Downloaded 856 times
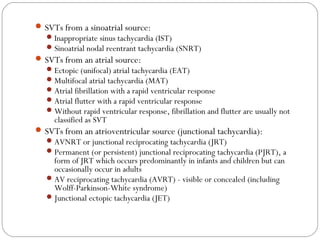
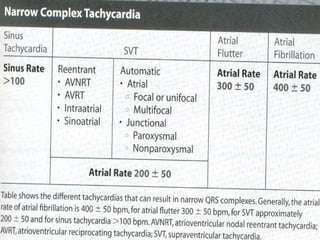
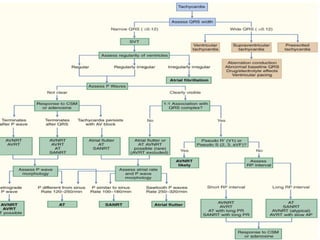
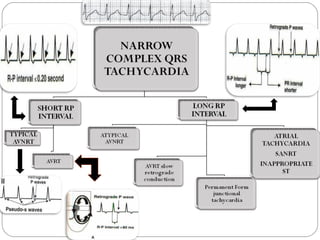


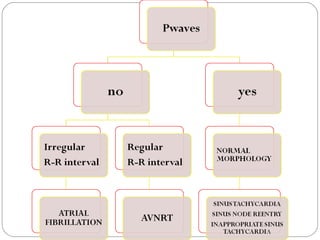
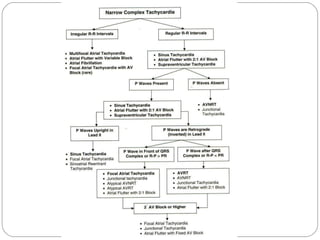
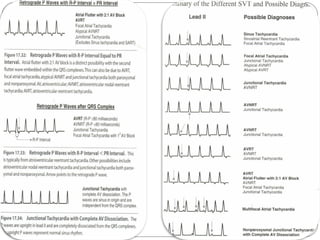
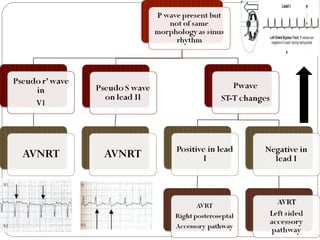

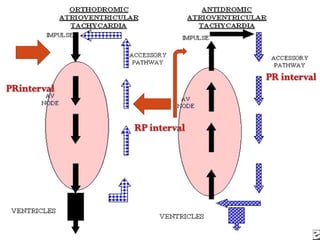
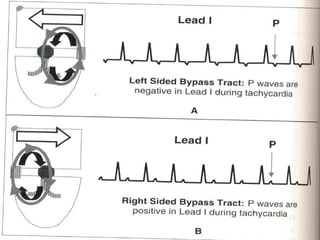
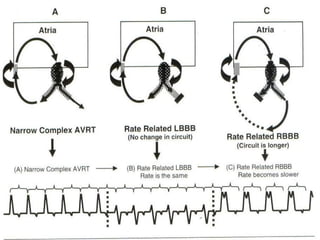

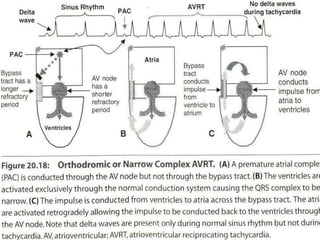
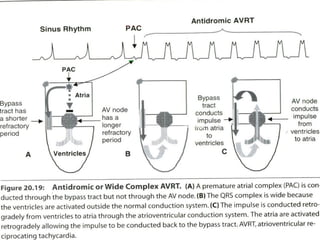
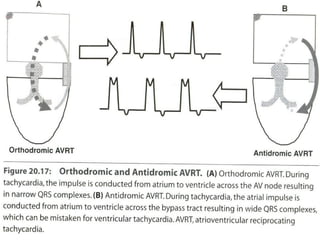

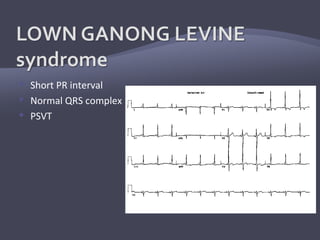


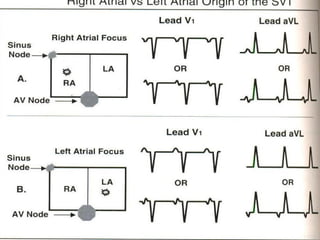

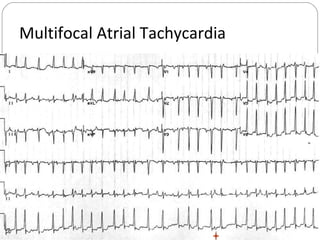


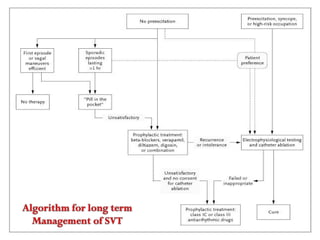
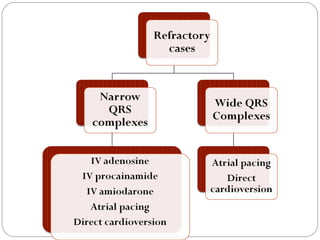

The document discusses various types of supraventricular tachycardia (SVT), including those originating from the sinoatrial, atrial, and atrioventricular sources, along with their ECG characteristics. Specific SVT types such as inappropriate sinus tachycardia, atrial fibrillation, and atrial flutter are described in detail, along with mechanisms and abnormal findings on ECG. The importance of identifying precipitating factors and acute termination strategies for SVT is also emphasized.







































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



