Downloaded 155 times




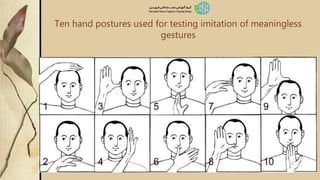
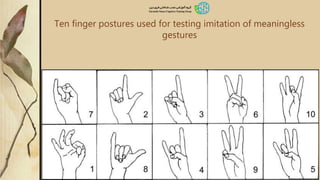





The document discusses apraxia, a disorder characterized by the inability to perform learned movements despite having intact sensory and motor function. It outlines various types of apraxia, their clinical manifestations, and the role of the parietal cortex in motor control. Additionally, it highlights the significance of mirror neurons and presents clinical tests for diagnosing apraxia.























































































