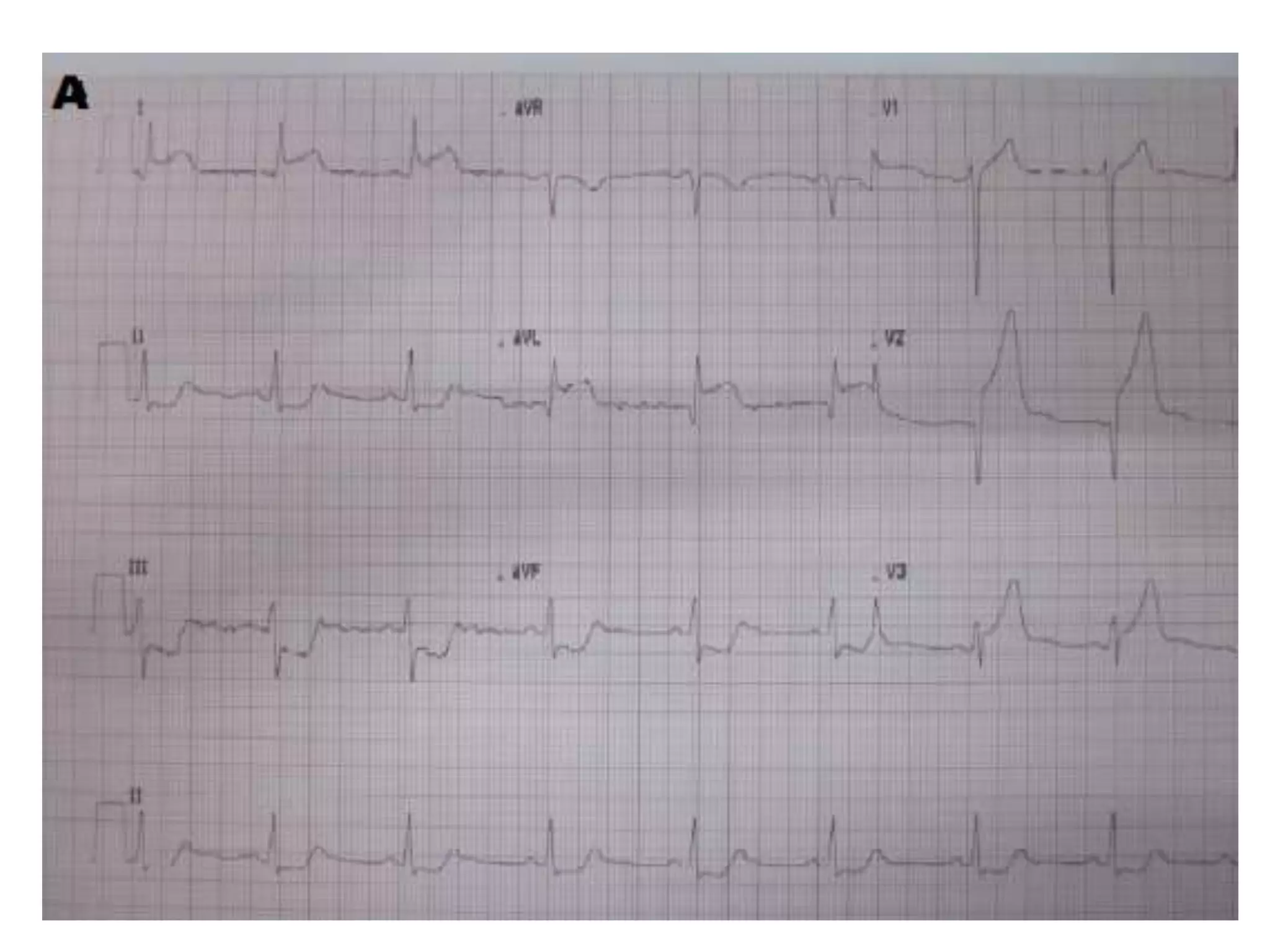
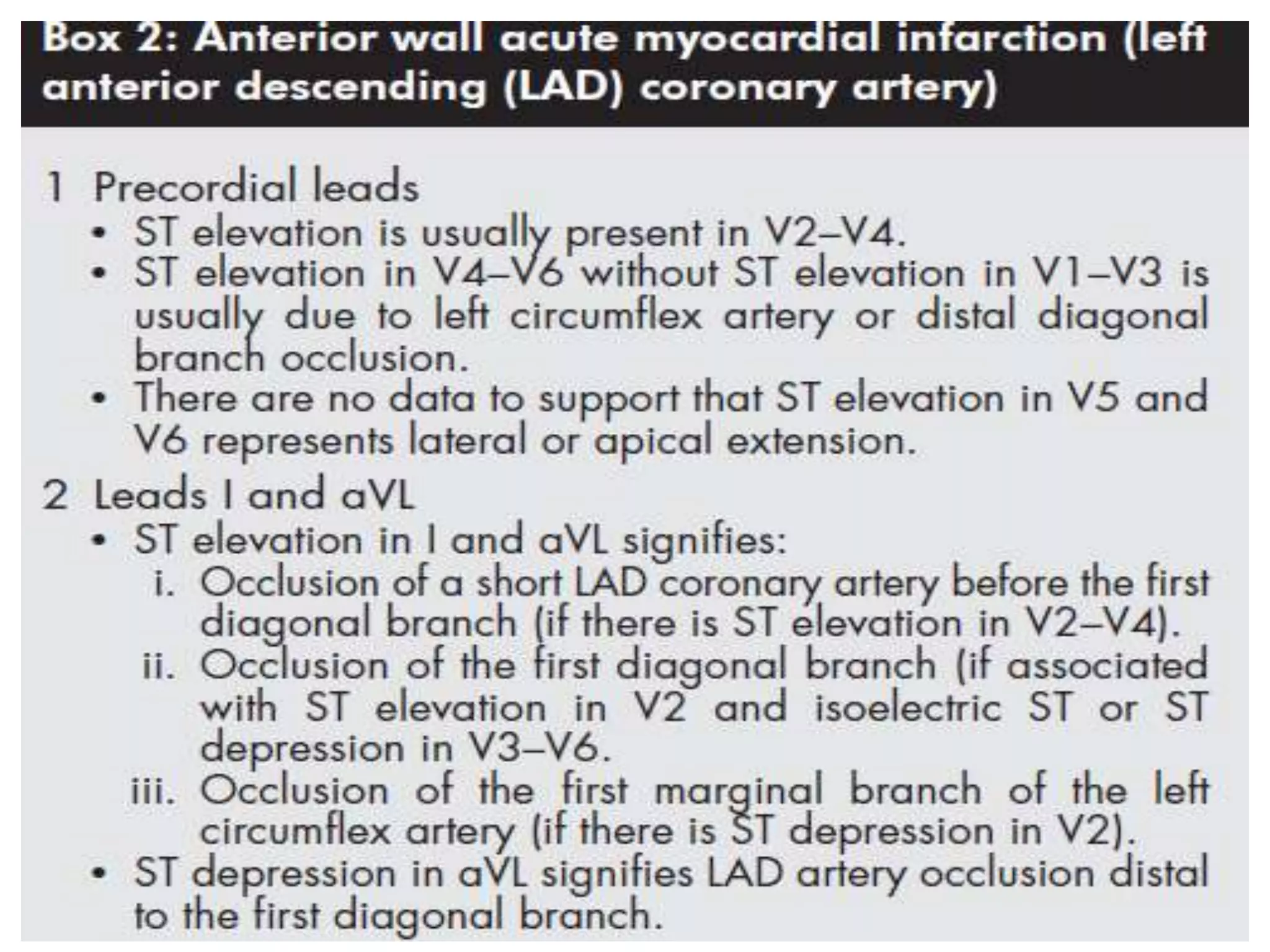
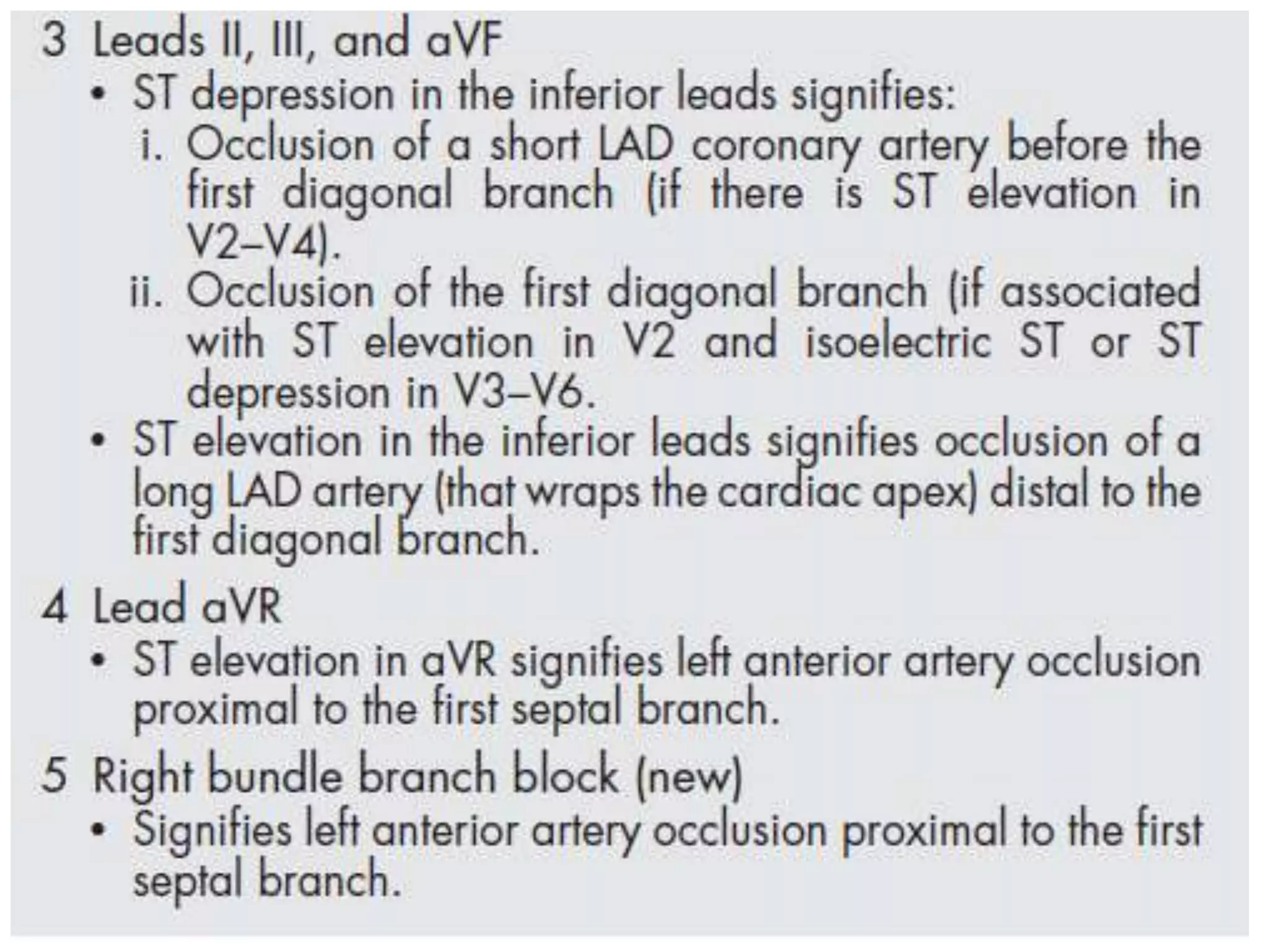
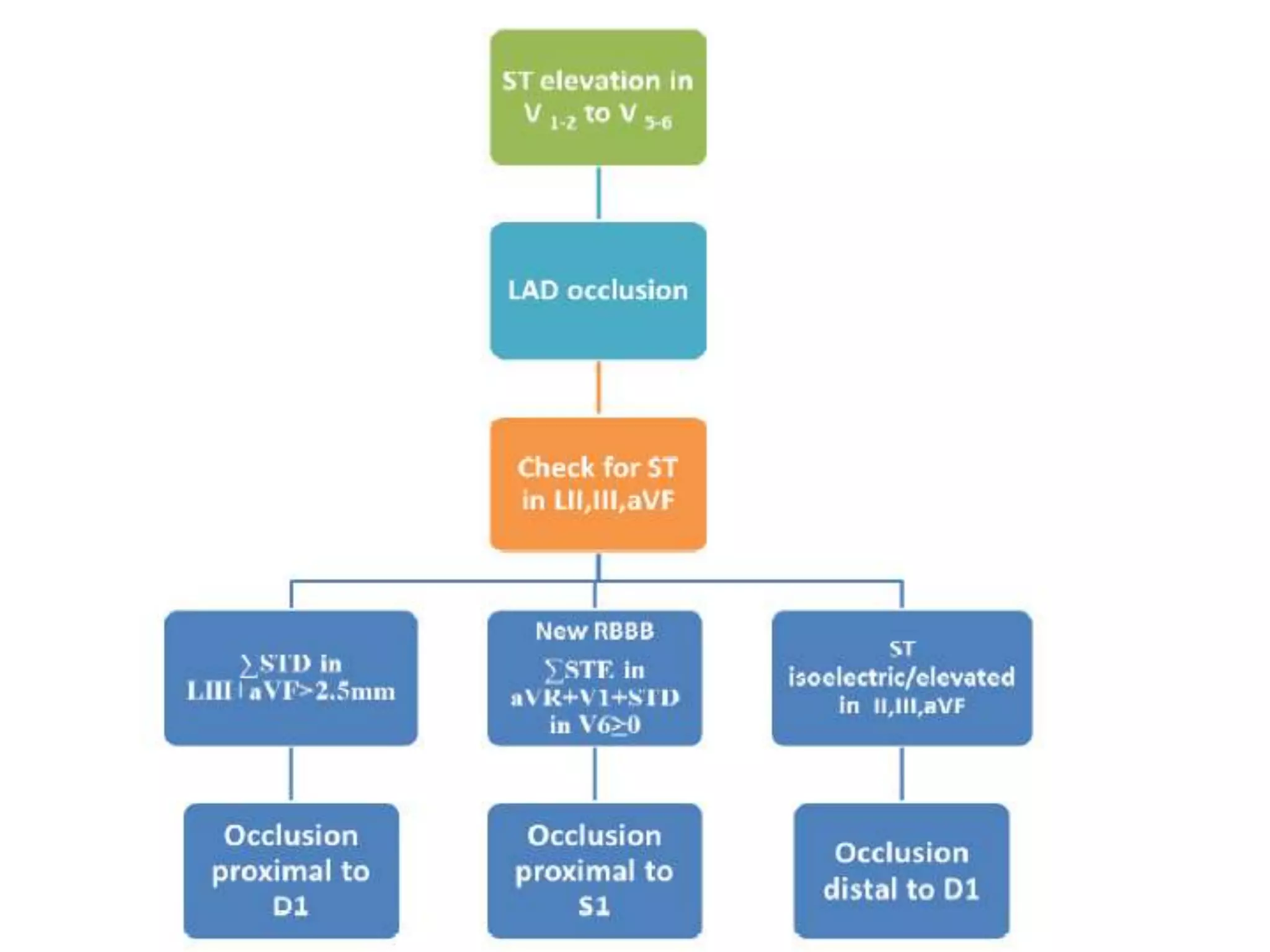


The document discusses coronary artery anatomy and ECG localization of the culprit vessel during acute myocardial infarction. It describes the typical blood supply and branches of the right coronary artery, left main coronary artery, left anterior descending artery, and left circumflex artery. It then covers how the ECG can be used to localize whether the right coronary artery, left circumflex artery, or other vessels are responsible for an acute MI based on the leads showing ST elevation and depression. Factors such as the ratio of ST changes in different leads help indicate whether proximal or distal vessels are involved.





























































































