Downloaded 136 times
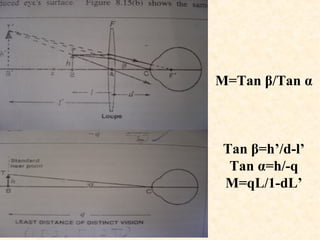
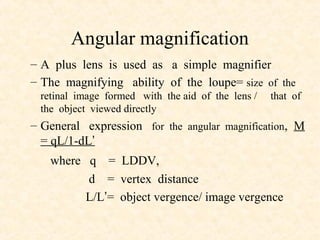


The document explores various types of magnification used in ocular examinations, including linear and angular magnification, as well as nominal, maximum, and iso-accommodative magnification. It discusses concepts such as spectacle magnification, relative spectacle magnification, and their clinical significance, particularly in assessing conditions affecting vision. Additionally, it details the uses of different optical instruments including microscopes and telescopes, highlighting how they magnify images for clinical or educational purposes.