Downloaded 200 times
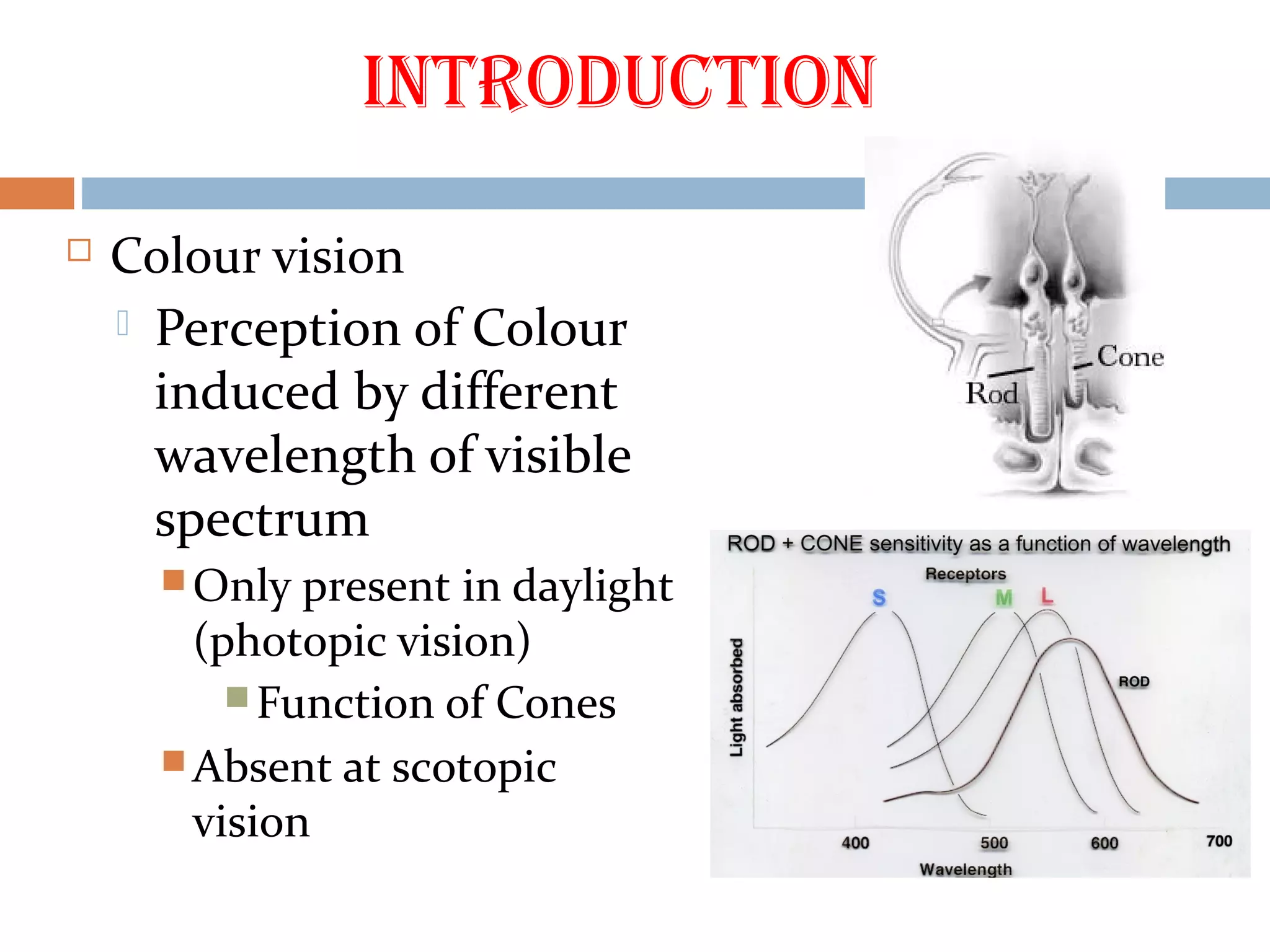
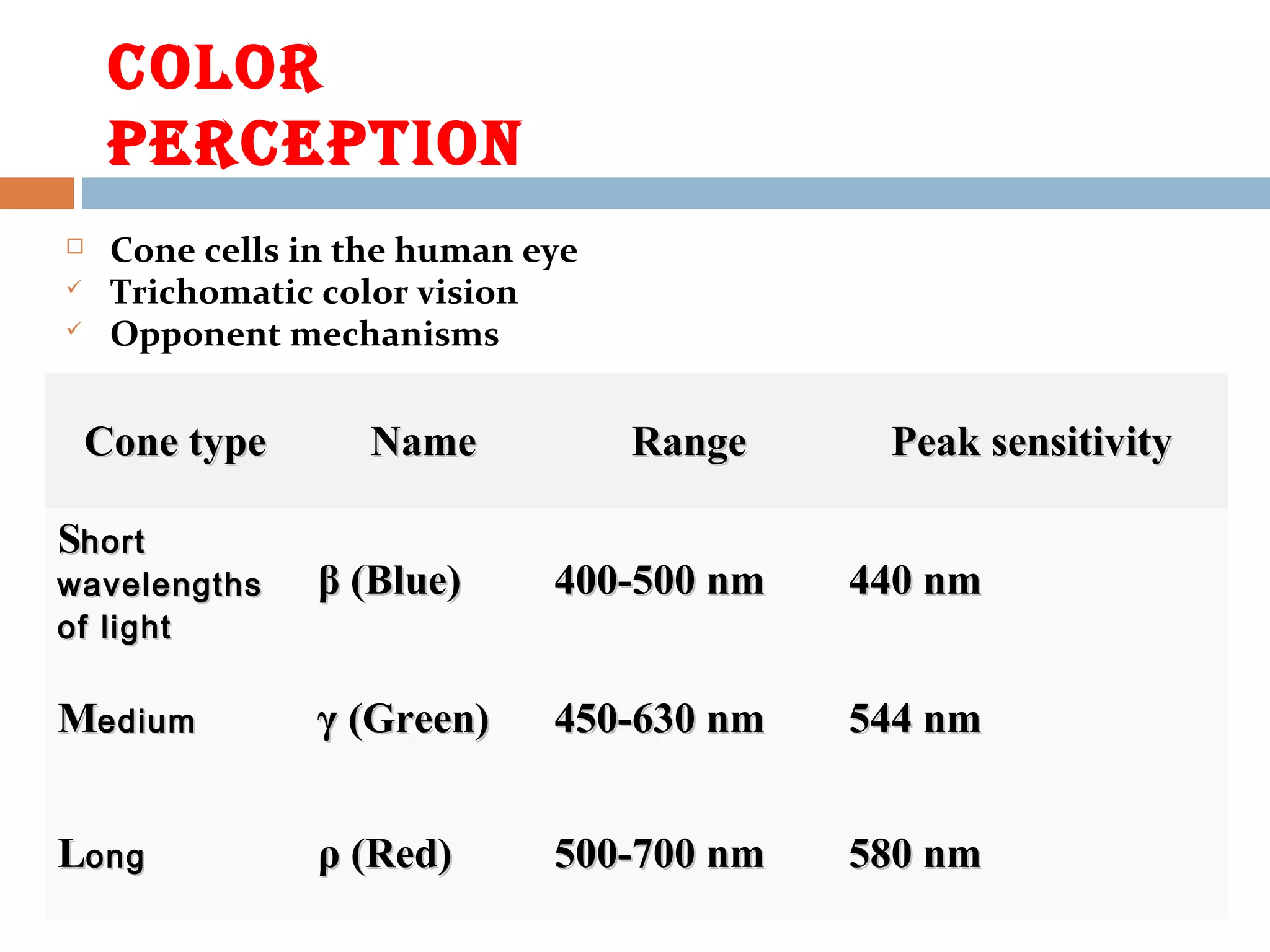
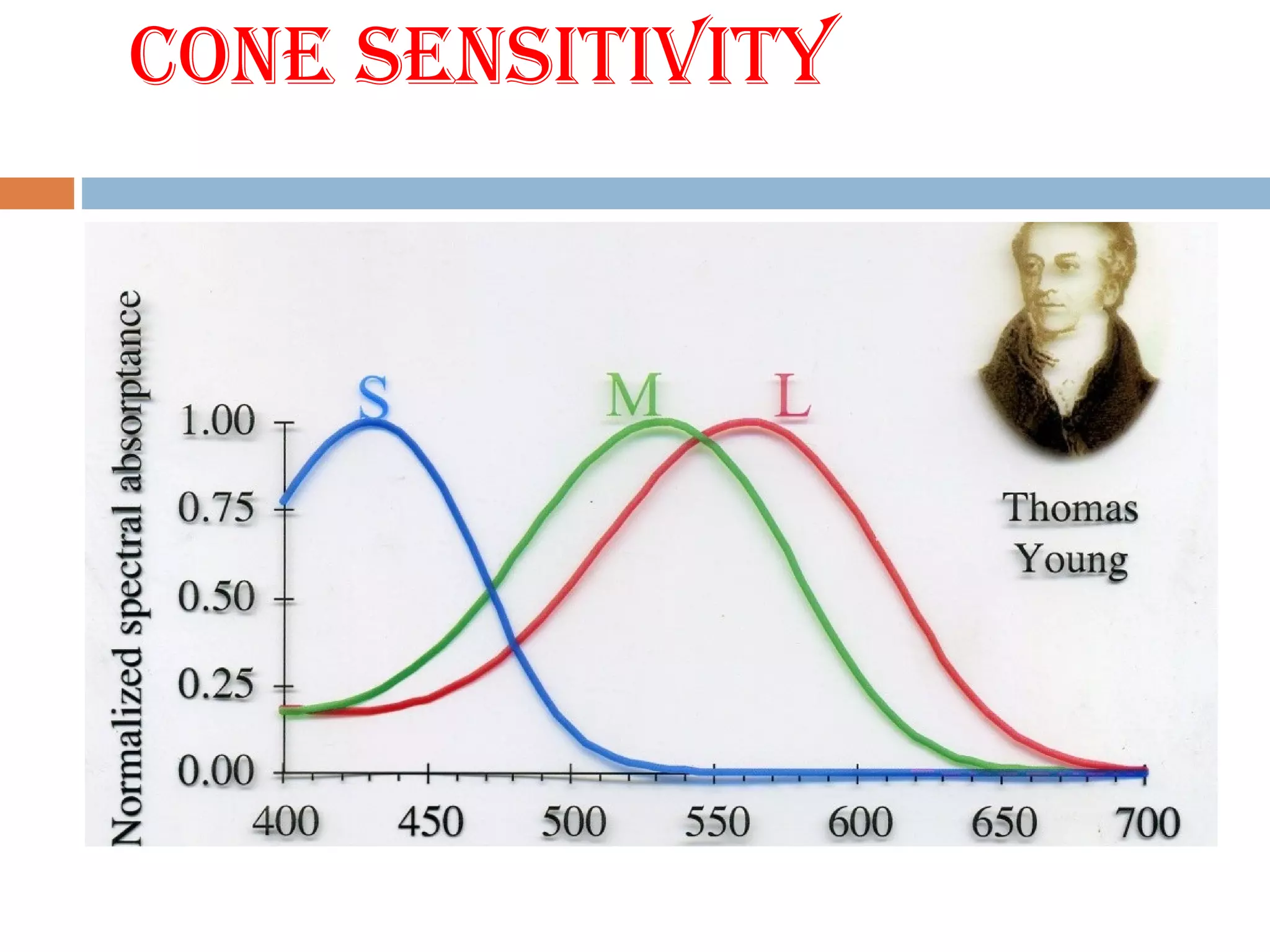
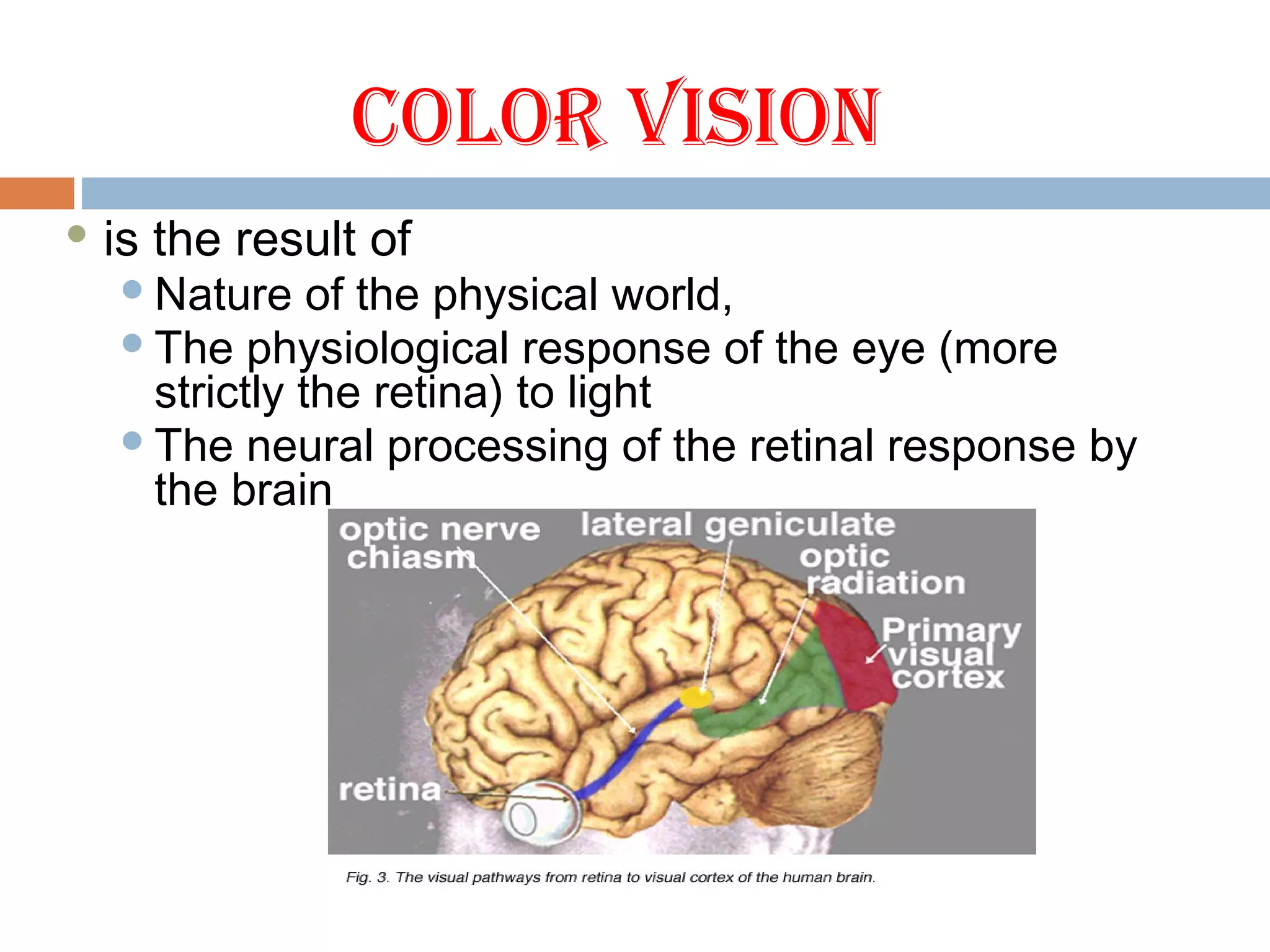
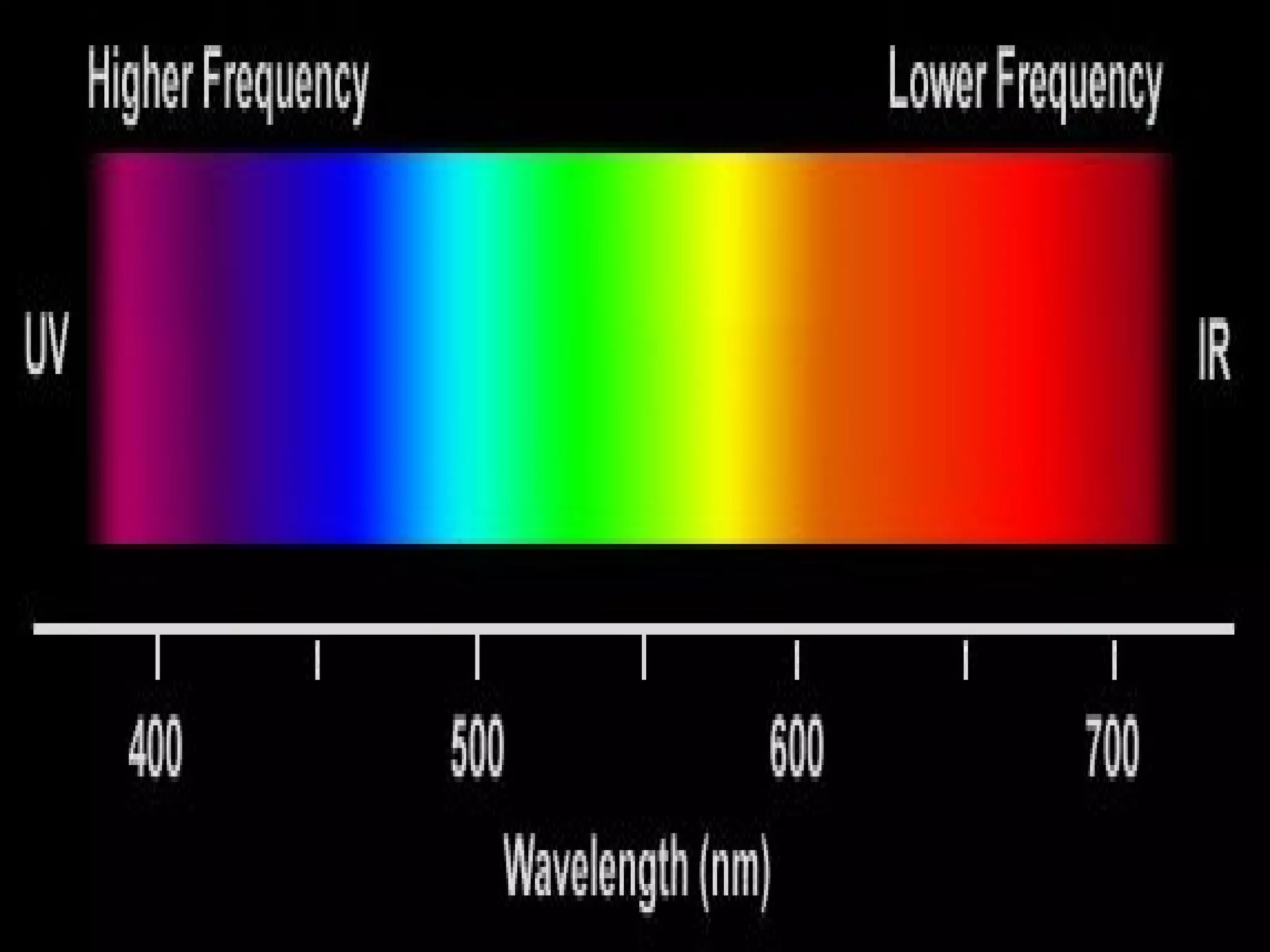
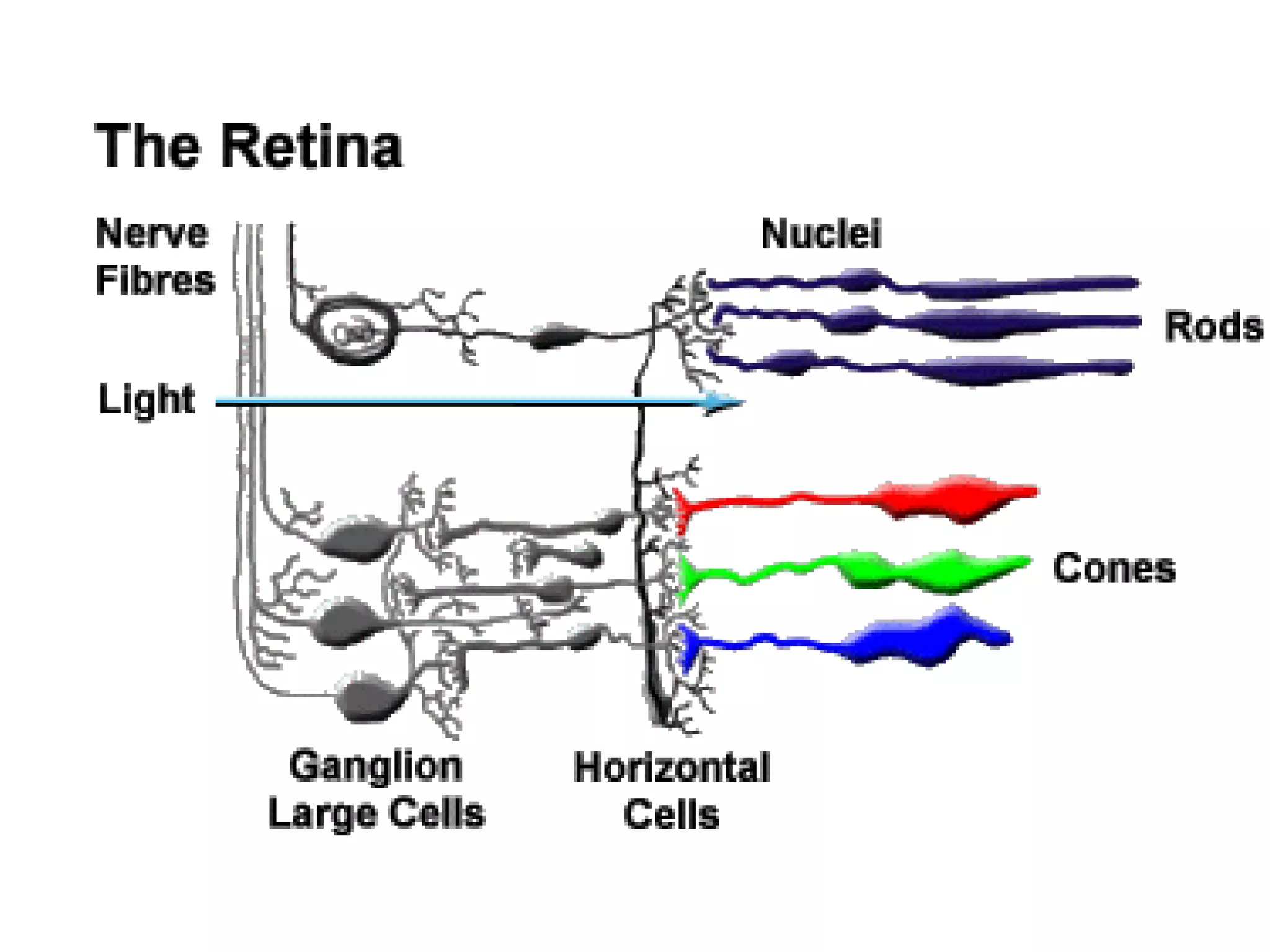


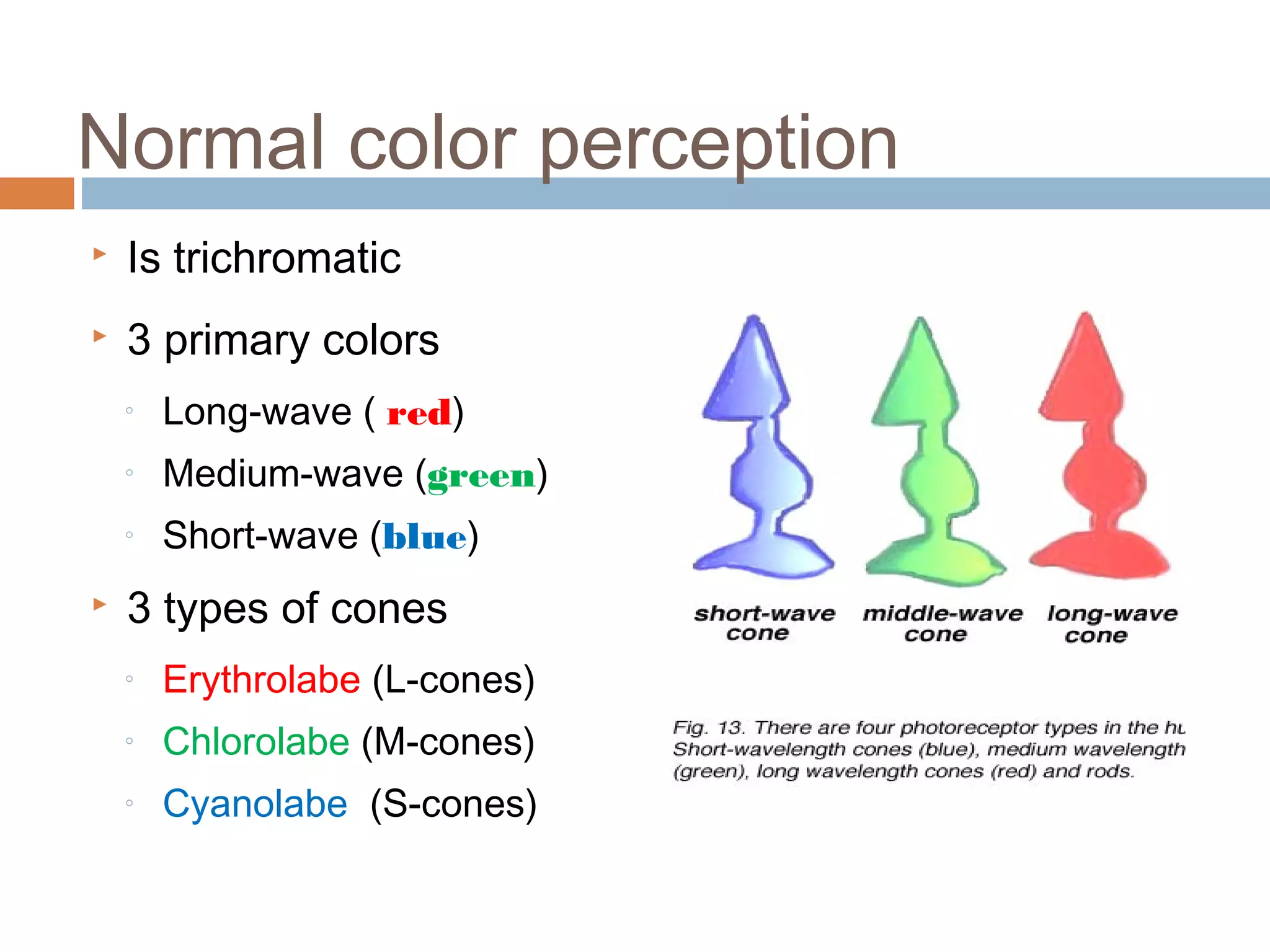
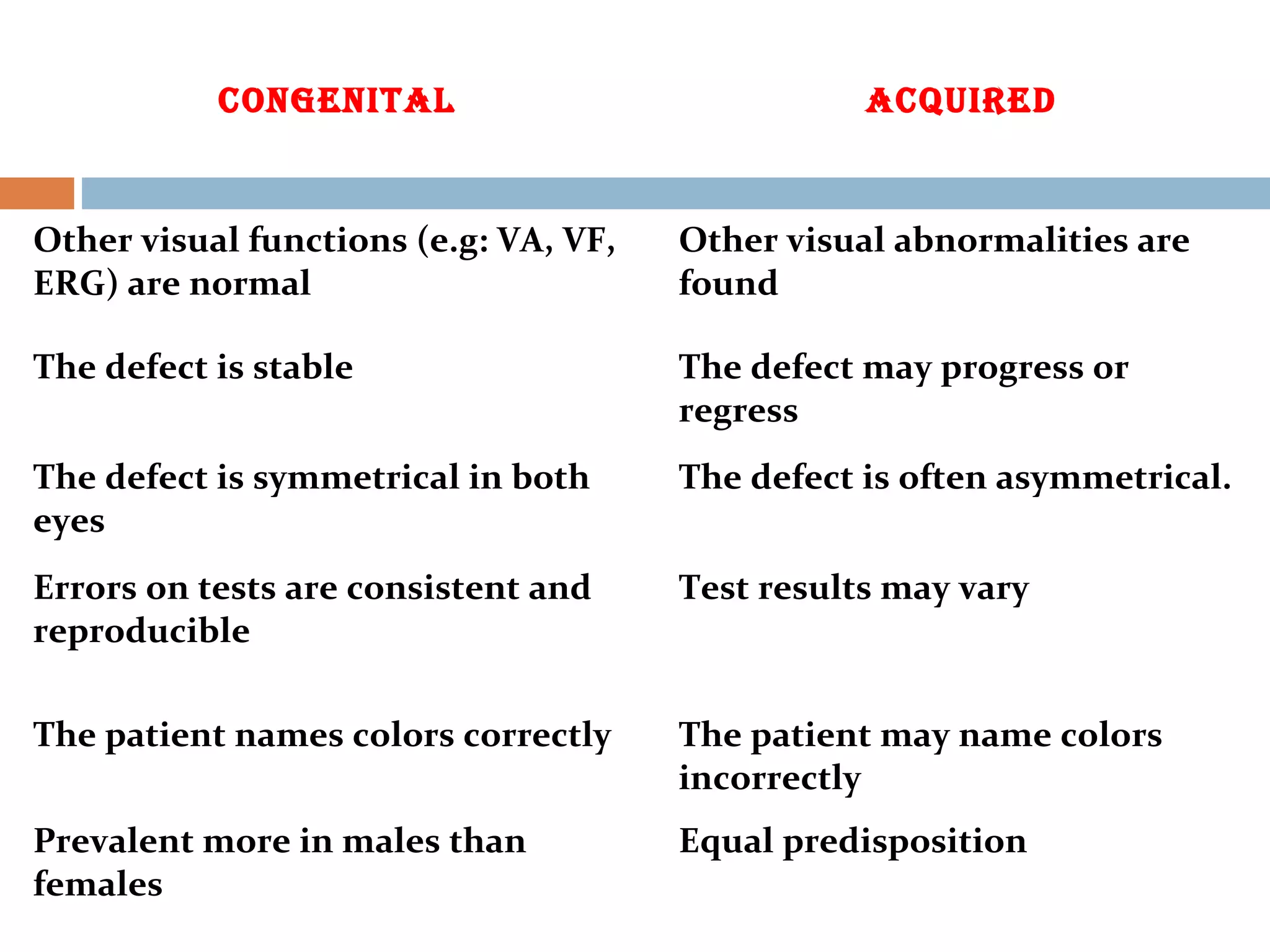

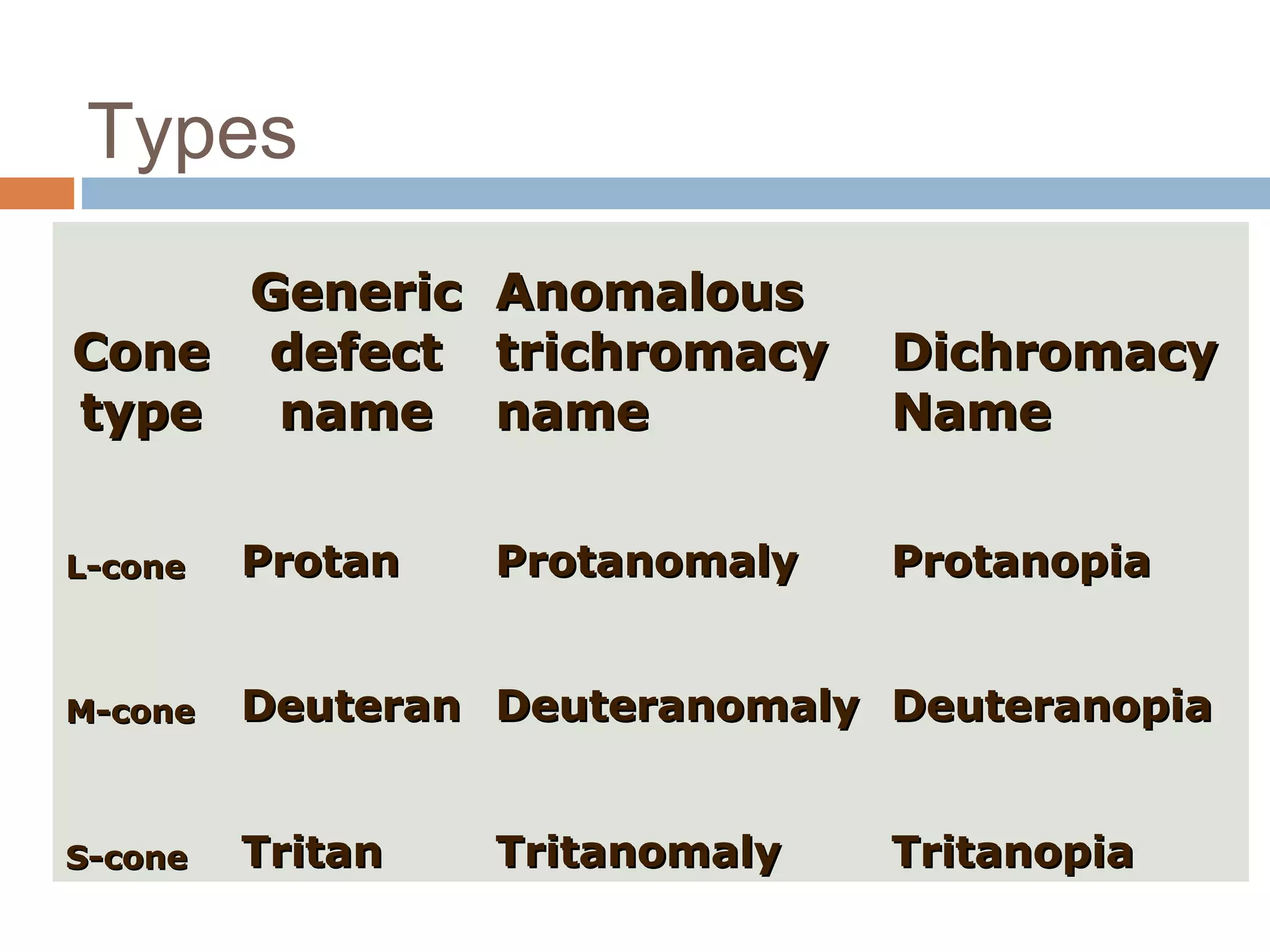
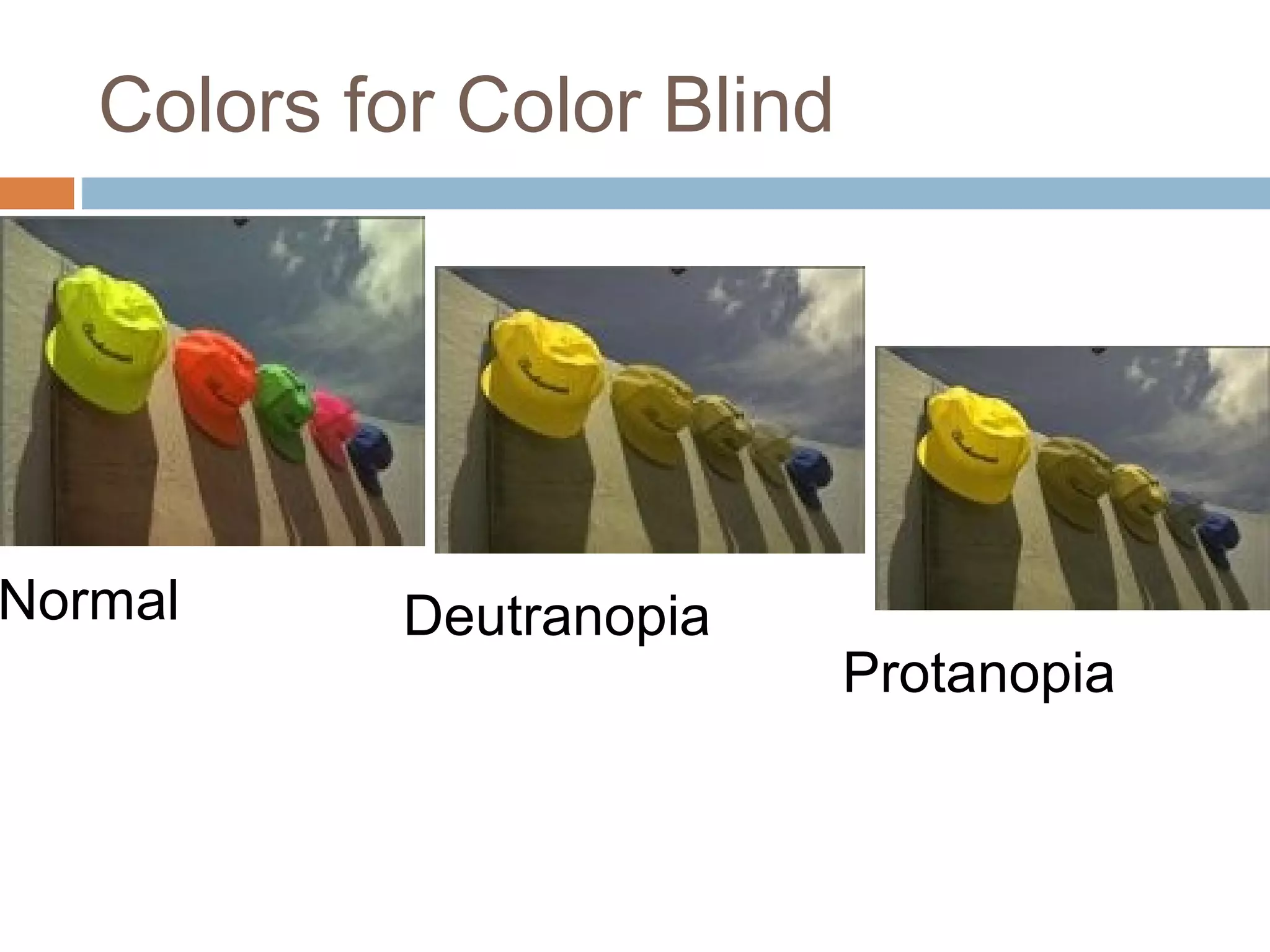
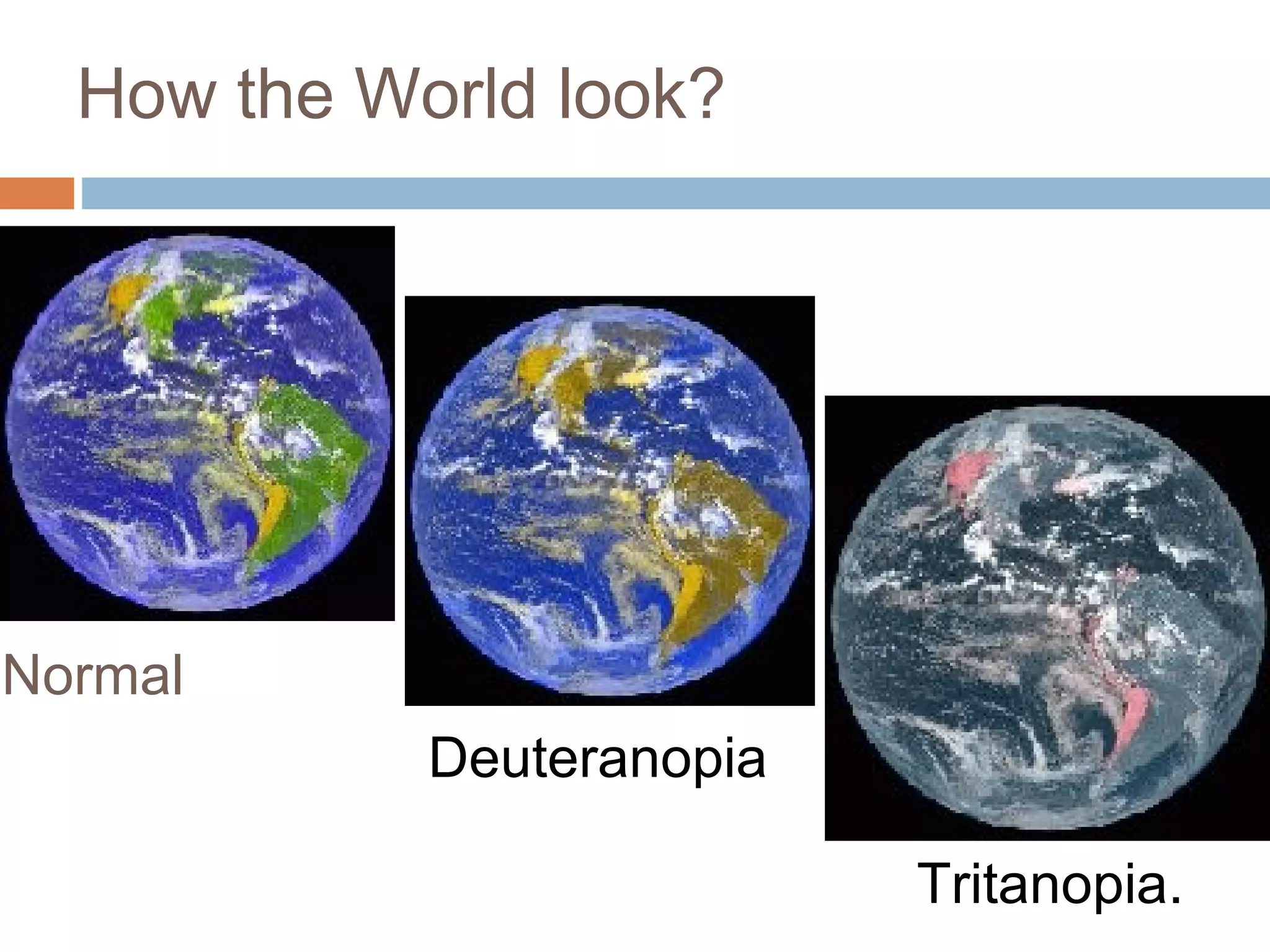




The document provides an in-depth overview of color vision, including definitions, physiological processes, types of color vision defects, and theories explaining color perception such as the trichromatic and opponent color theories. It discusses the role of cone cells in the eye, genetic factors contributing to color blindness, and the categorization of color vision deficiencies such as congenital and acquired types. Additionally, it highlights the prevalence of color vision defects and their inheritance patterns, emphasizing the importance of genetic factors in understanding these conditions.













































































![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)









