Downloaded 373 times
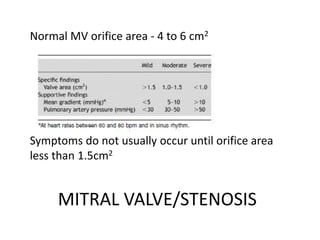
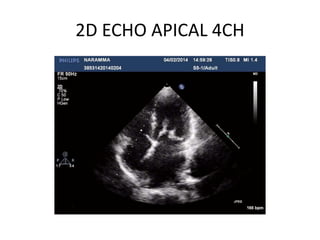
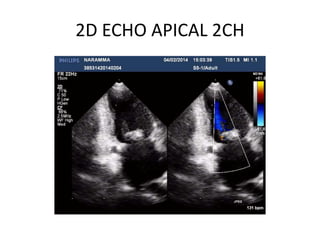
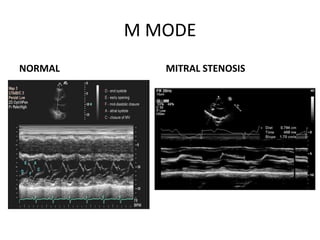
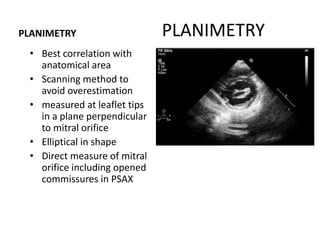
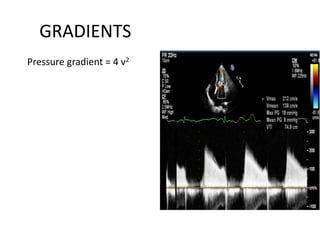
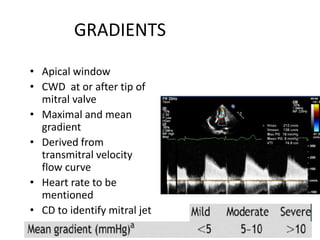
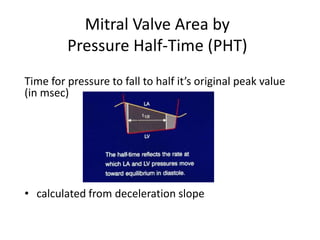
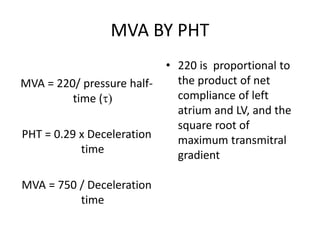
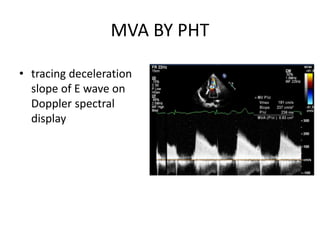
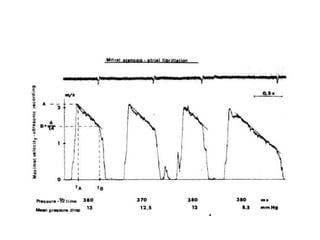

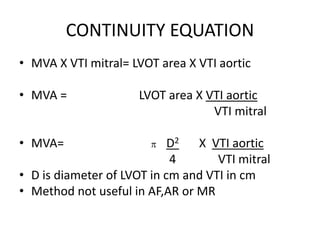
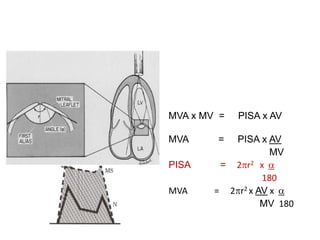

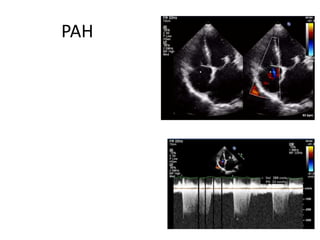
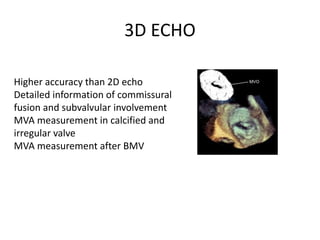


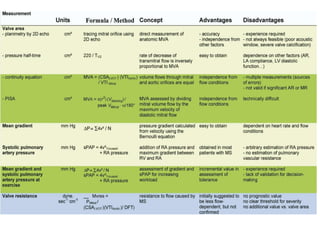
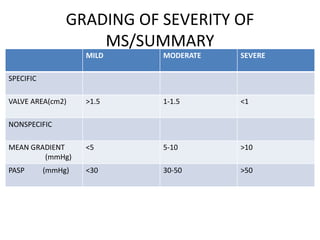


Mitral stenosis can be evaluated using echocardiography. Key findings include measuring the mitral valve area using planimetry, pressure half-time, and continuity equation methods. Pressure gradients and pulmonary artery systolic pressure can also assess severity. Mild mitral stenosis is defined as a mitral valve area greater than 1.5 cm2, moderate as 1-1.5 cm2, and severe as less than 1 cm2. Stress echocardiography may reveal symptoms in borderline cases by monitoring pressures with exercise.














































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








