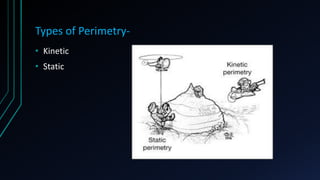
This document summarizes key aspects of perimetry testing. It defines the normal visual field and describes how perimetry can be used to detect functional vision loss and monitor disease progression. Two main types of perimetry are discussed: kinetic and static. Details are provided on testing strategies, stimuli brightness, interpreting results like total deviation and reliability indices. The document emphasizes the importance of perimetry in glaucoma and neurological diagnosis and management.







![Threshold estimation- [BRACKETING STRATEGY]
• 4-2 STRATEGY algorithm is most commonly used
• STEPS-
Testing started with full threshold
Intensity of stimulus is decreased
by 4db Steps till stimulus is NO
longer seen
Now stimulus is increased by 2db
steps till stimulus is seen again](https://image.slidesharecdn.com/perimetry-190619034634/85/Perimetry-15-320.jpg)

![• FAST PAC- decreased test time by 40%
- follows similar stair-stepping technique as in
full threshold
- but increment is 3db instead of 4db.
- crosses threshold only once
• SITA [SWEDISH INTERACTIVE THRESHOLD ALGORITHM]
standard- takes ½ time than full threshold technique
• SITA fast- takes ½ time than Fastpac](https://image.slidesharecdn.com/perimetry-190619034634/85/Perimetry-18-320.jpg)