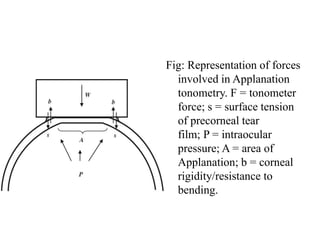
Goldman applanation tonometry is an effective method for measuring intraocular pressure (IOP) using a slit-lamp and fluorescein-stained cornea. The technique utilizes the Imbert-Fick principle and involves aligning semicircles created by a biprism while applying a measurable force to the cornea. Factors such as corneal astigmatism, curvature, edema, and thickness can affect the accuracy of IOP readings, necessitating careful patient handling and preparation.