Downloaded 56 times








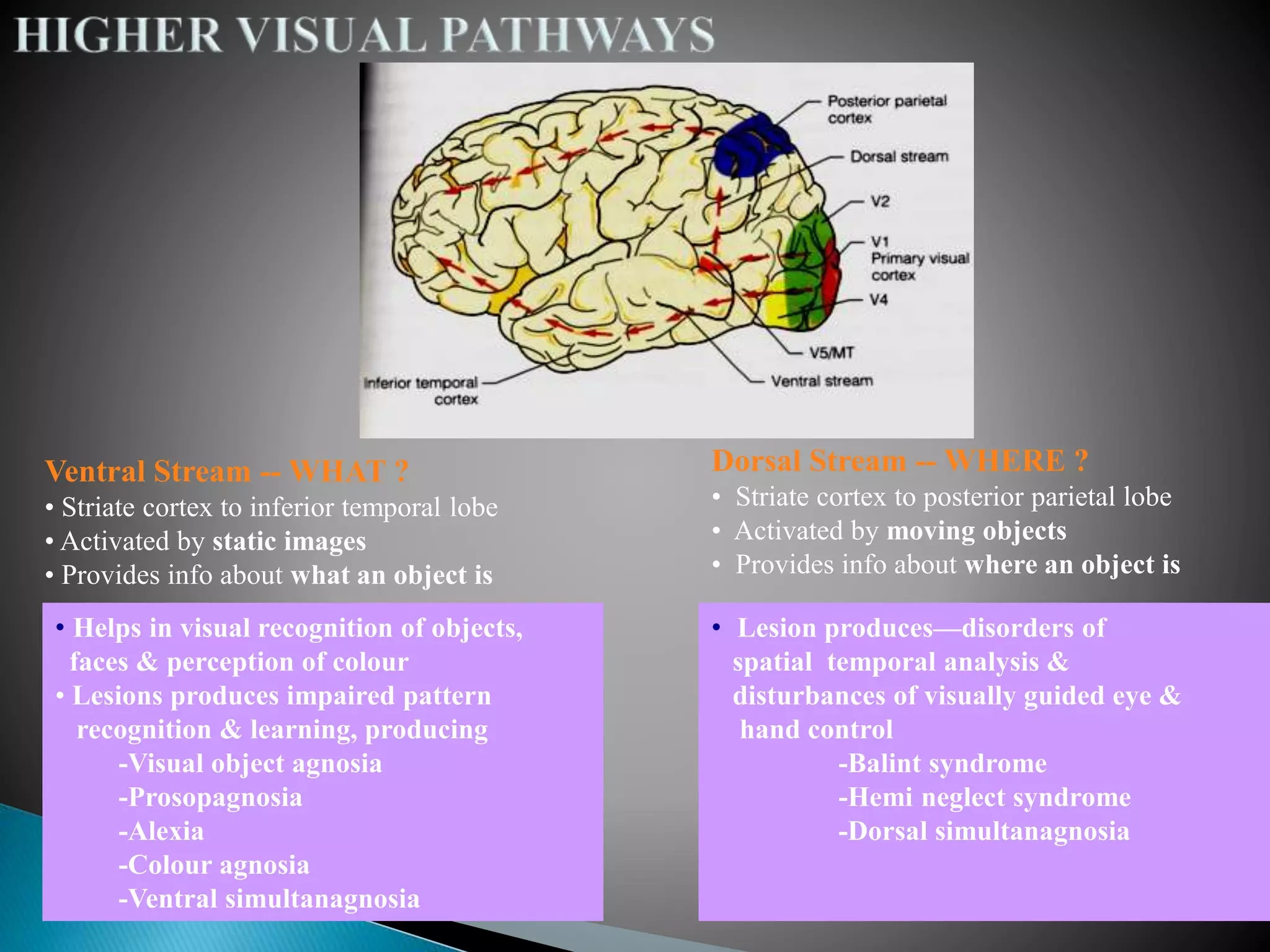




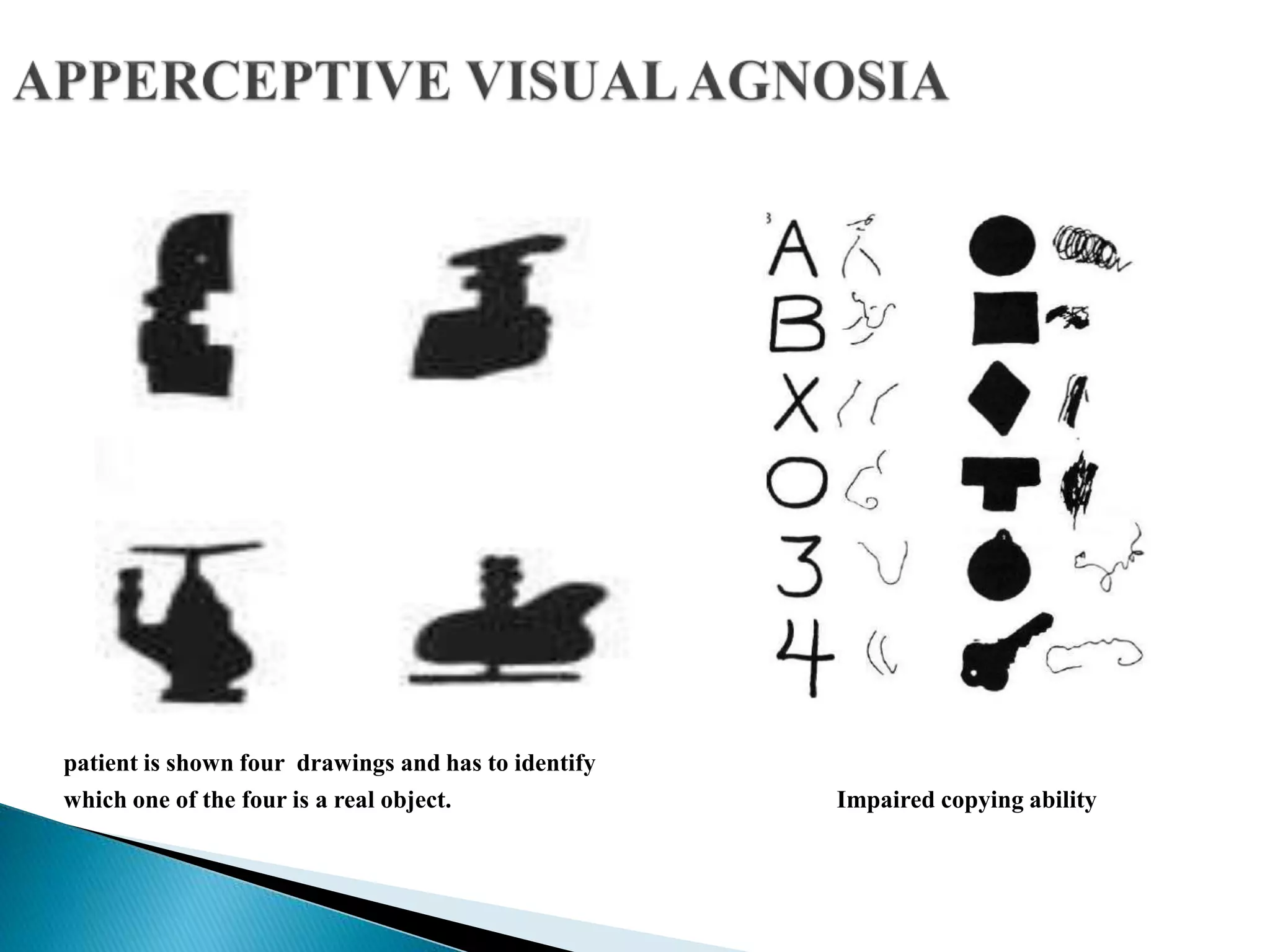












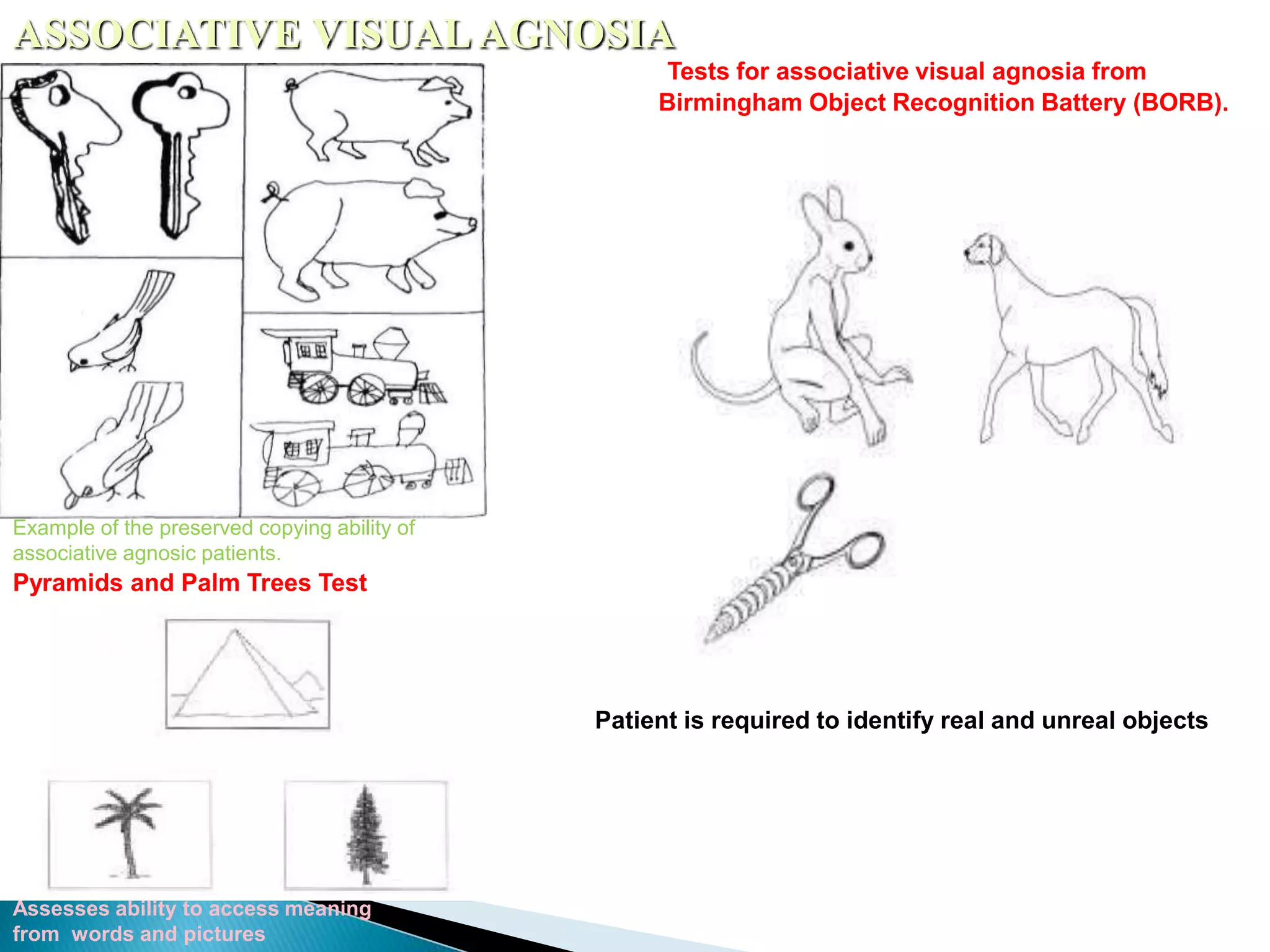










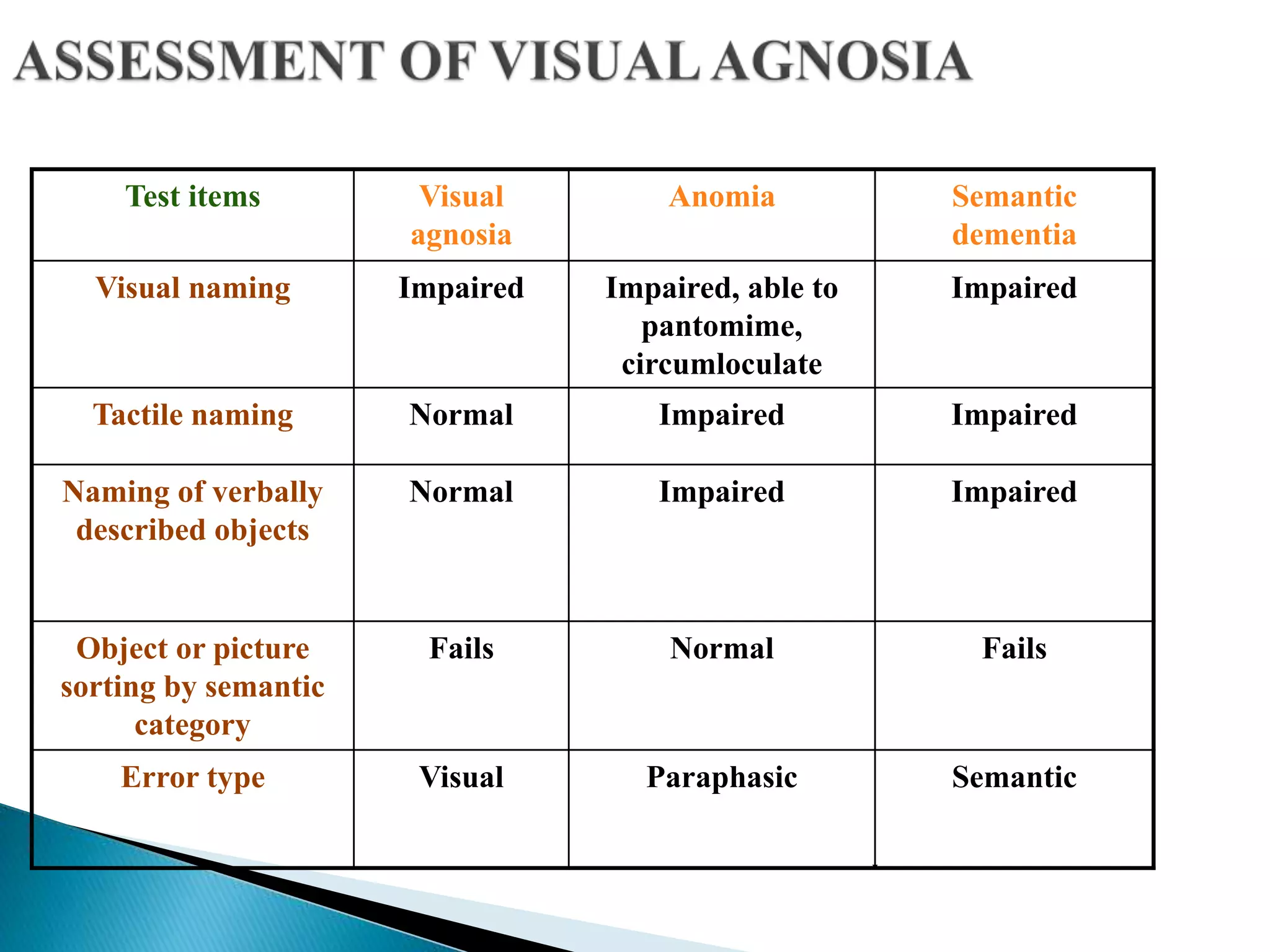















This document discusses various types of agnosia, which are neuropsychological disorders involving the failure to recognize familiar objects despite intact sensory perception and intellectual ability. It describes visual, auditory, tactile, olfactory and gustatory agnosias. Within visual agnosia, it distinguishes apperceptive and associative subtypes and discusses related syndromes like prosopagnosia, simultanagnosia, alexia and color agnosia. It covers the neuroanatomy, assessment and causes of different agnosias.