Download as PDF, PPTX
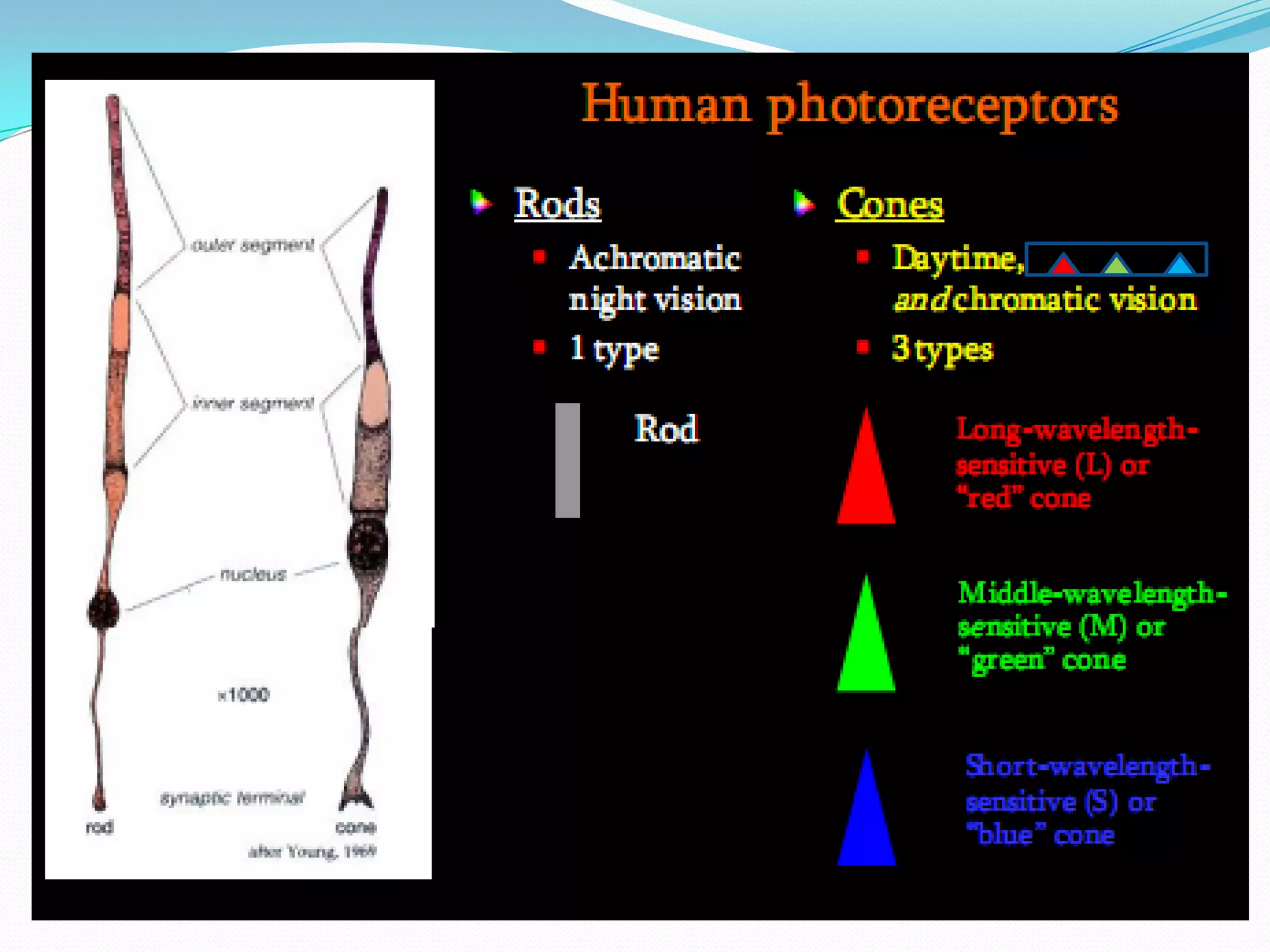
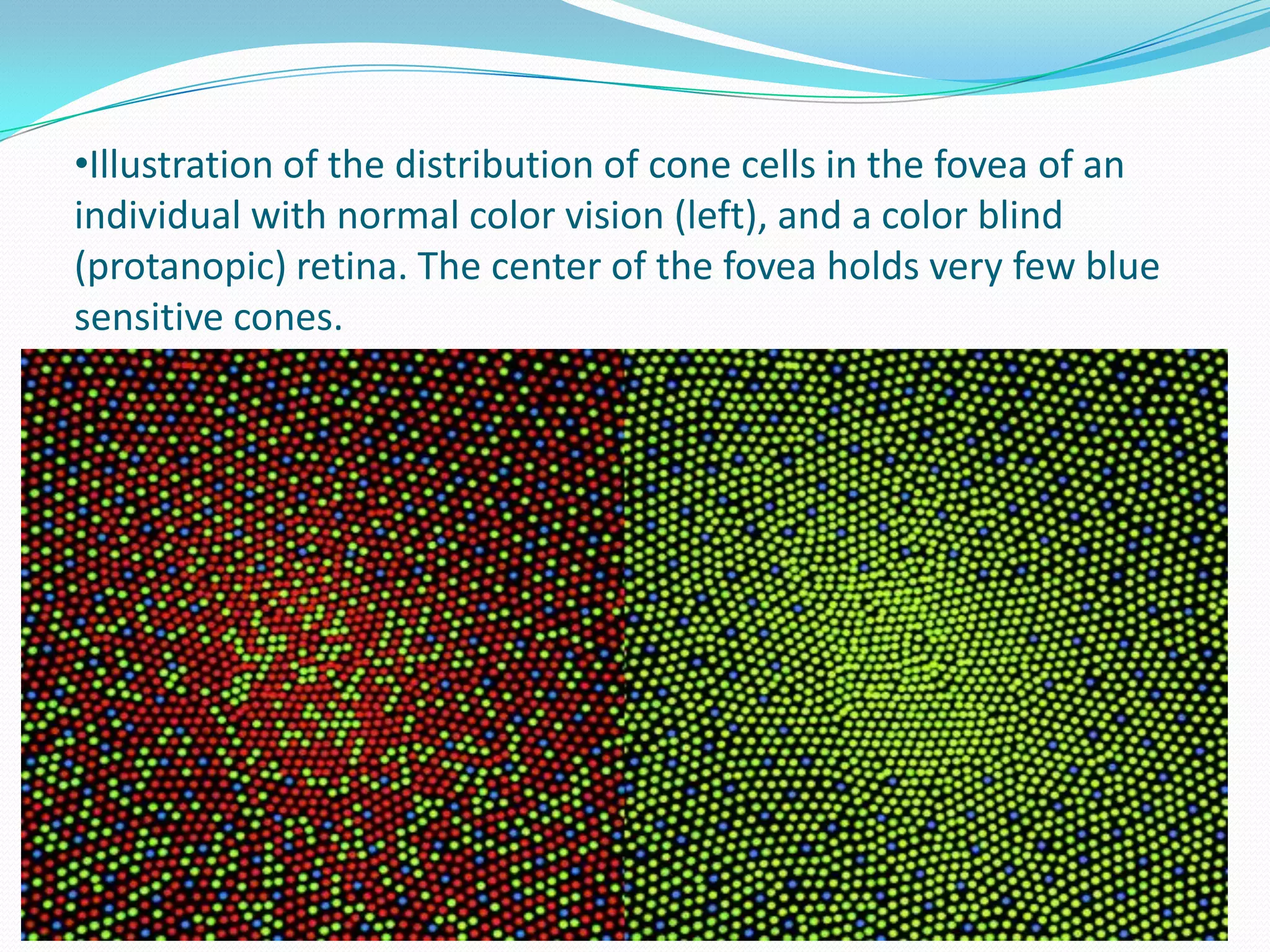
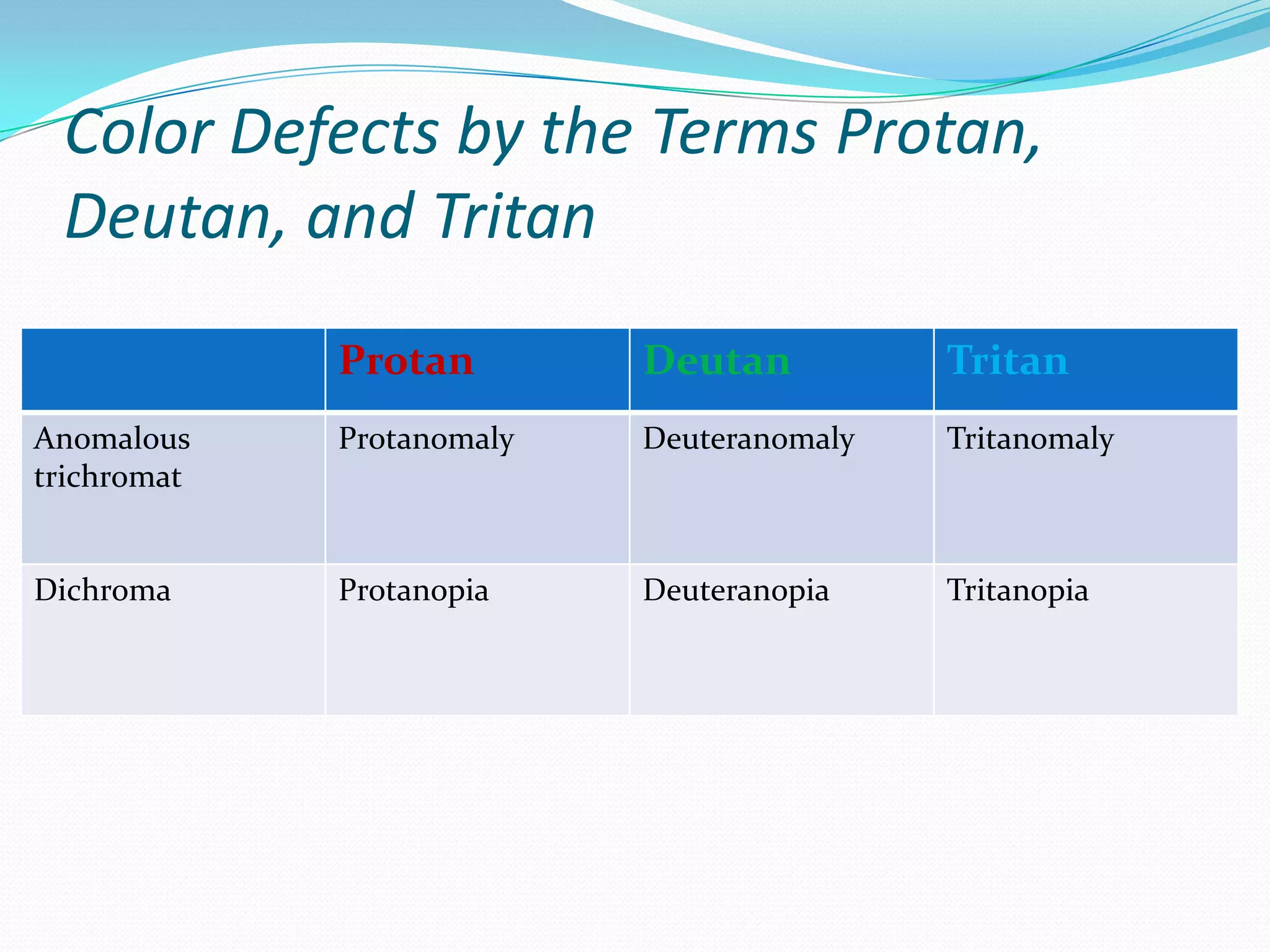
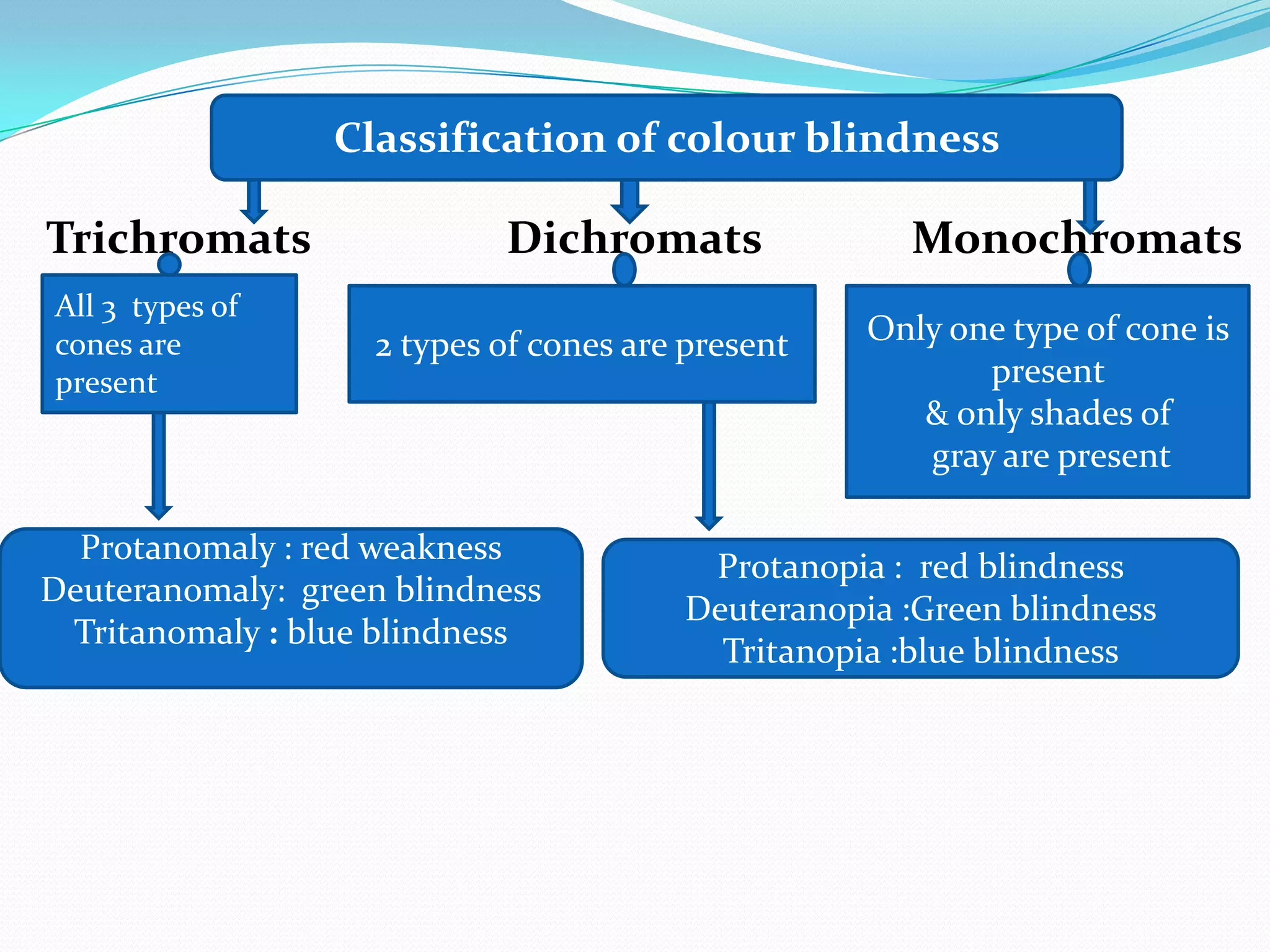
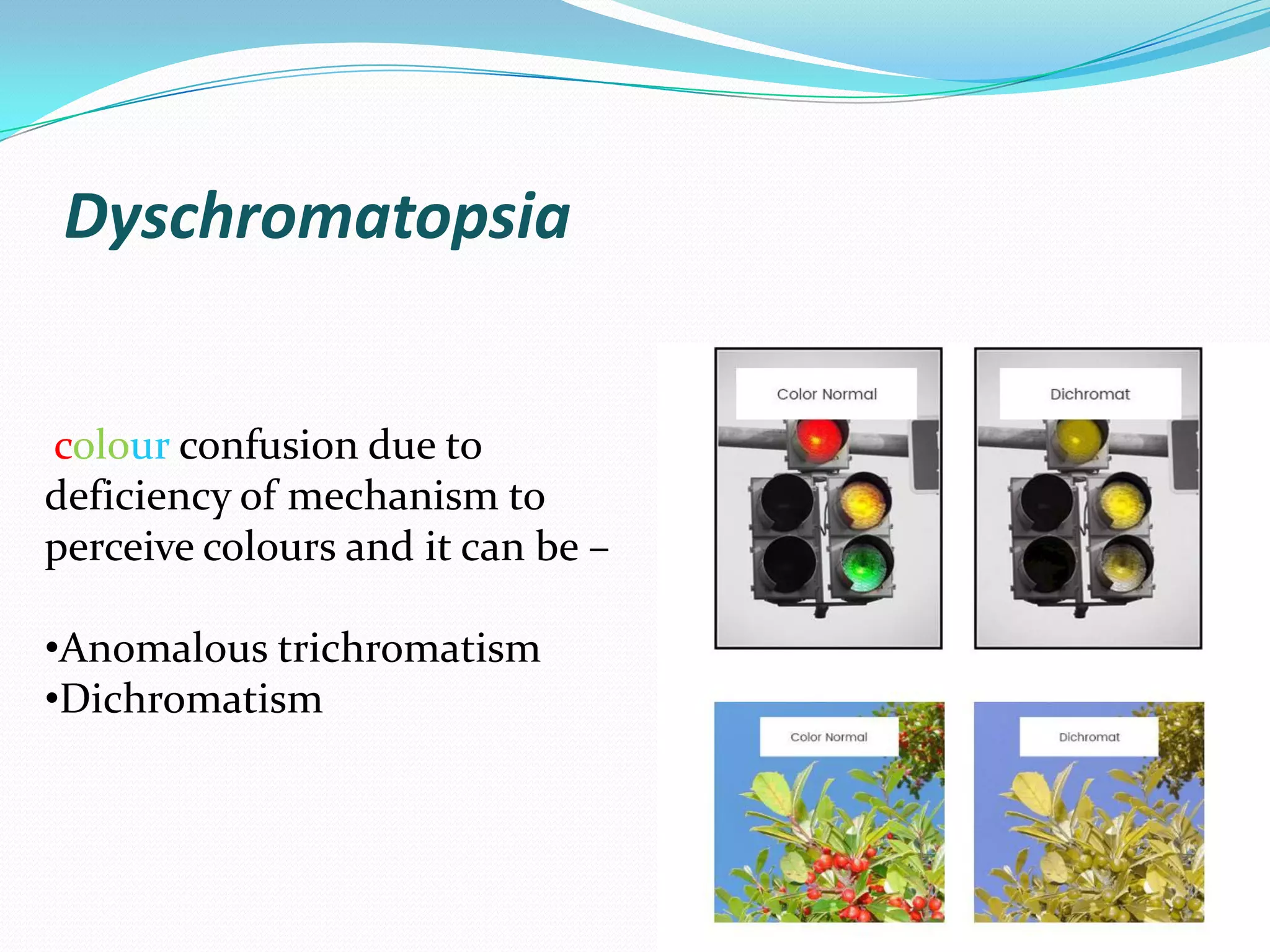
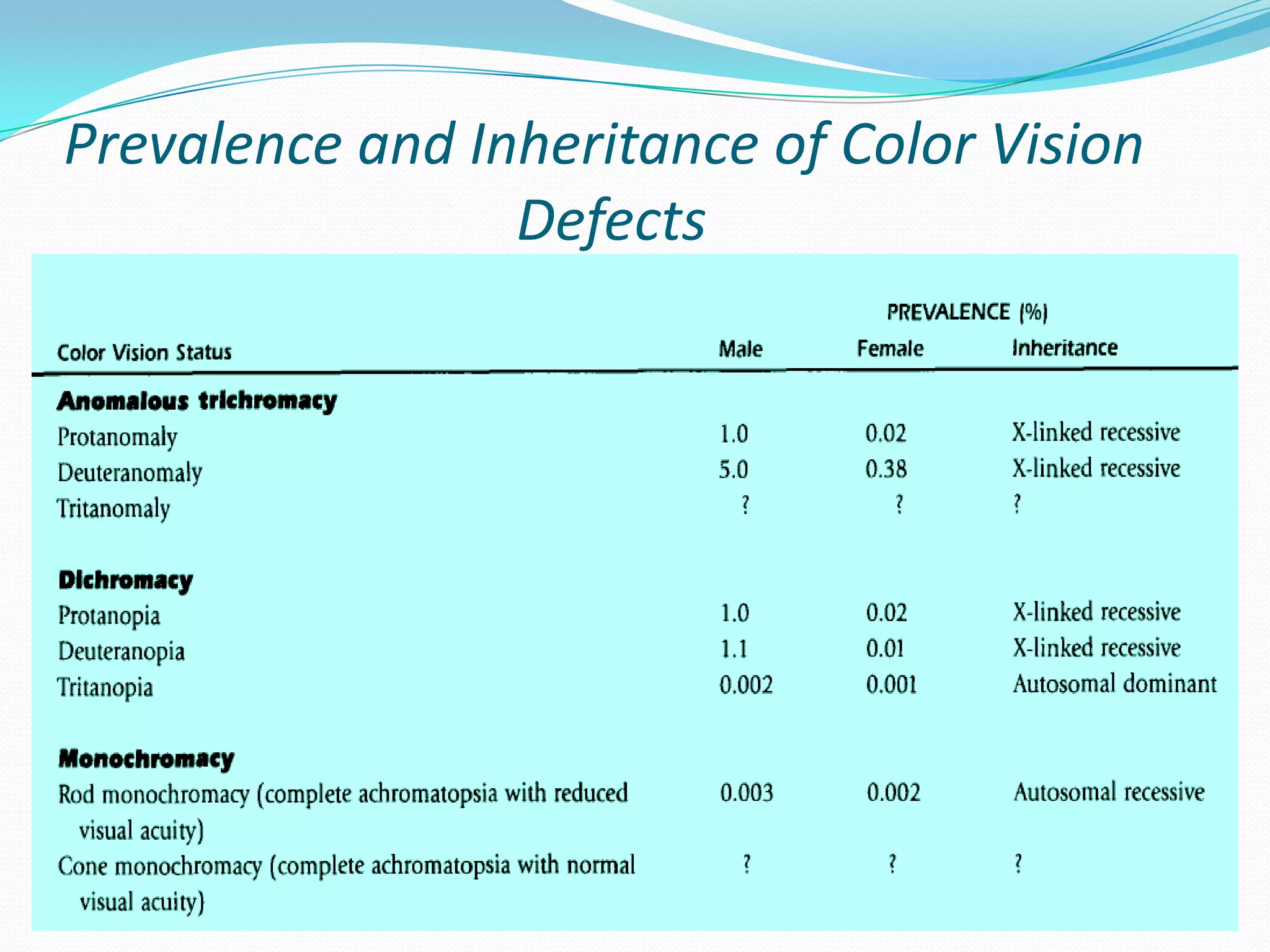
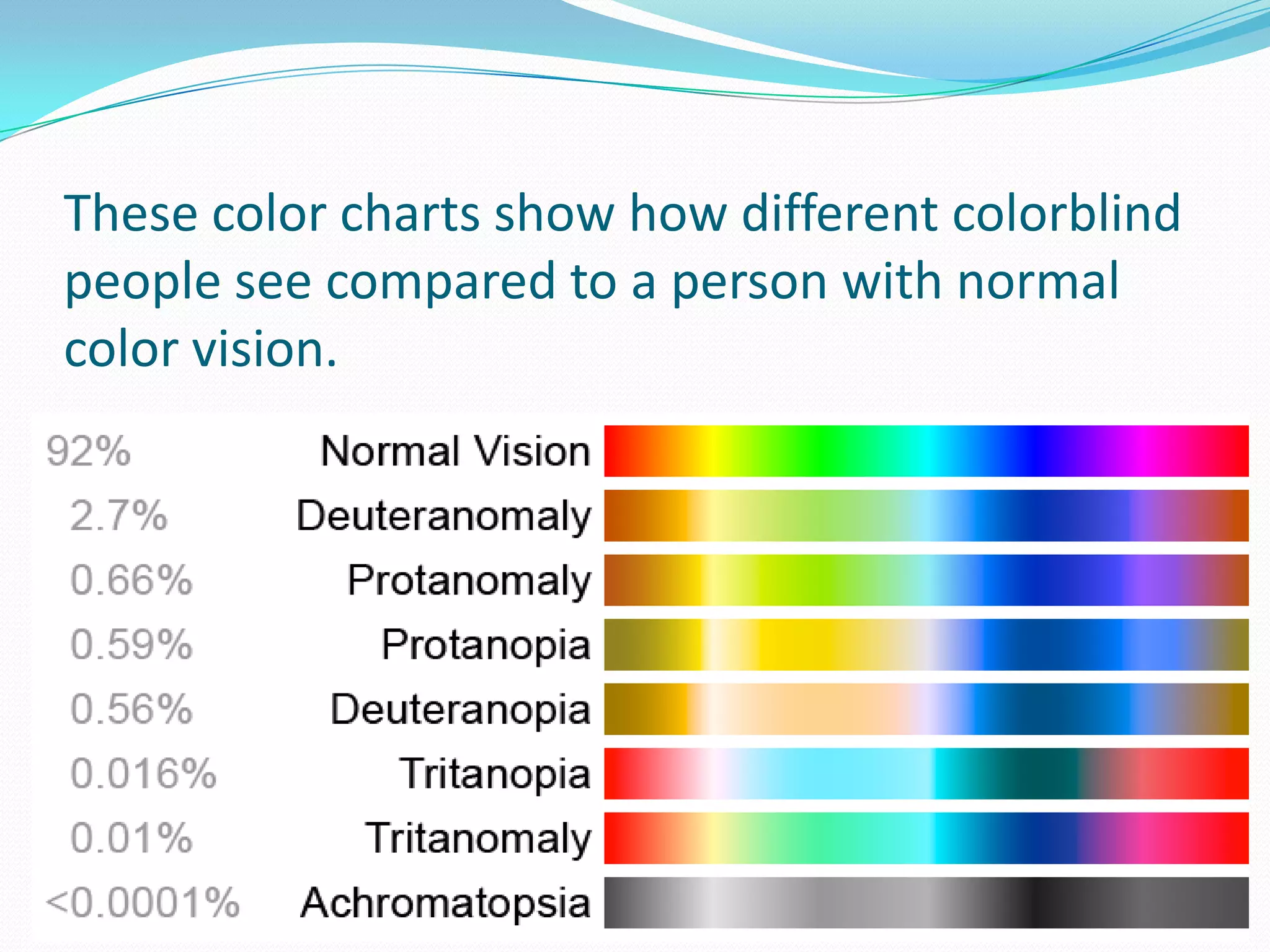

This document discusses color vision and color blindness. It begins with an introduction to color vision, noting that it is mediated by cone cells in the retina and allows humans to perceive differences in light wavelengths. It then discusses types of color blindness such as red-green and blue-yellow deficiencies. The types of color blindness are classified and the prevalence and inheritance patterns are described. Causes of acquired color vision defects from ocular diseases and medications are also summarized.














































































