Downloaded 76 times

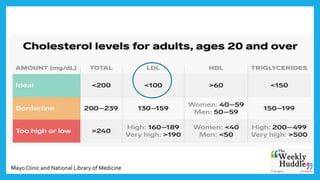
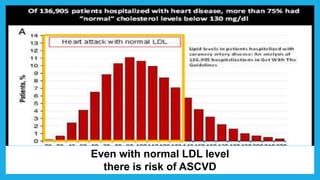
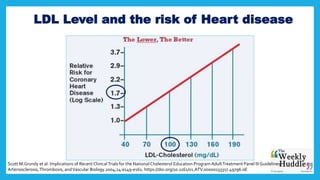
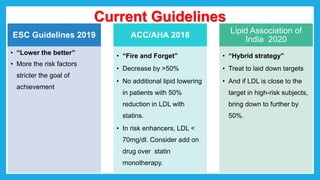
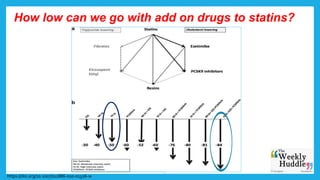
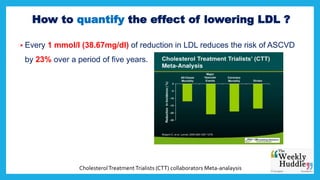
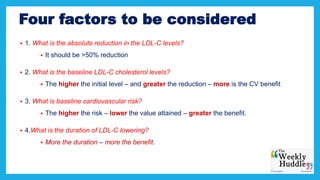
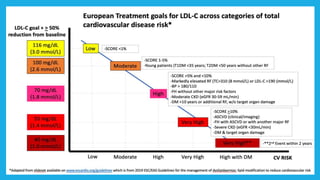
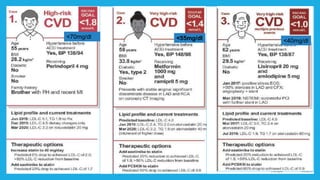
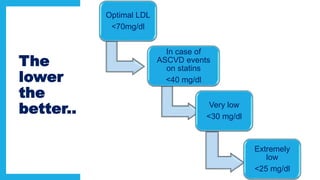
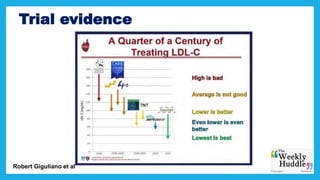
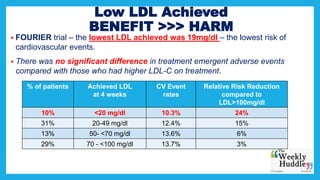


This document discusses guidelines for lowering LDL cholesterol levels to reduce cardiovascular risk. It notes that while normal LDL levels are considered low risk, even normal levels still carry some risk. Current guidelines recommend lowering LDL as much as possible, by at least 50%, with a target under 70 mg/dL or lower for high-risk patients. Clinical trials have shown lower LDL levels are associated with greater risk reduction, down to levels under 40 mg/dL, though very low levels below 25 mg/dL require more evidence. Potential safety risks of extremely low levels are also examined. The conclusion emphasizes the importance of early detection and management of dyslipidemia to prevent cardiovascular disease.























































































