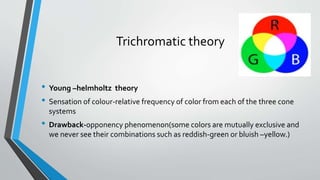
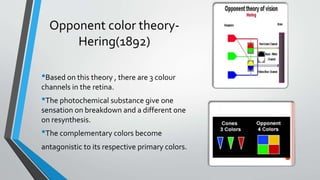
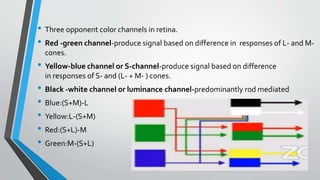
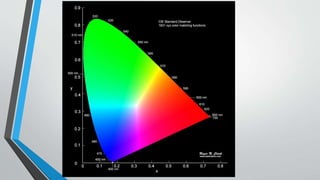
The document discusses color vision, including the physiological and neurological mechanisms behind color perception, as well as types of color vision deficiencies such as congenital and acquired color blindness. It details the role of cone photoreceptors and various theories explaining color sensation, including trichromatic and opponent color theories. Additionally, it covers color vision testing methods and classification systems like the CIE and Munsell color systems, highlighting approaches for assessing and diagnosing color deficiencies.