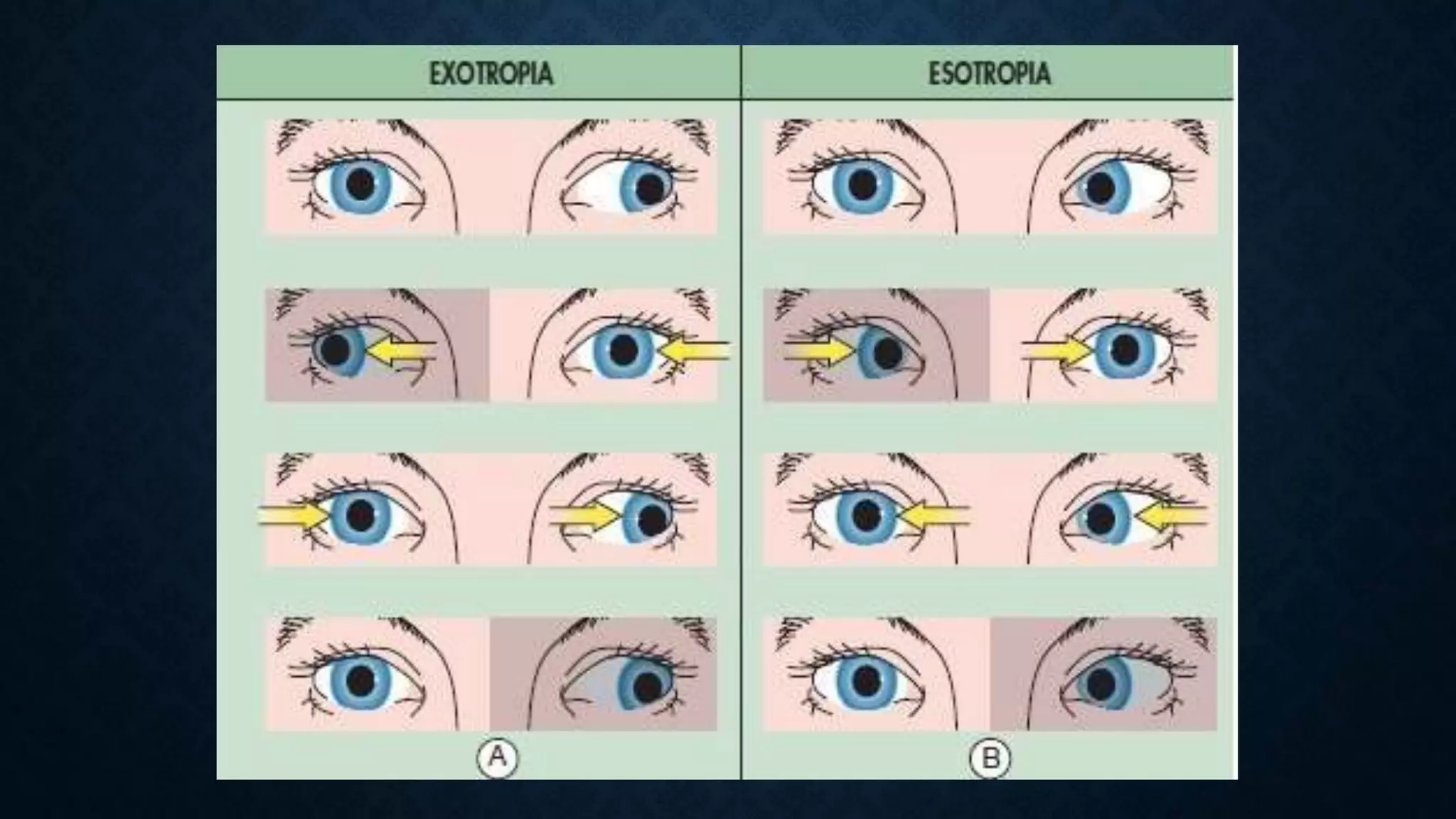
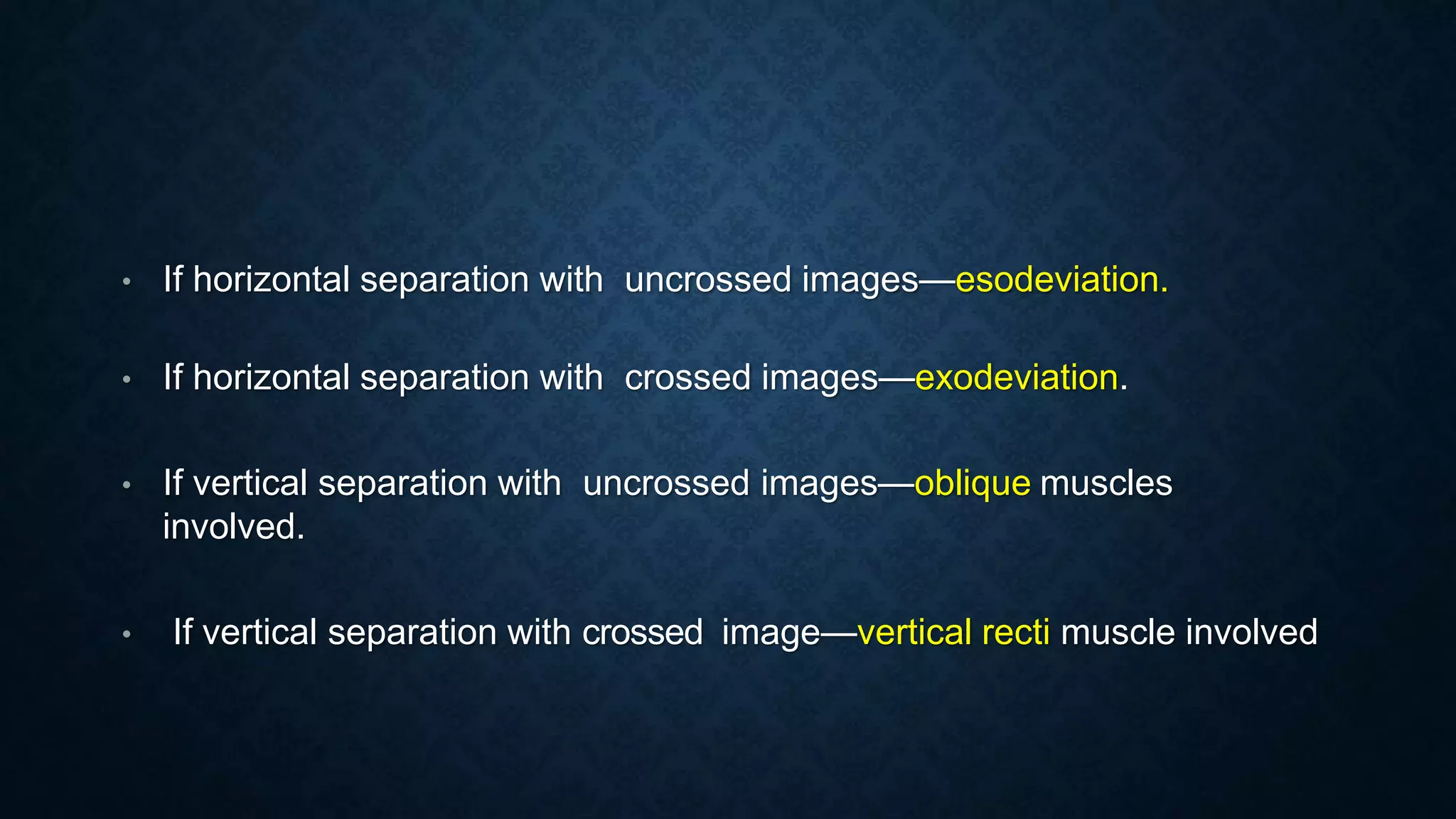
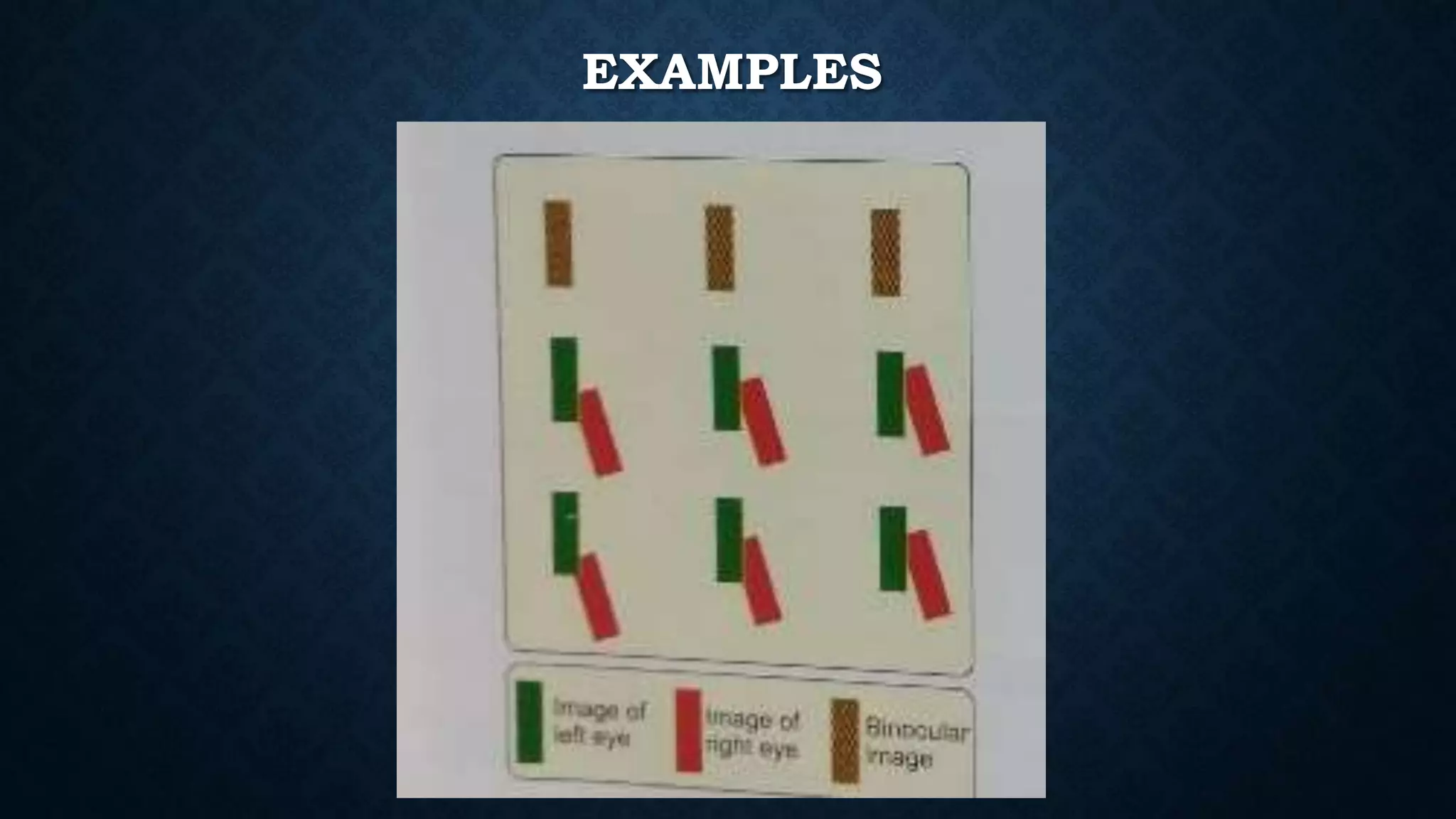
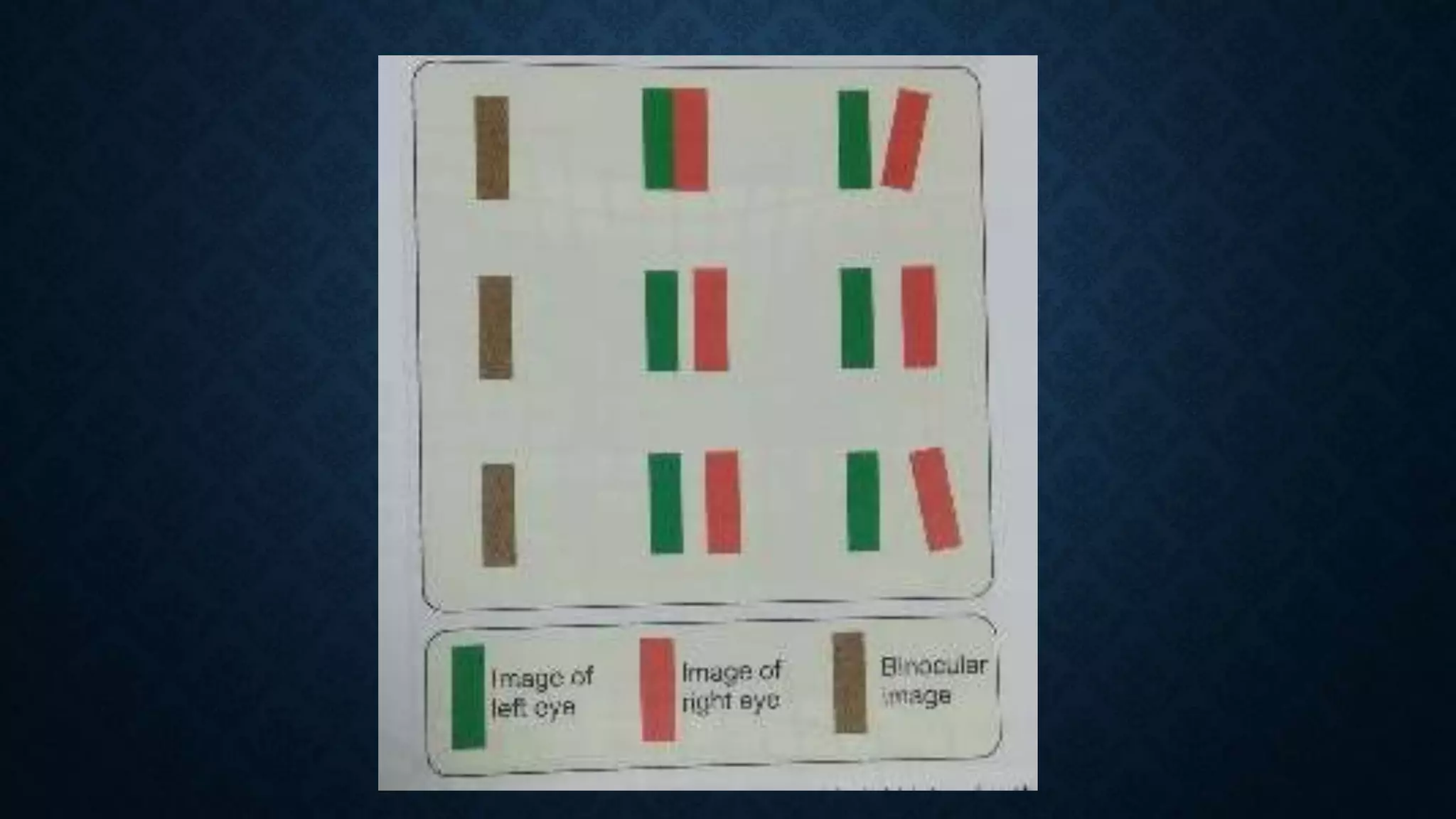
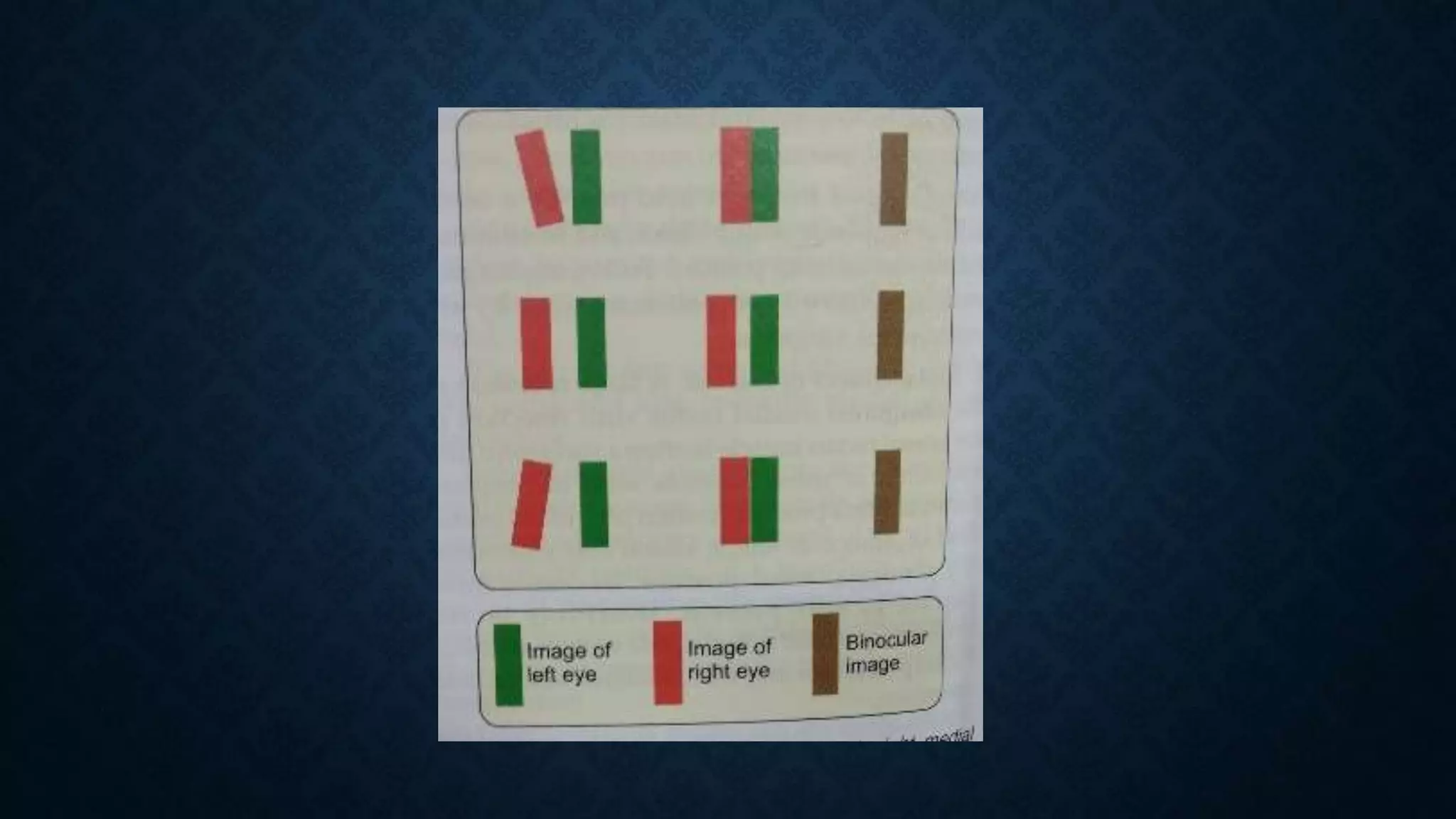
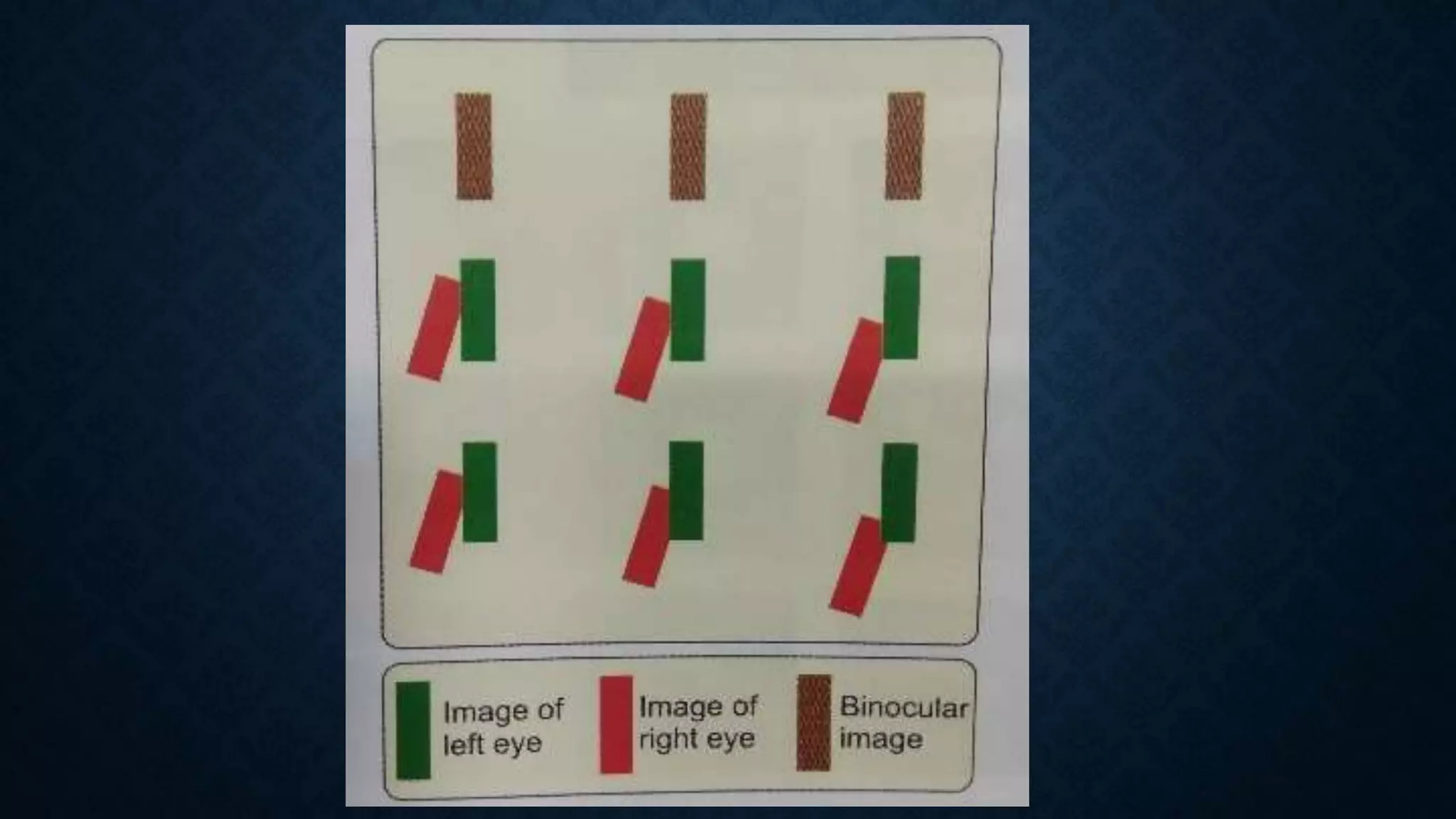
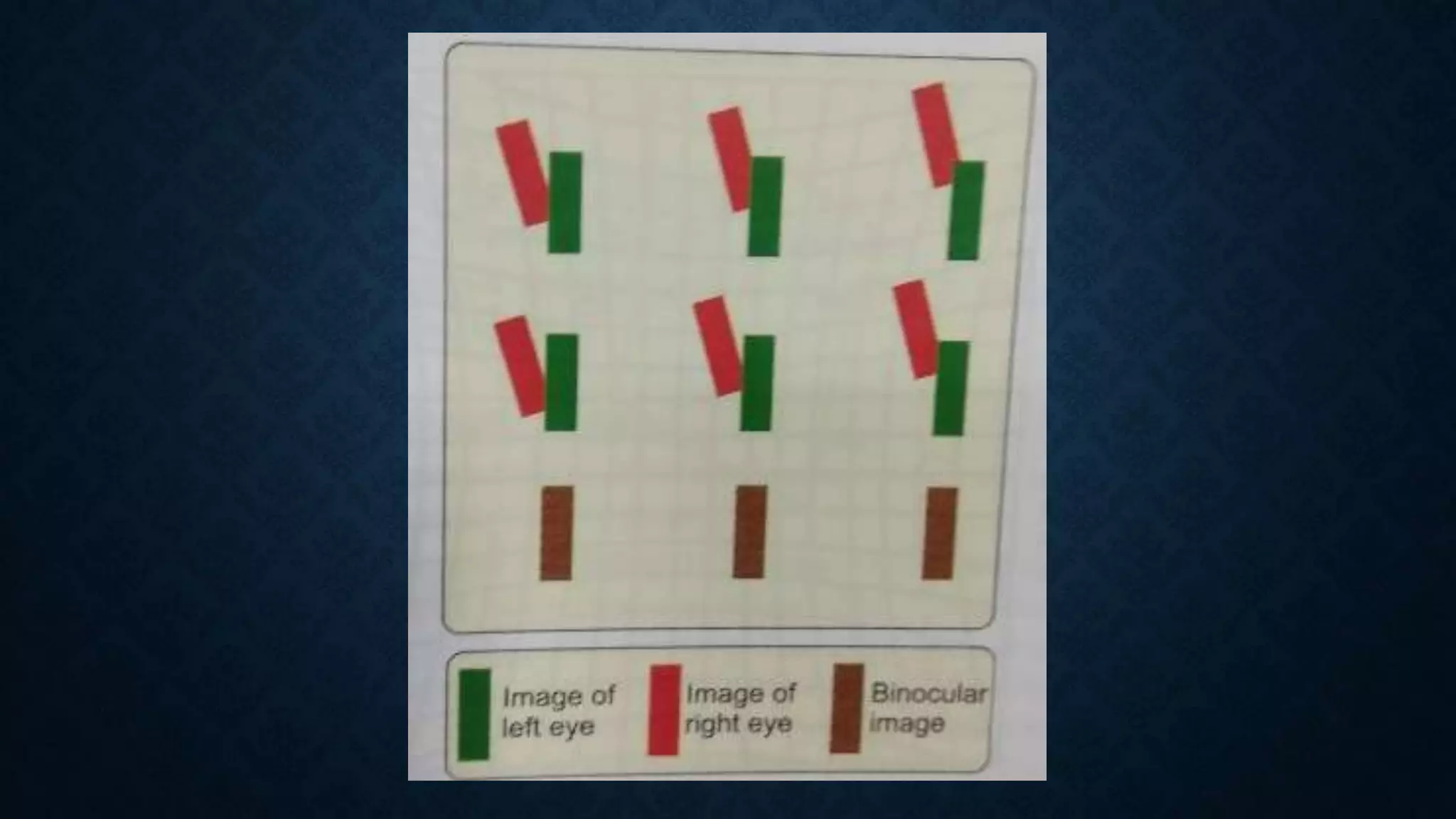
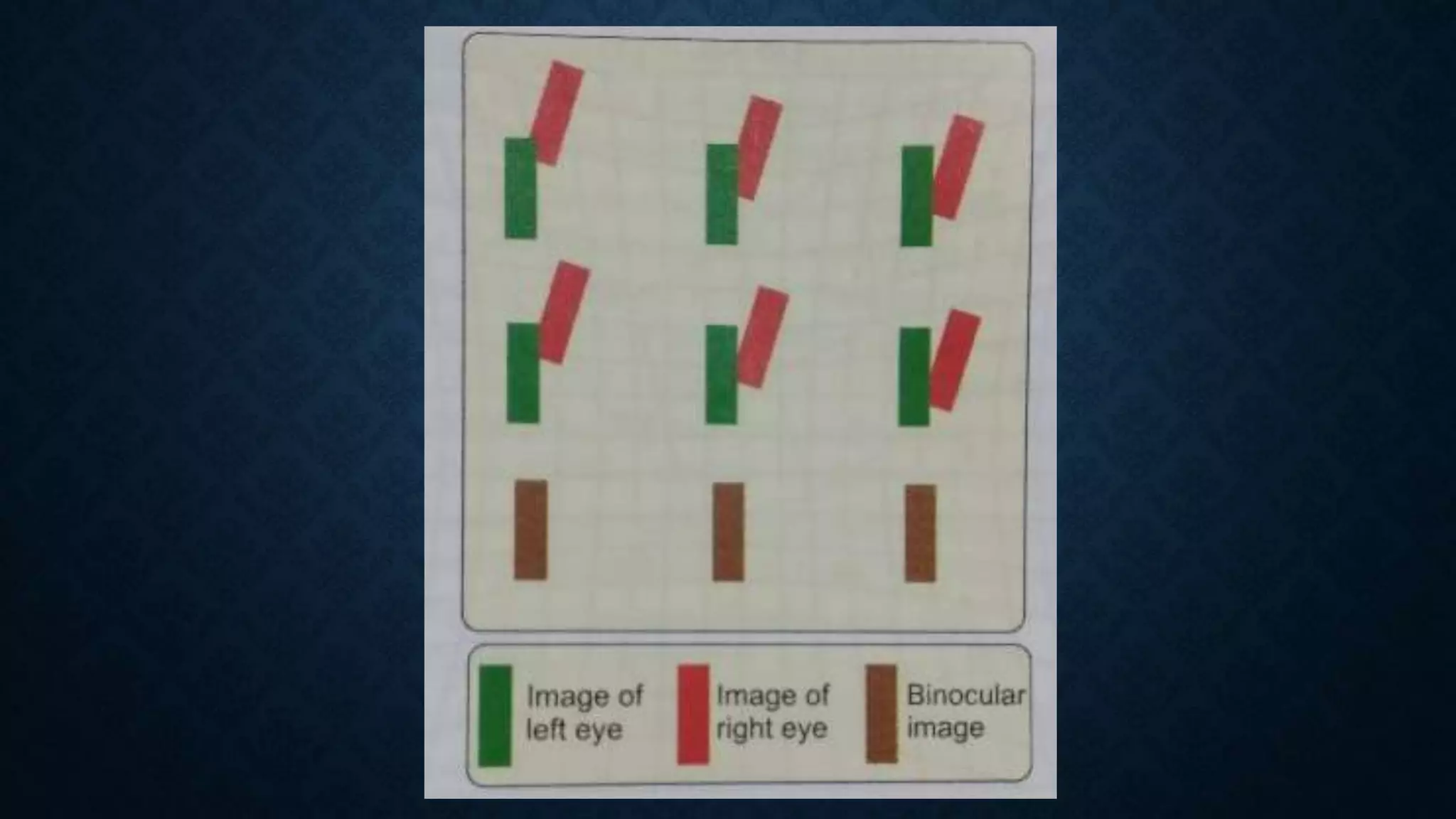
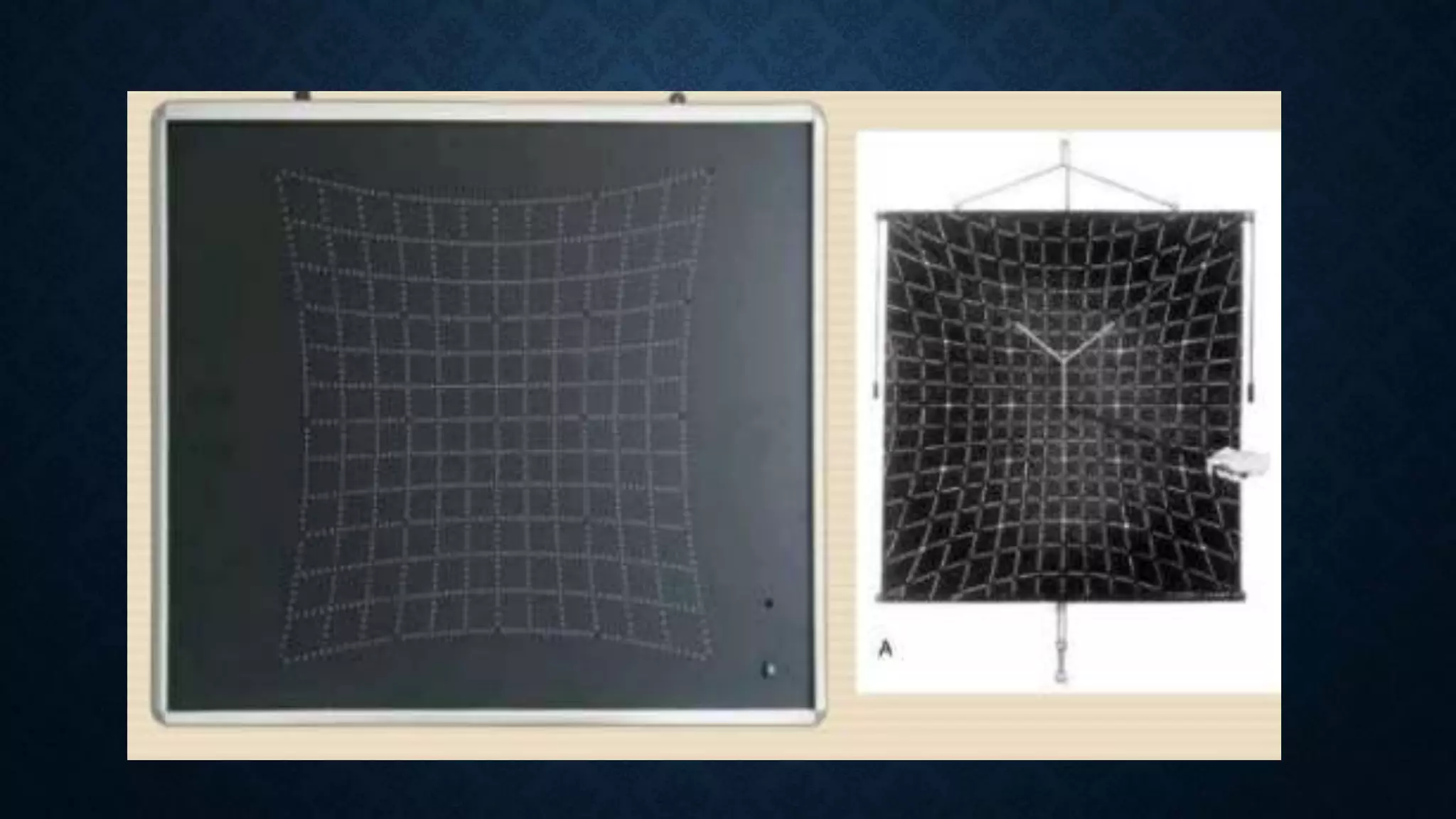
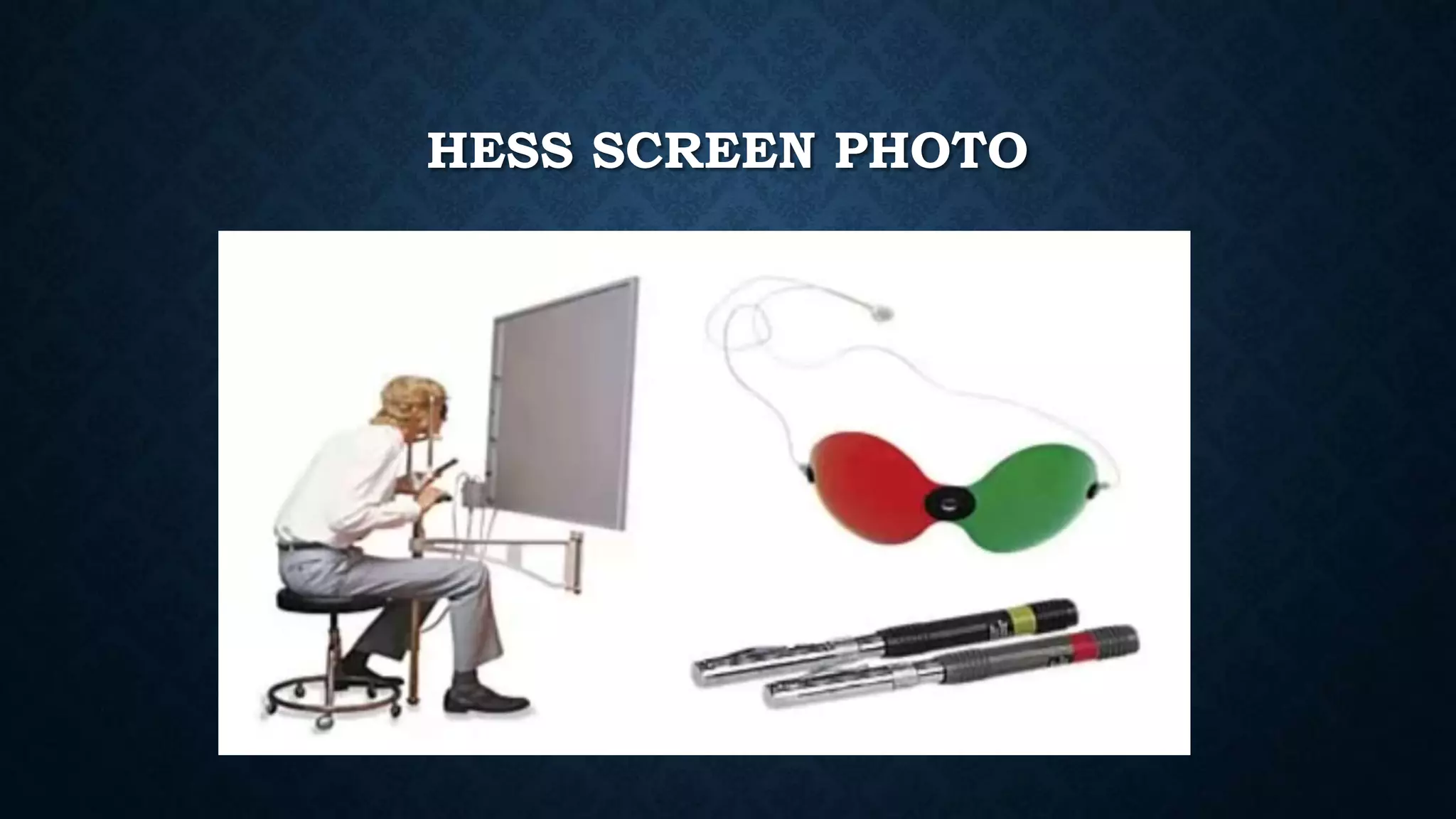
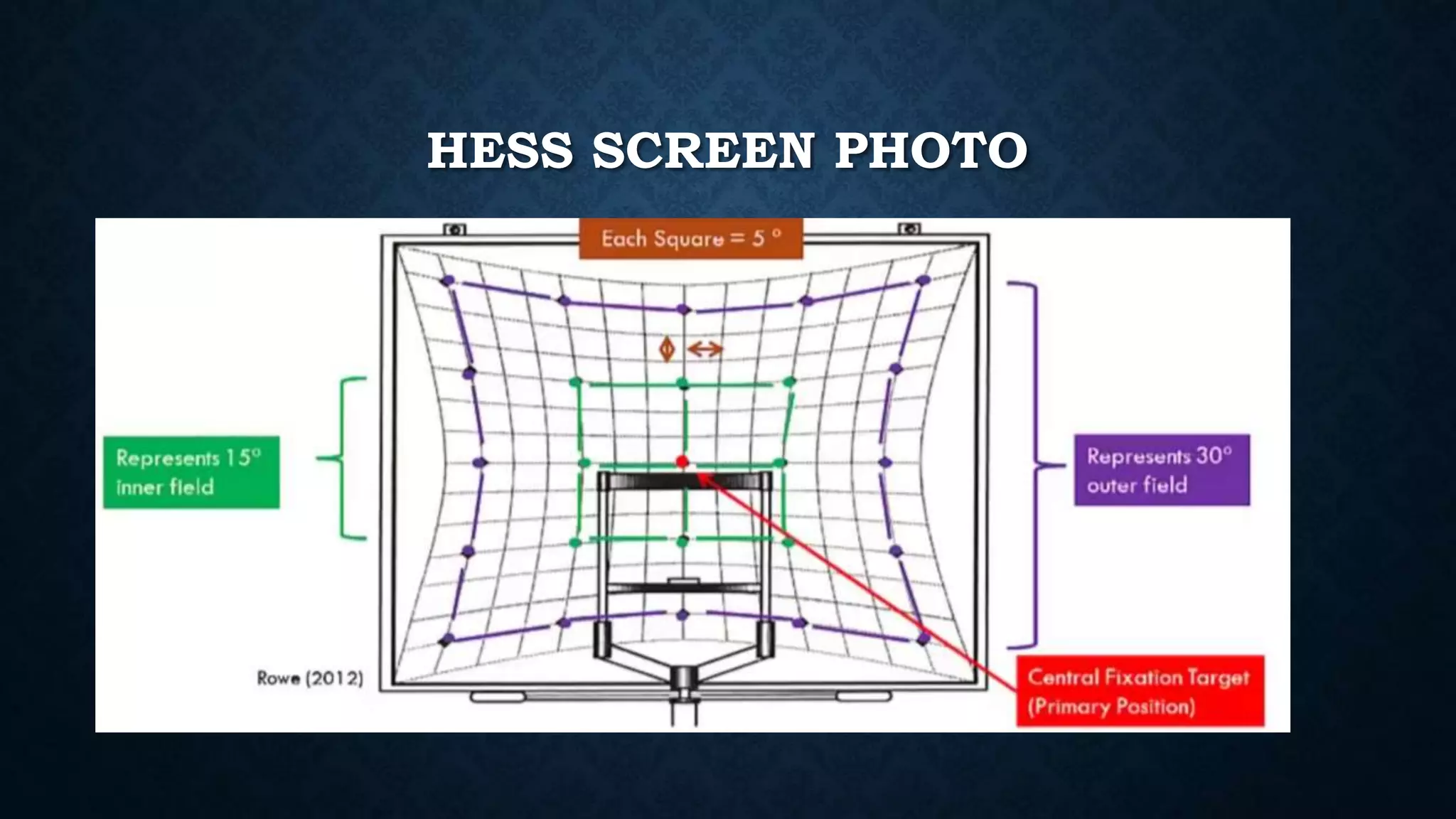
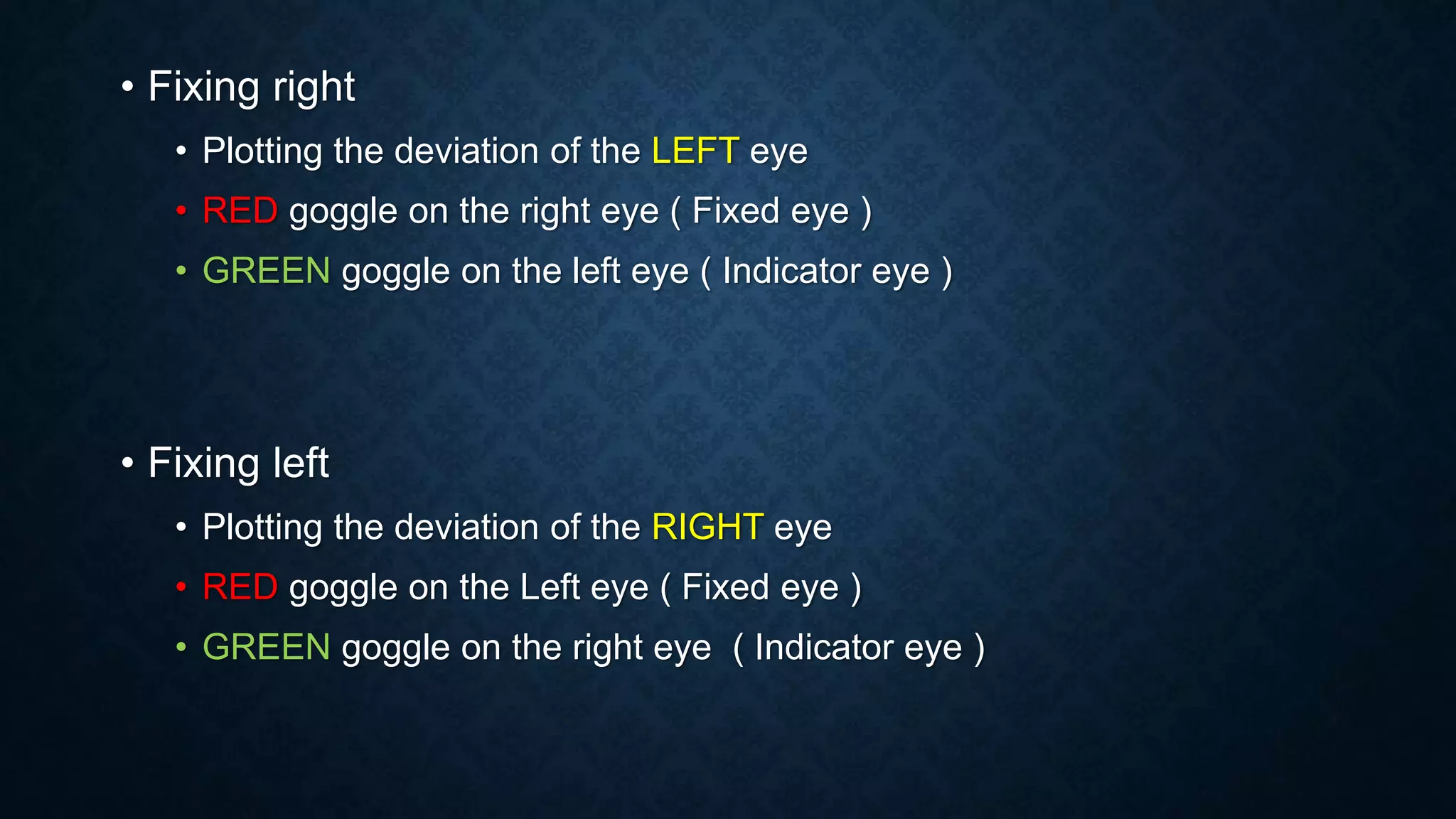
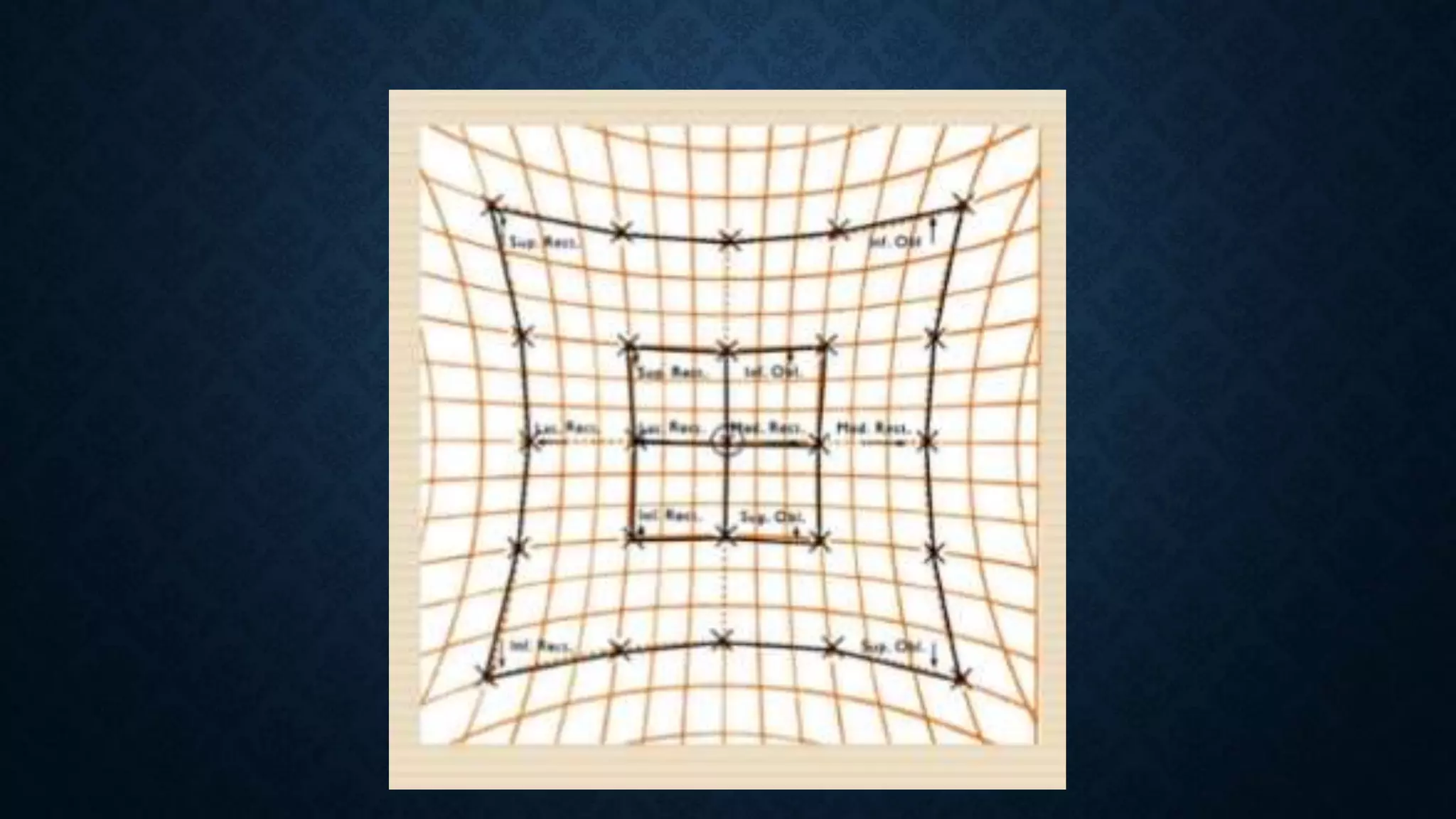
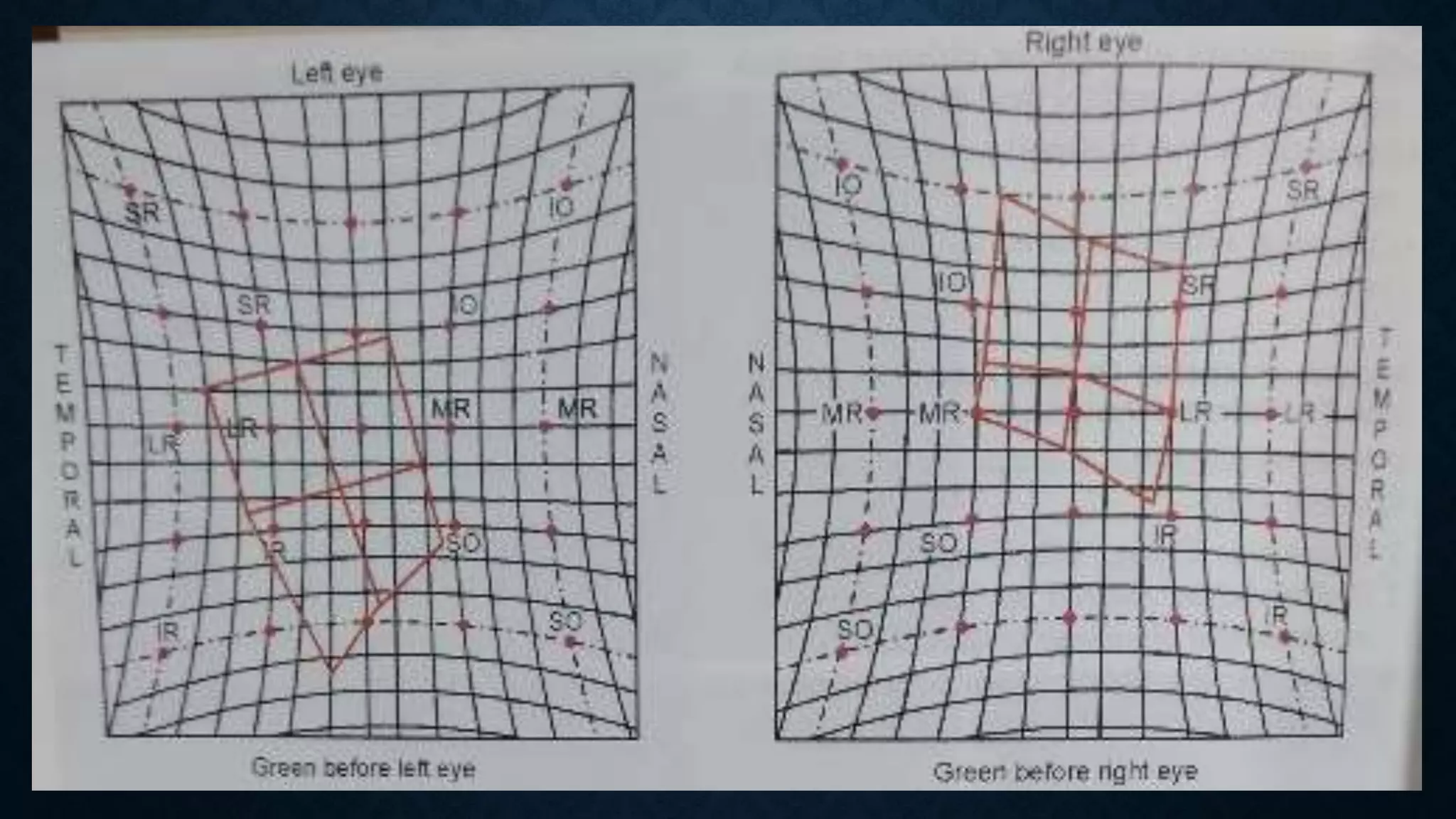
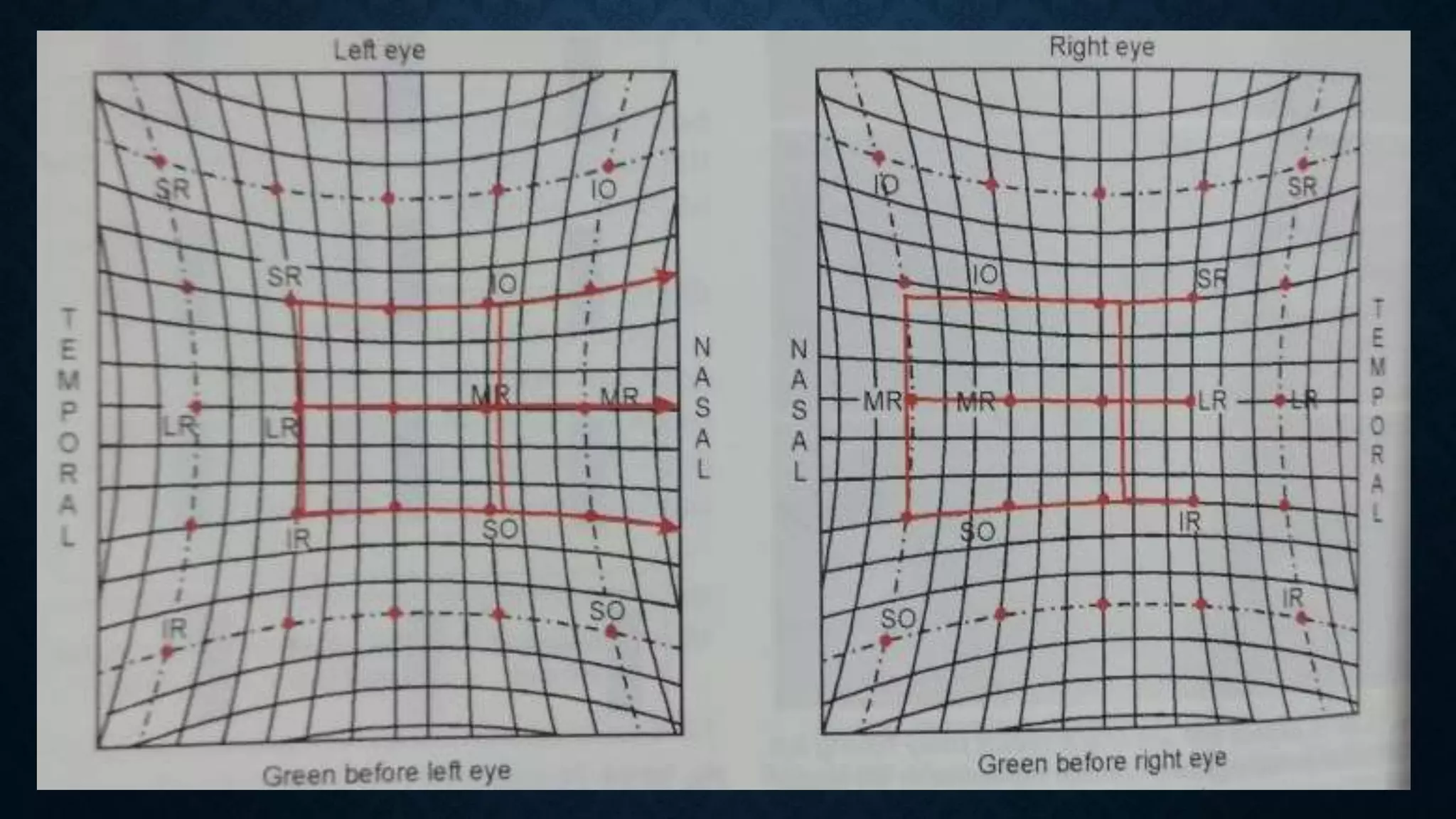
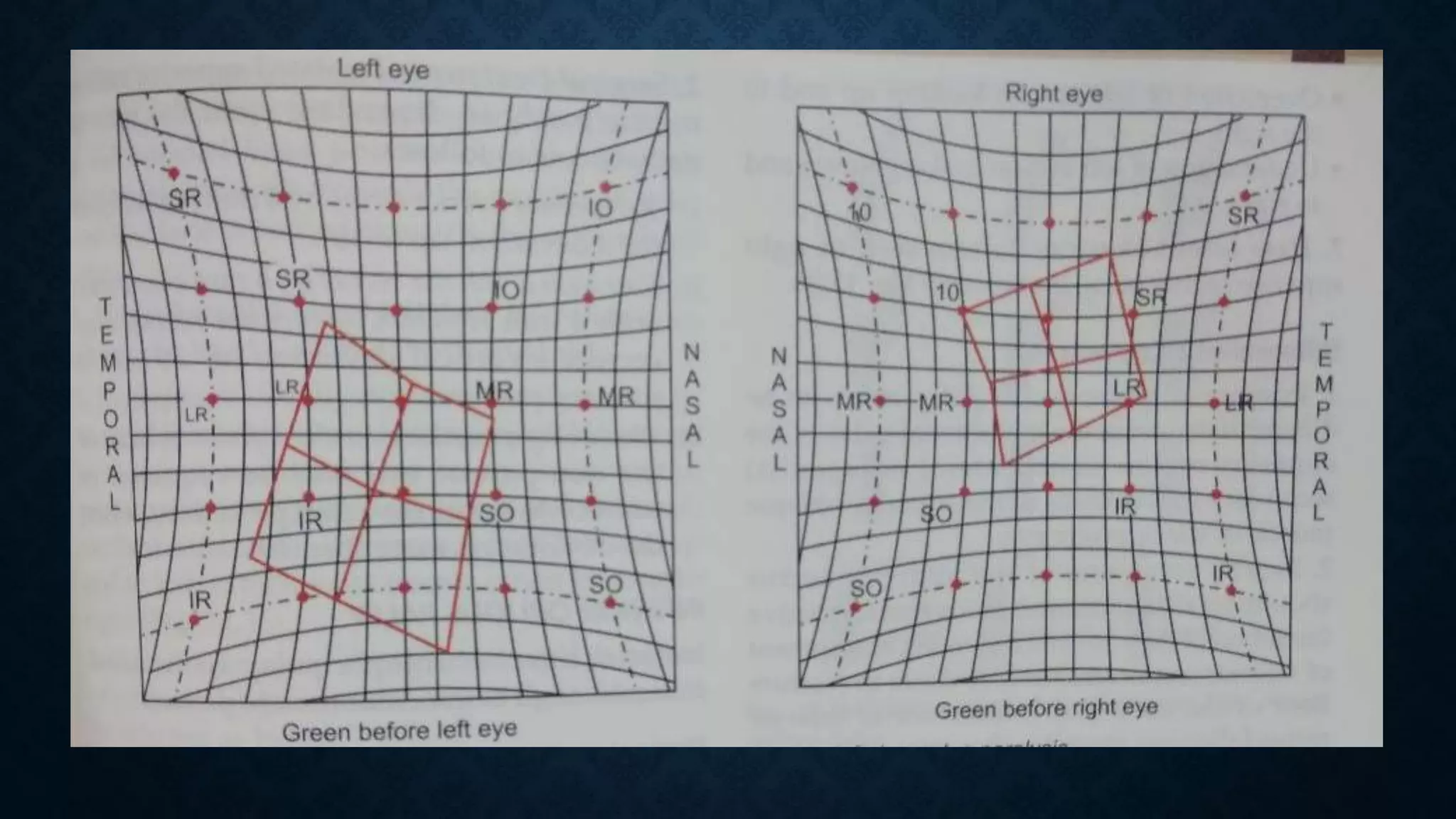
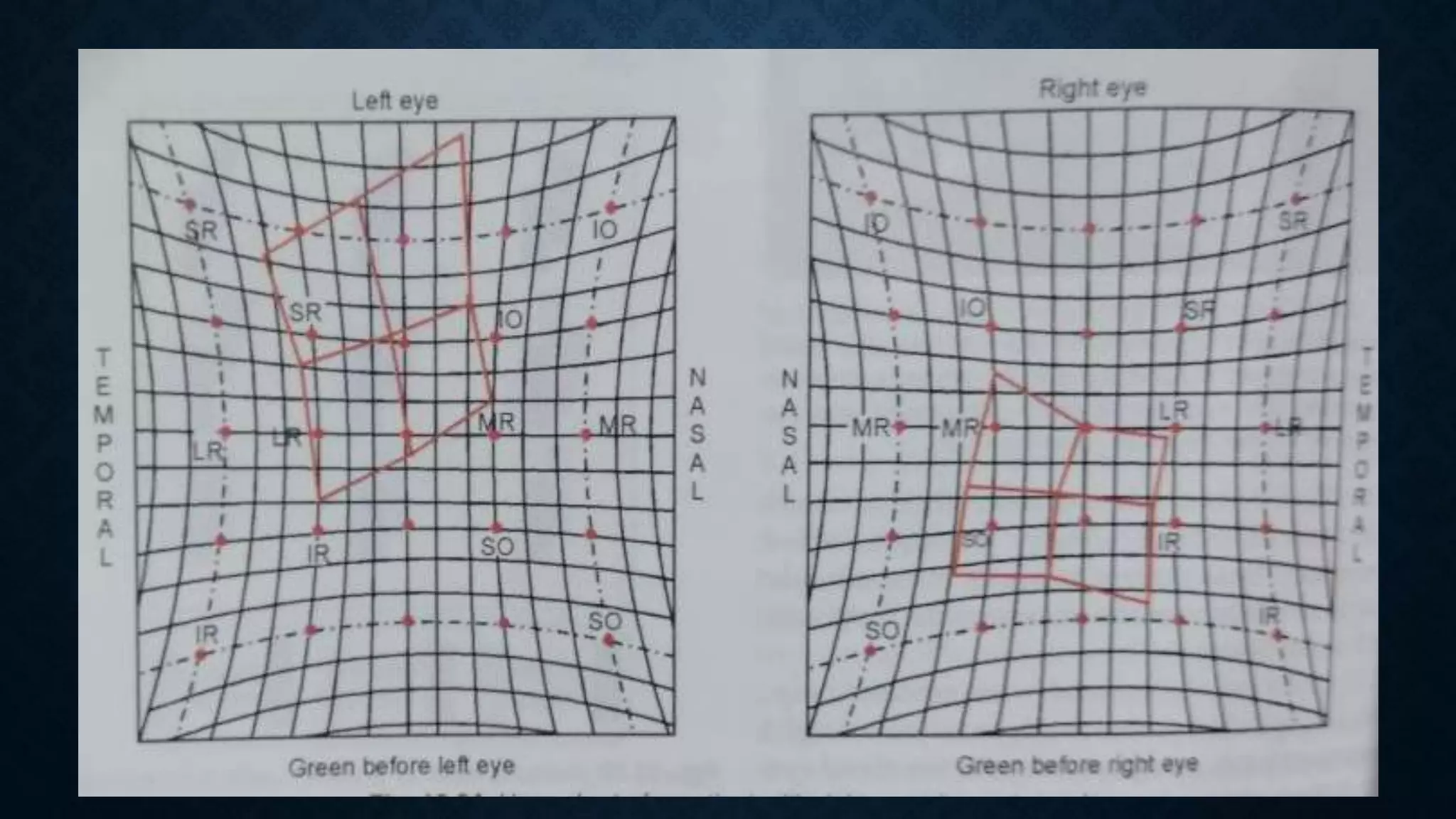
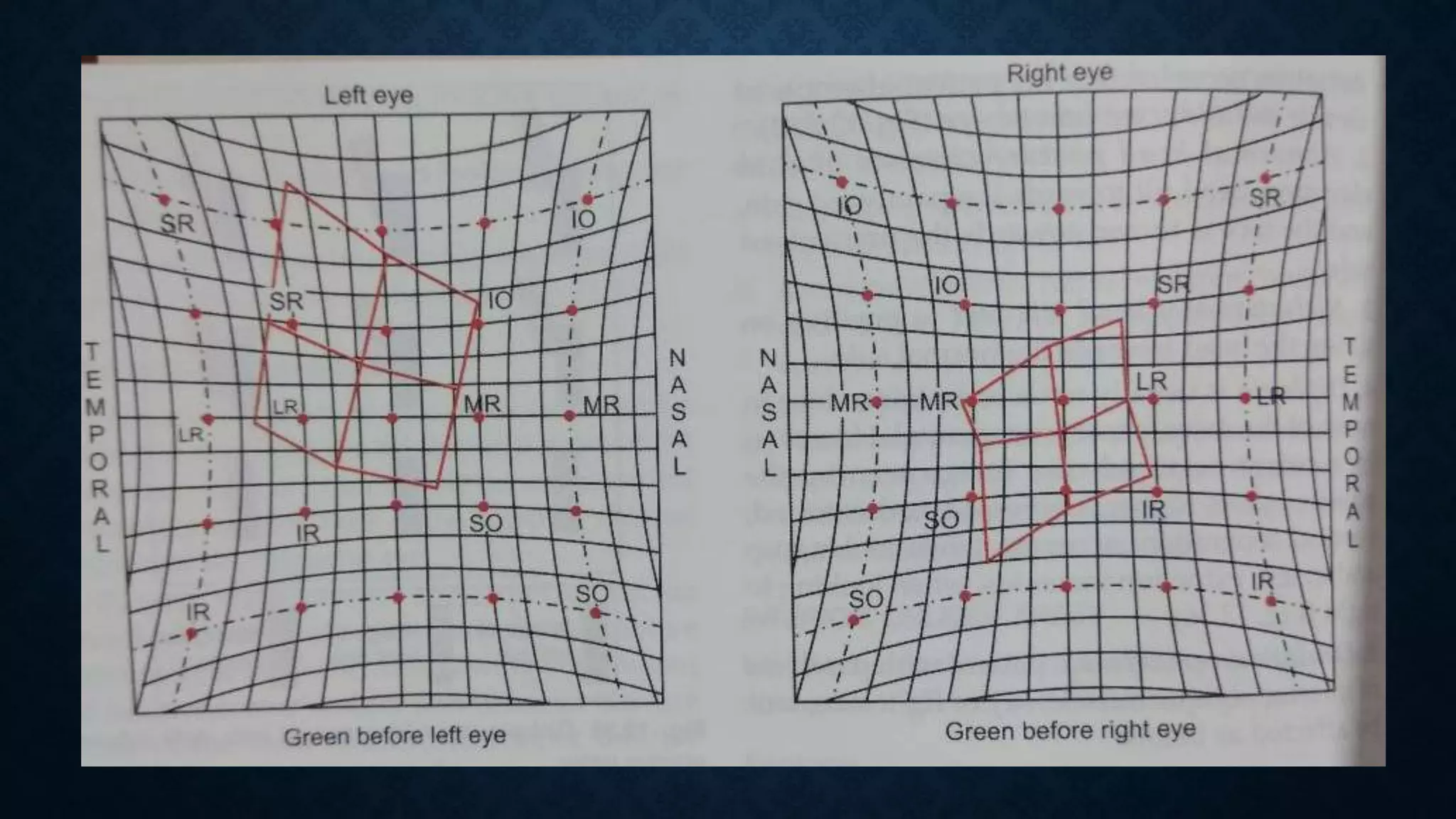
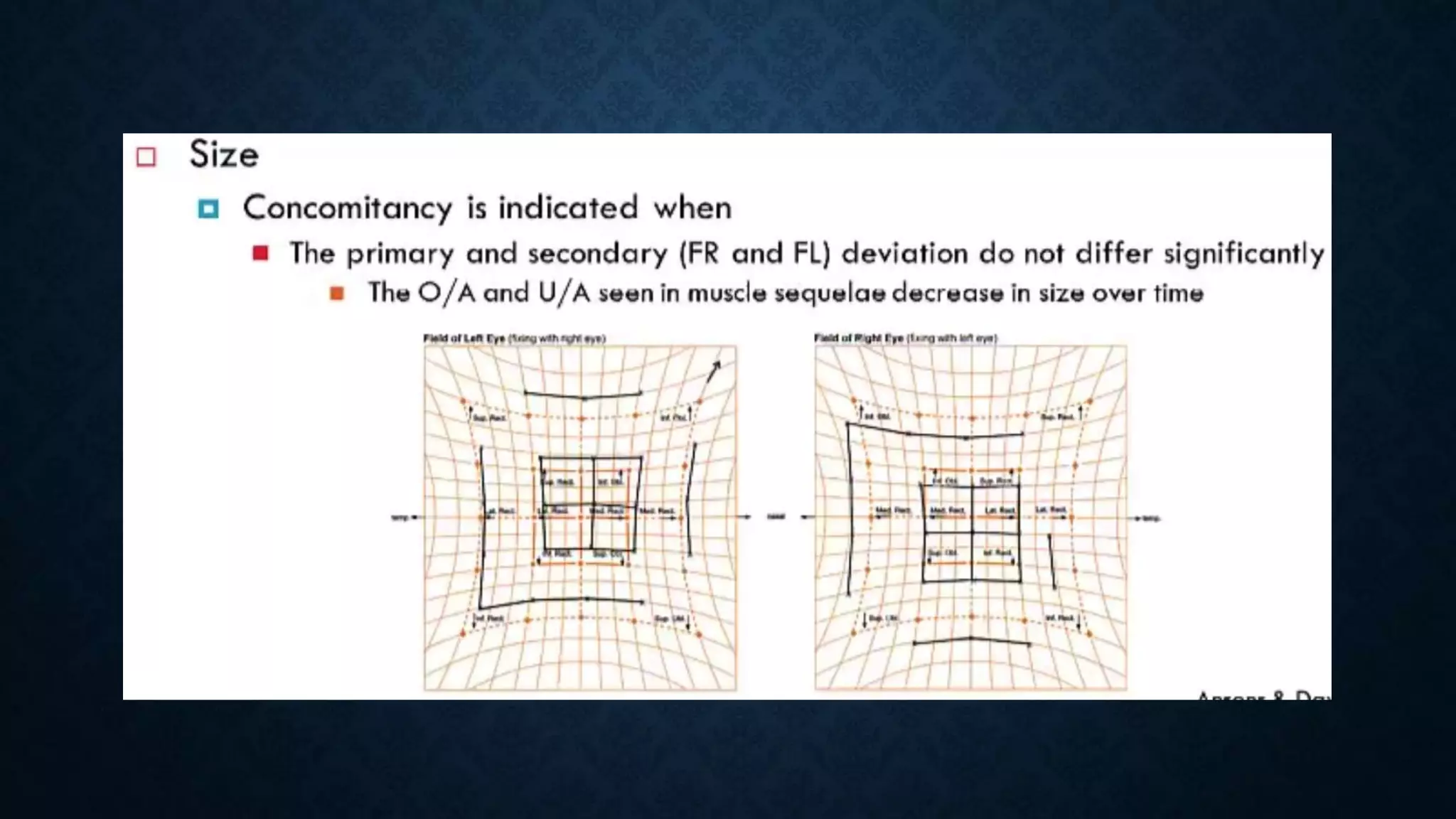
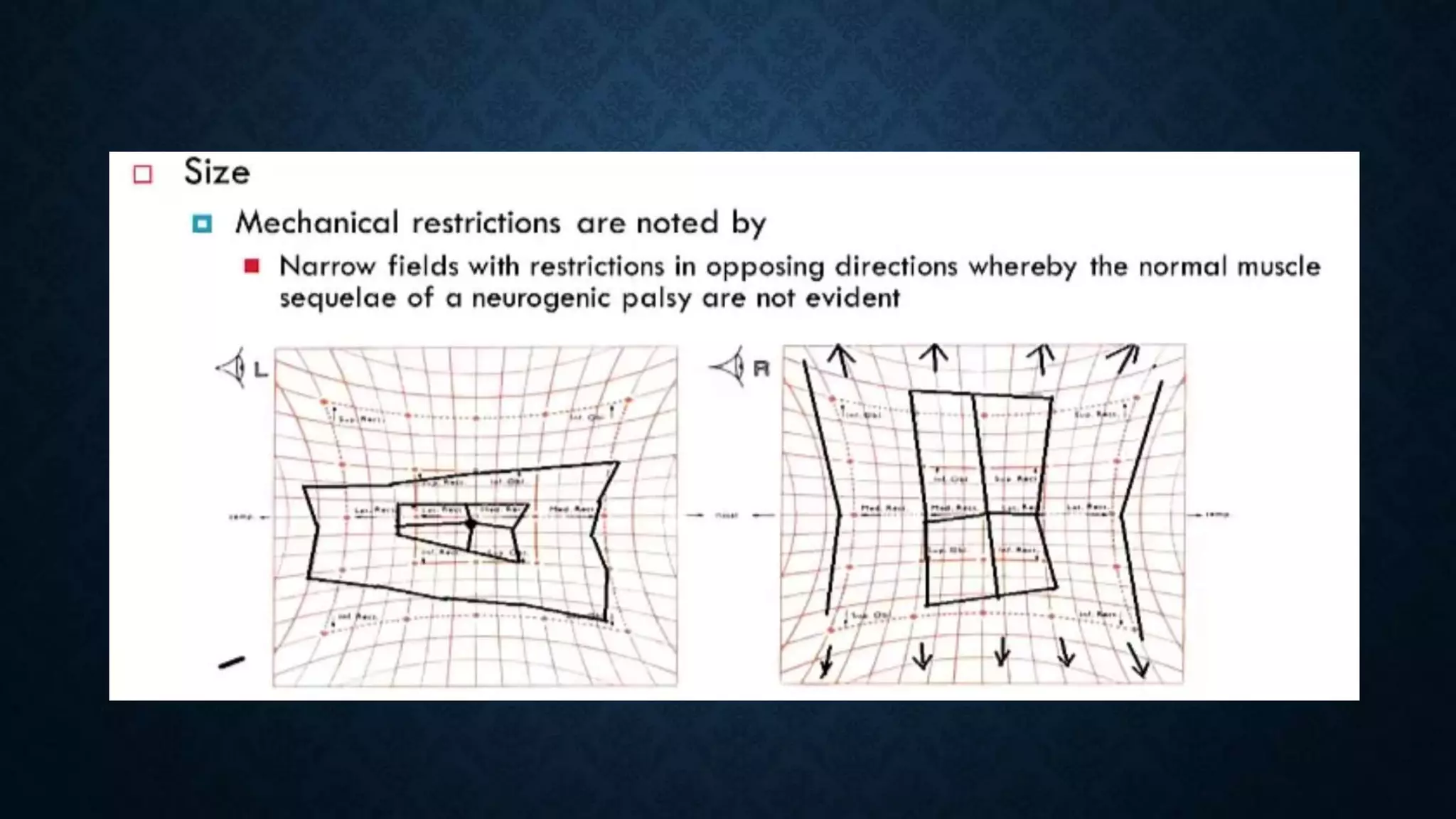
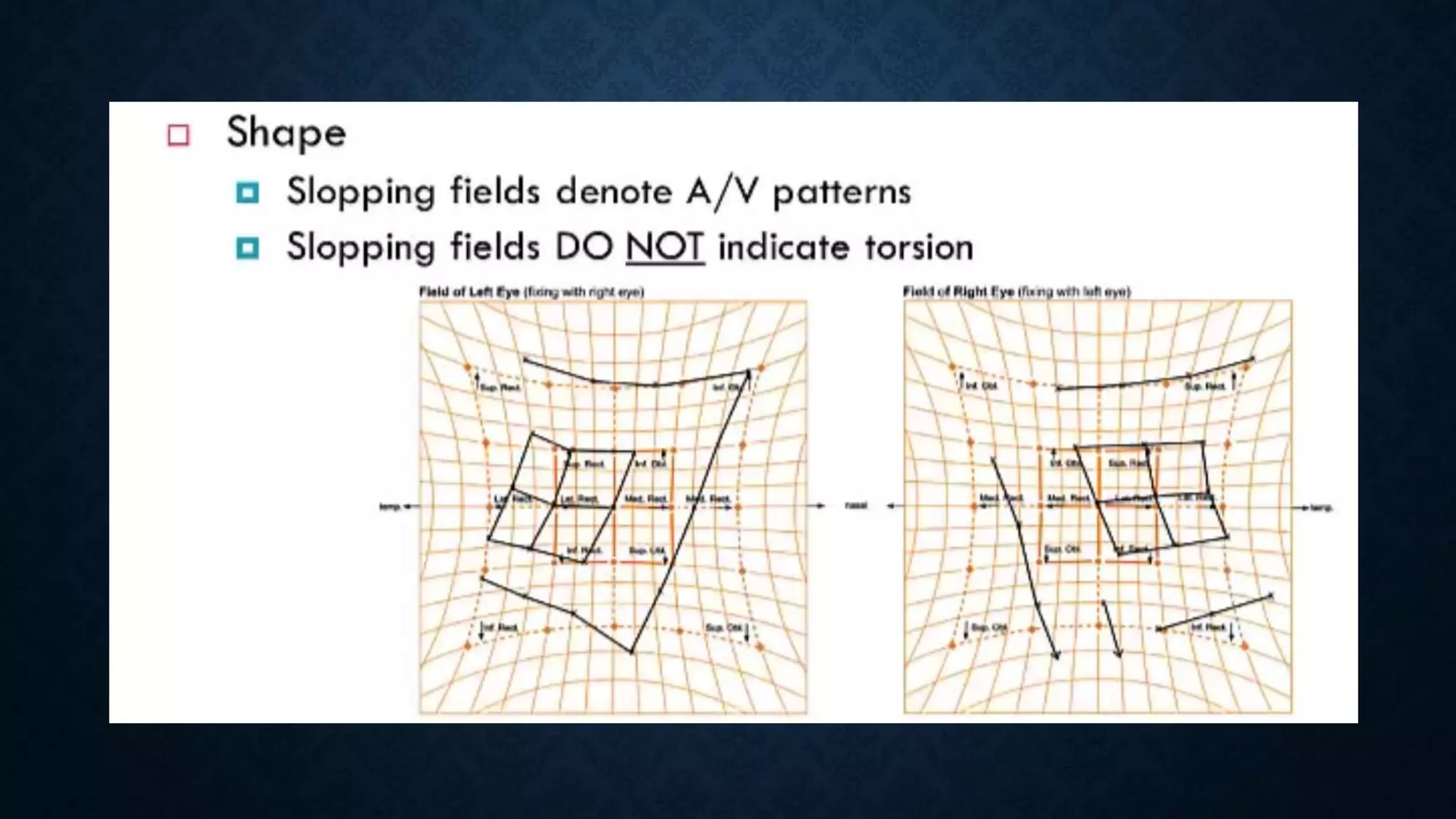
This document discusses various tests used to evaluate binocular vision, including cover tests, Hess charting, and diplopia charting. Cover tests are used to detect manifest or latent strabismus and determine deviation direction. Hess charting maps eye positions in 9 gazes using colored lenses to dissociate vision between eyes. It identifies muscle under or overaction. Diplopia charting records double vision separation in 9 gazes to localize affected muscles. These objective tests evaluate binocular function and strabismus type and localization.