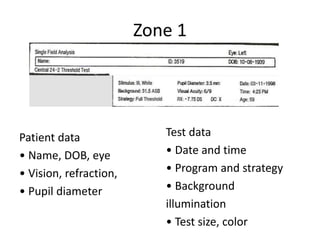
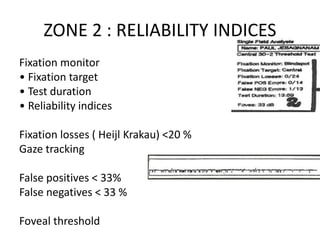
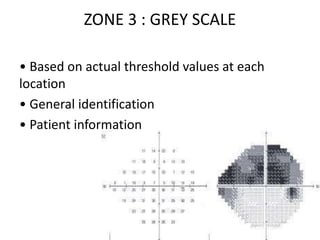
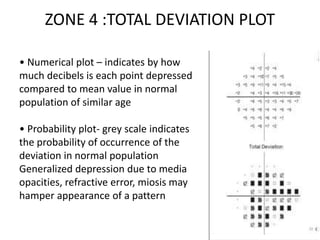
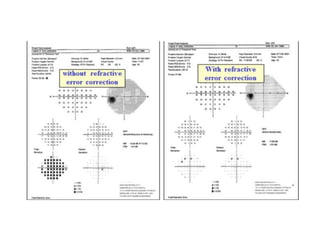
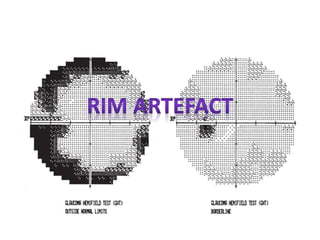
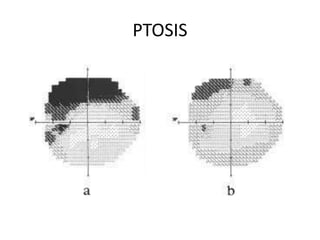
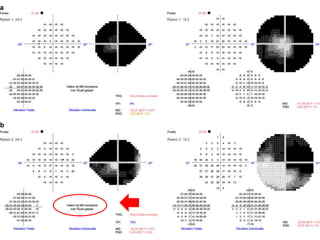
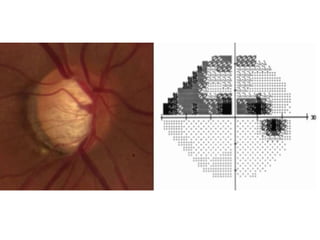
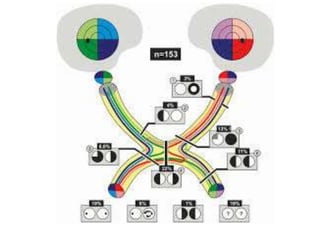
This document discusses the visual field and visual field testing. It defines the visual field as the part of the environment that can be detected by a steady eye. It then discusses the physiological basis of the visual field and factors that can affect visual field testing results, such as stimulus characteristics and patient factors. The document also summarizes different types of visual field defects and explains common perimetry techniques and their advantages. It provides details on visual field test interpretation, including reliability indices, total and pattern deviation plots, and classification of results.