Downloaded 246 times

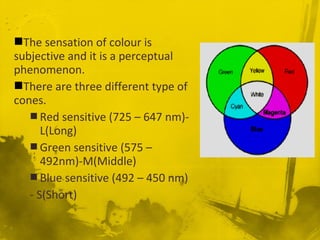

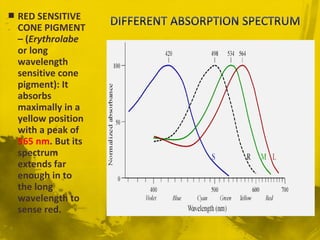

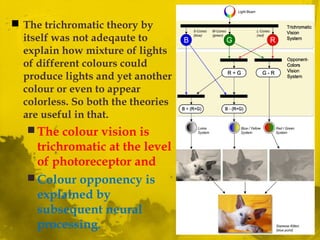
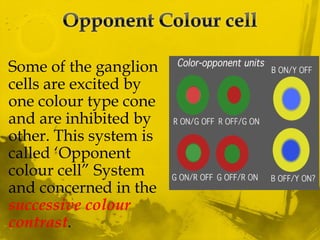
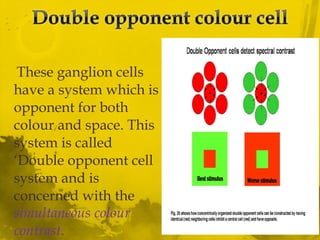
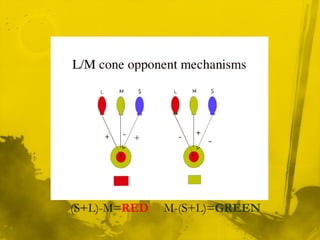
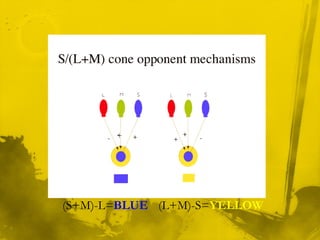
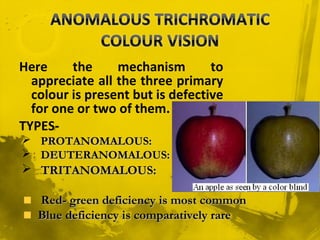


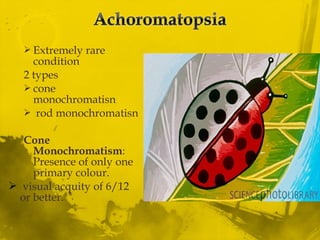
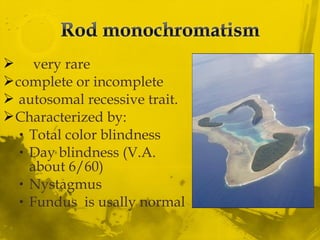
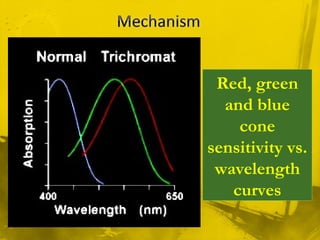
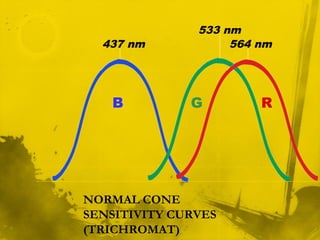
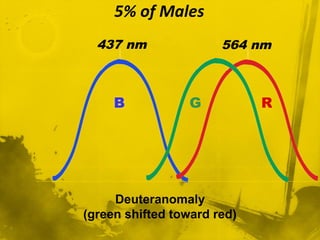
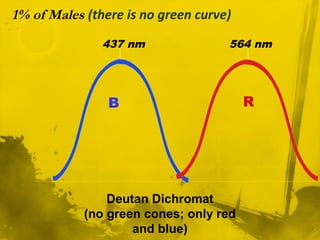
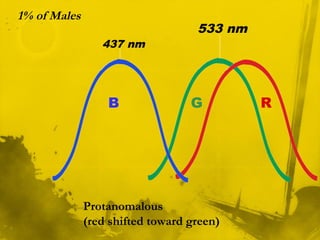
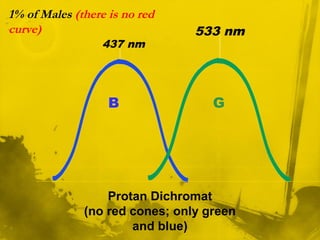
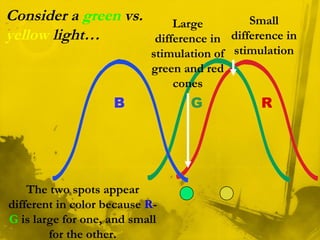
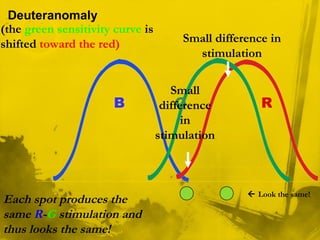
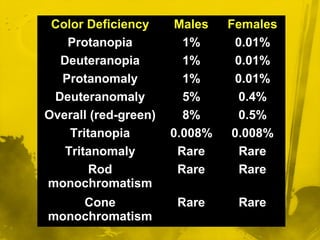


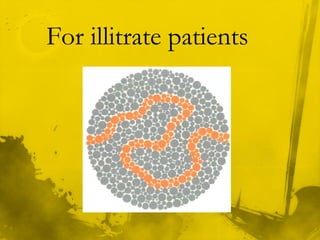
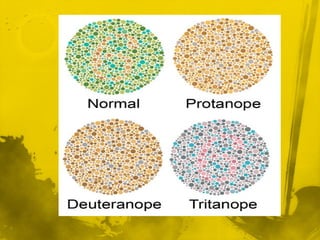







This document discusses color vision and color blindness. It begins by describing the three types of cones in the eye that are sensitive to long, middle, and short wavelengths of light, corresponding to red, green, and blue colors. It explains that color vision is achieved through the trichromatic theory, with colors resulting from different combinations of the three primary colors stimulating the cones. The document also discusses color opponent processing and color blindness, outlining different types like dichromacy and anomalous trichromacy that affect color perception. Tests for color blindness like Ishihara plates are also mentioned.













































































