Downloaded 384 times


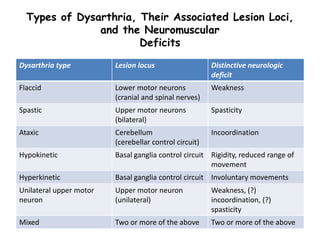
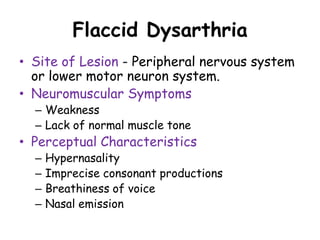

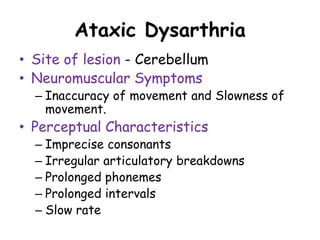
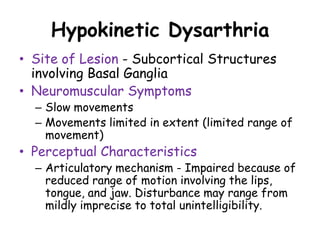
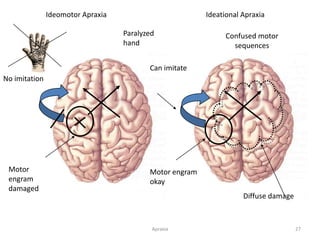
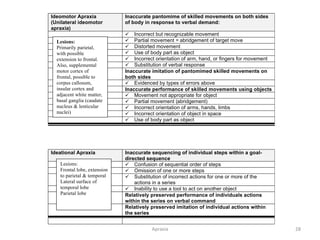
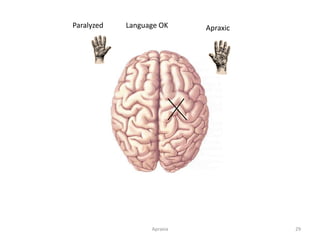
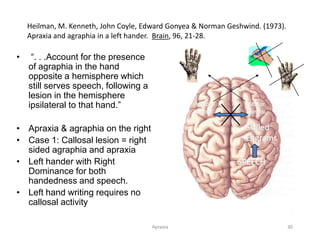

This document provides definitions and descriptions of motor speech disorders. It begins by defining motor speech disorders as resulting from neurological impairment that affects the retrieval, activation, or execution of speech movements. The two main types are described as dysarthria and apraxia. Dysarthria is defined as a group of speech disorders caused by disturbances in muscle control for speech. Various types of dysarthria are outlined based on the site of lesion and perceptual characteristics. Apraxia is defined as a disorder of the planning and programming of speech movements. Causes and characteristics of apraxia are also described.






















































































