Downloaded 163 times
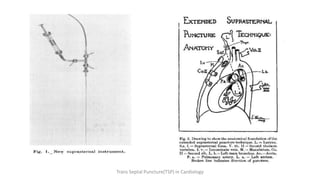
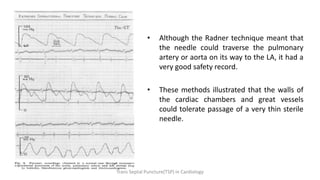
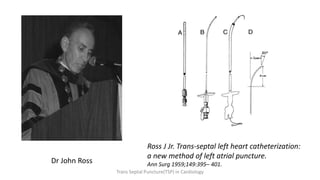



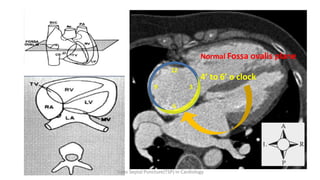
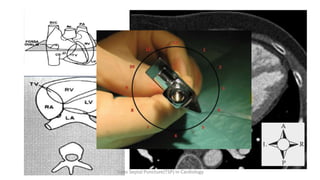
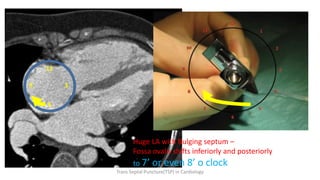
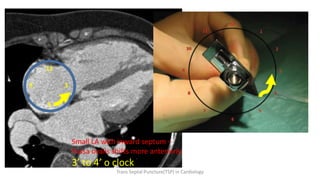
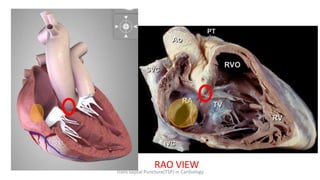
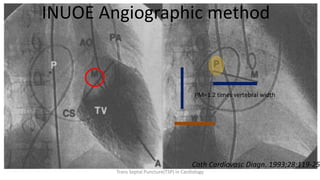
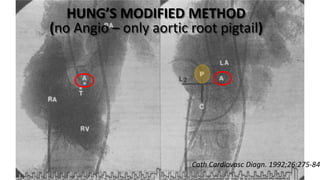
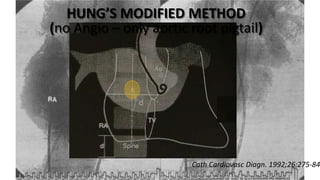

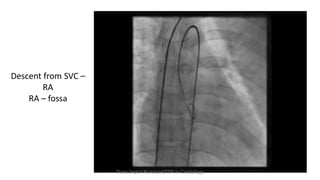
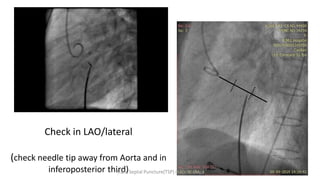


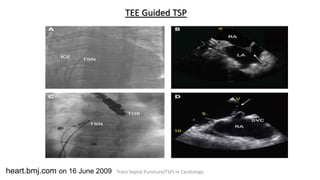
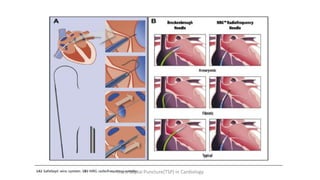
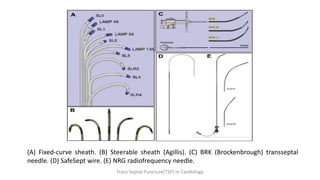

Trans septal puncture (TSP) is a technique in cardiology developed to access the left atrium (LA) directly through the intra-atrial septum, facilitating various procedures like left heart catheterization and catheter ablation of atrial fibrillation. Over the years, the TSP technique has evolved, with significant contributions from various clinicians, ensuring safety and effectiveness through improved needle and catheter designs. The procedure has specific indications, contraindications, and procedural steps that have made it a routine skill for modern cardiac electrophysiologists.















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


