This document discusses automated perimetry, which is used to evaluate the visual field. It begins by explaining the importance of perimetry in diagnosing and monitoring glaucoma and other conditions. It then defines key concepts like the visual field and hill of vision. The document discusses the components and procedures of automated perimetry testing, including factors that influence the results like stimulus characteristics, fixation monitoring, and testing strategies. It describes different perimetry tests and their applications in evaluating various eye diseases. In summary, the document provides an overview of automated perimetry, its role in eye care, and the technical aspects of performing this important visual field assessment test.

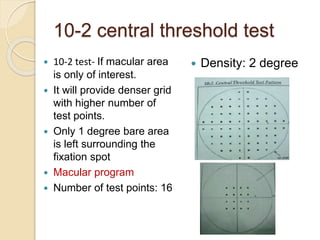


























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









