Downloaded 88 times







![Deficits of dorsal stream
Disorders of motion perception
-associated with damage to areas of extrastriate visualcortex
analogous to V5.[“OPTIC ATAXIA”]
Disorders of spatial perception
-Balint syndrome
-Dressing apraxia and constructional ‘‘apraxia’’
• Confusingly, these are not apraxias as such, but are rather
visuospatial deficits .](https://image.slidesharecdn.com/agnosiafinalppt-190628030129/75/Agnosia-ppt-13-2048.jpg)









































![AUDITORY NONVERBAL AGNOSIA Meaningful non-verbal sounds
– cannot identify
Pure –tone hearing - preserved
Language comprehension –
preserved
B/L temporal lobe lesions
PHONOSOGNOSIA Recognition of familiar voices –
impaired
Emotional intonation of speech
– cannot percieve [auditory
affective agnosia]
Right parietal lesion](https://image.slidesharecdn.com/agnosiafinalppt-190628030129/75/Agnosia-ppt-70-2048.jpg)









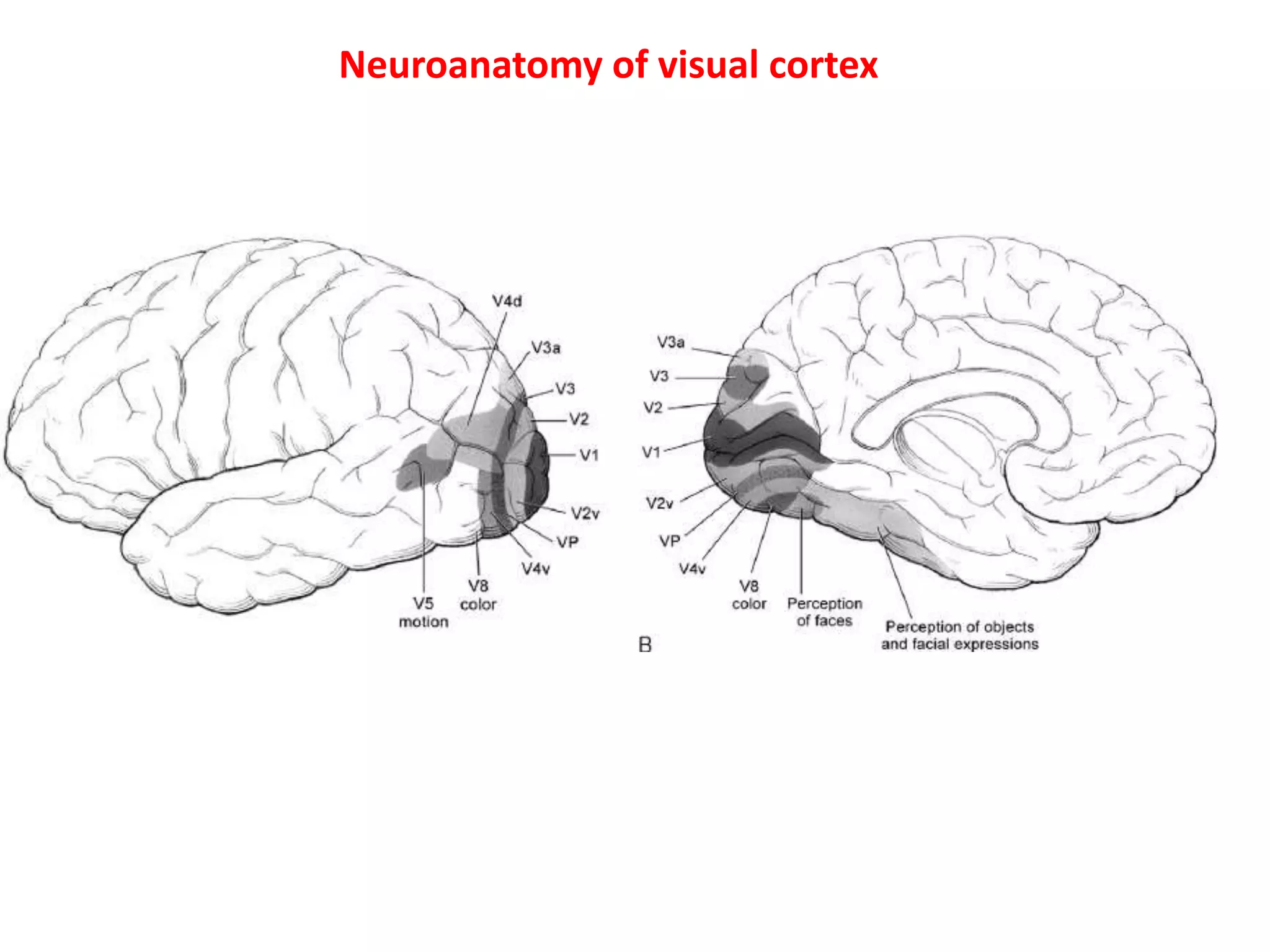
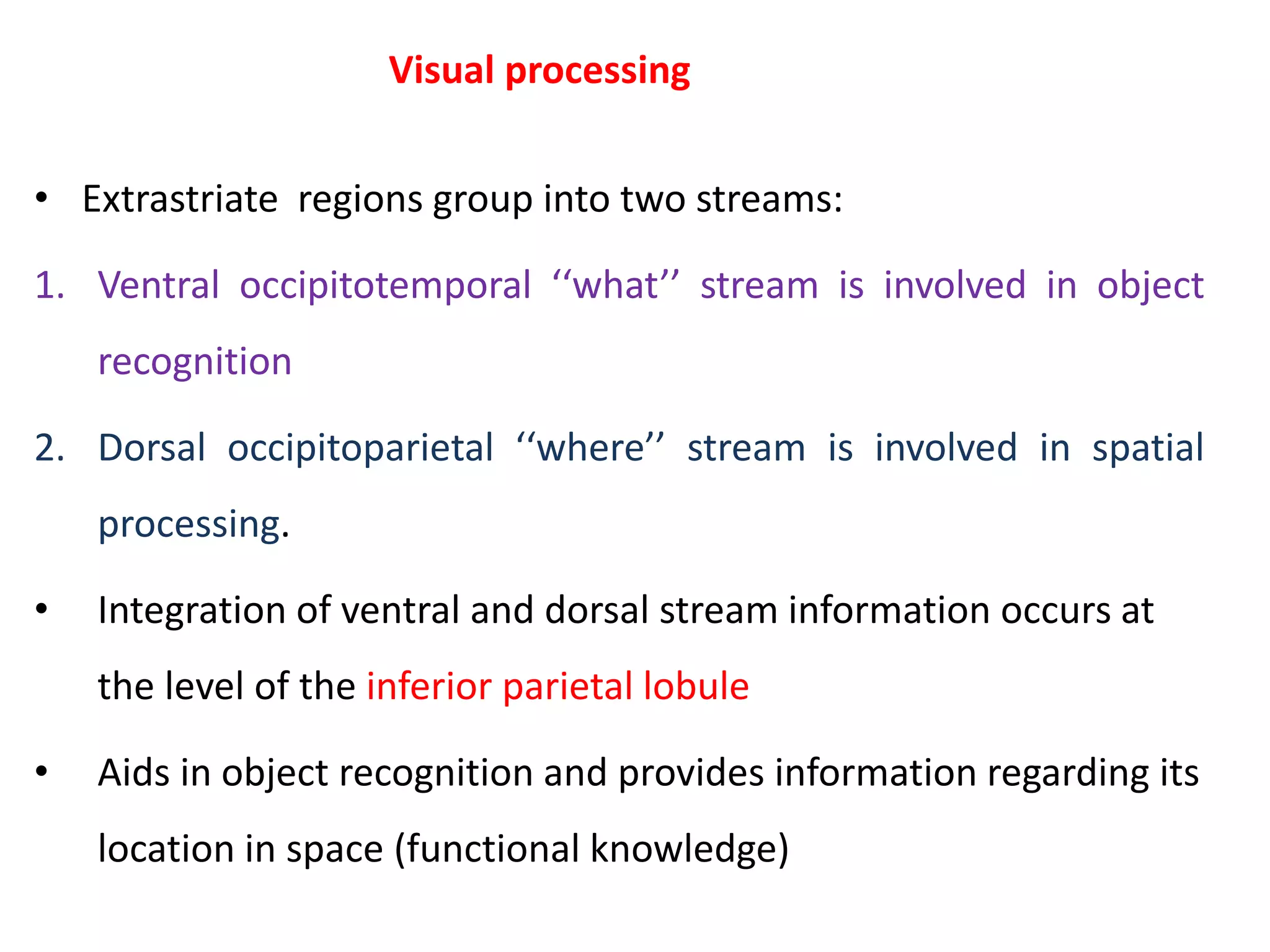
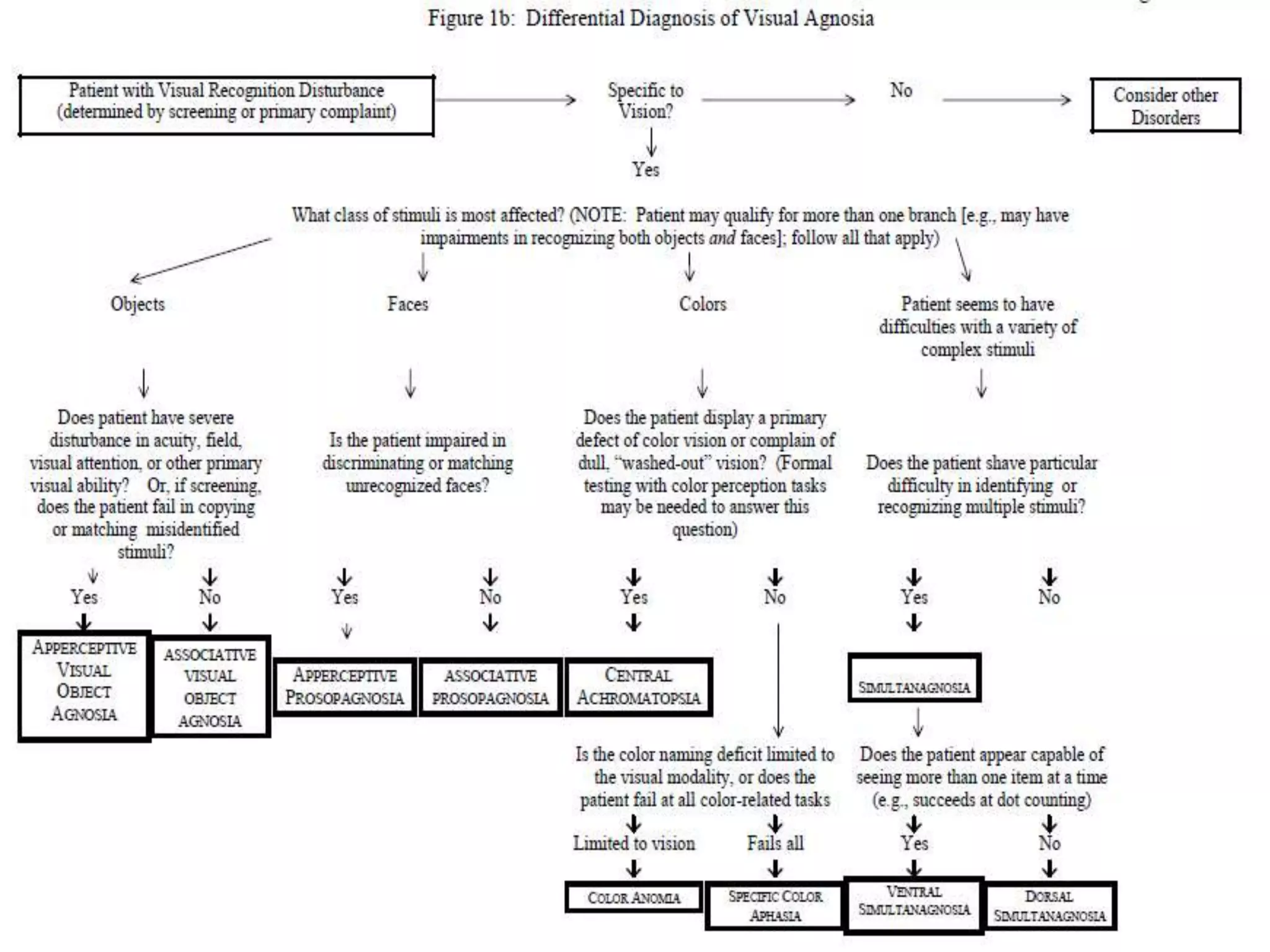
This document discusses different types of agnosia, which are disorders that cause inability to recognize sensory stimuli despite normal sensory perception. It defines agnosia and describes its classification into visual, auditory and tactile modalities. It provides details on visual processing pathways and disorders of the ventral "what" and dorsal "where" streams. Specific visual agnosias discussed include apperceptive, associative, integrative, prosopagnosia, color agnosia and simultanagnosia. Neuroanatomical bases and diagnostic criteria for each are outlined.
Defines agnosia, its meaning, symptoms, and historical context. Highlights classifications and characteristics.
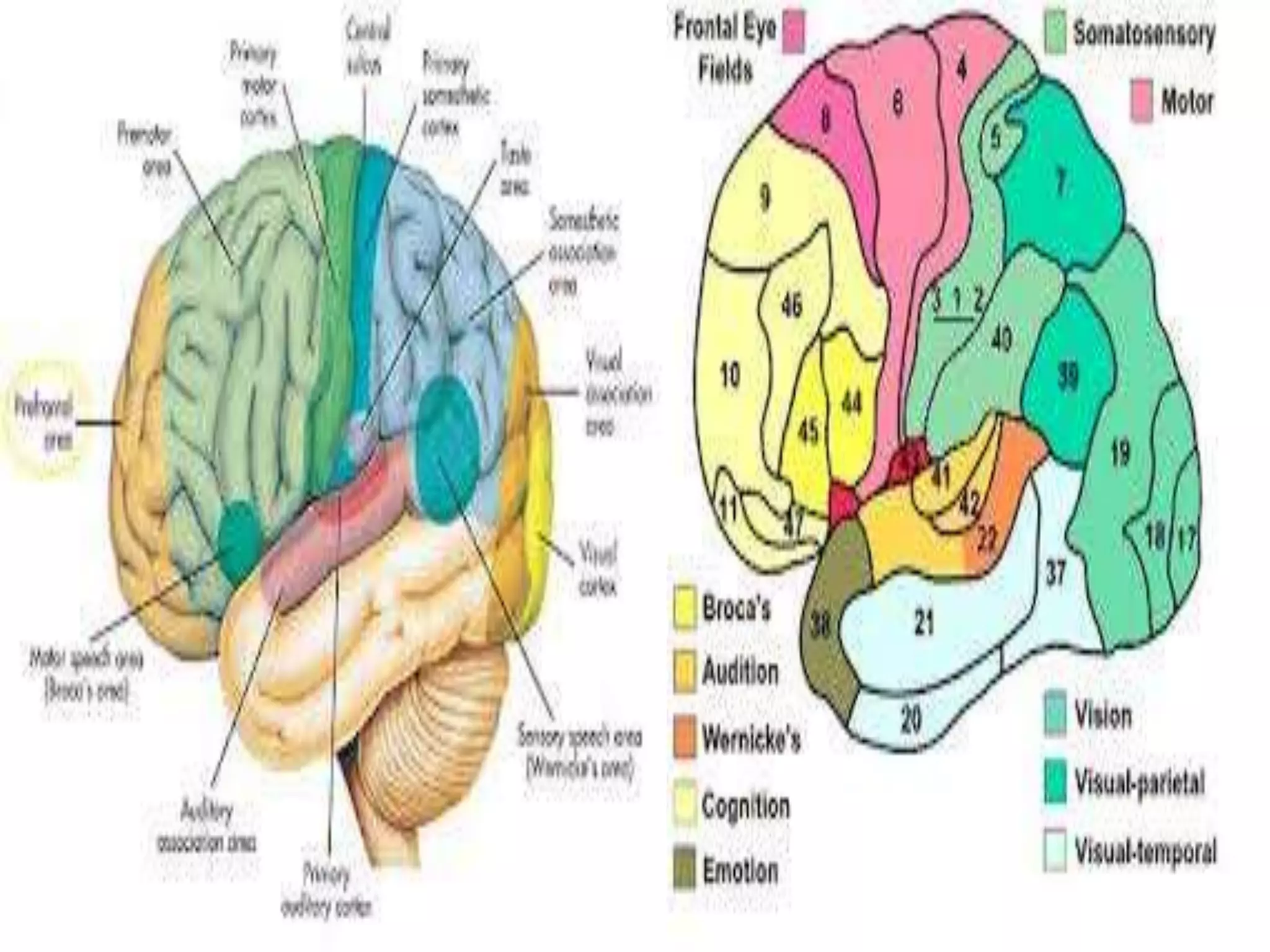
Discusses classifications of agnosias by modalities: visual, auditory, and tactile. Elaborates on visual agnosias. Describes specific disorders arising from visual processing issues, including Alexia and different types of agnosia.
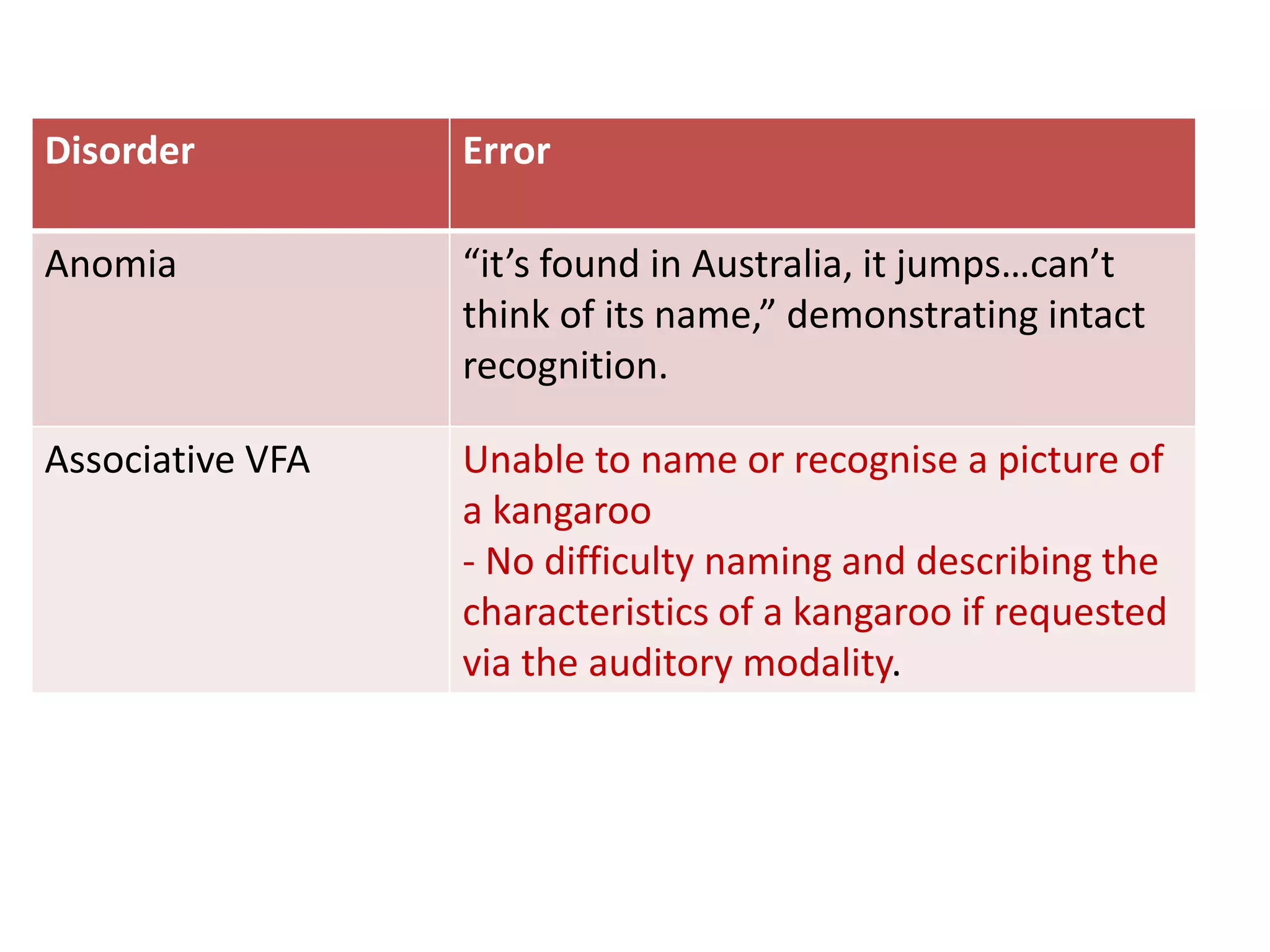
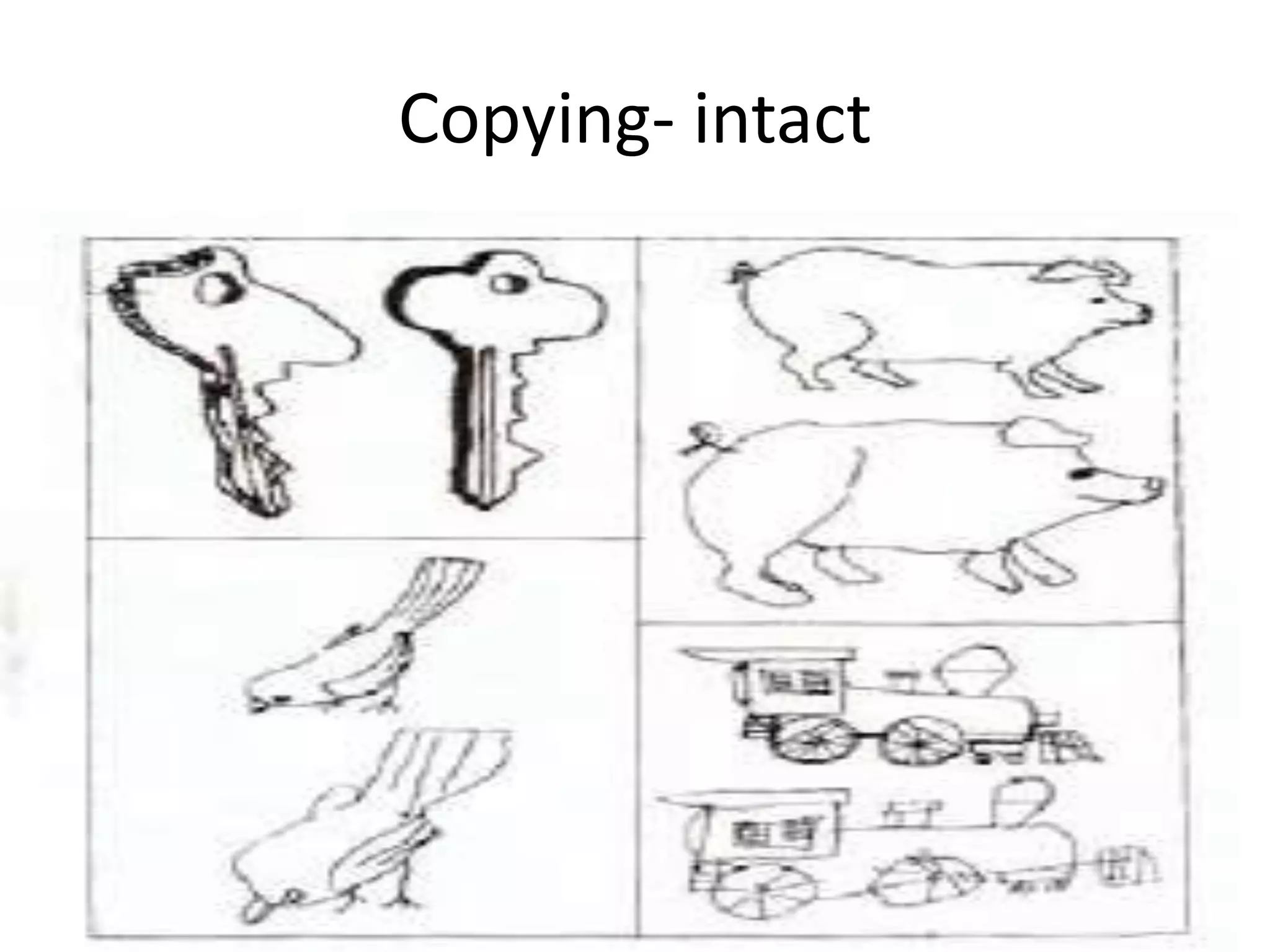
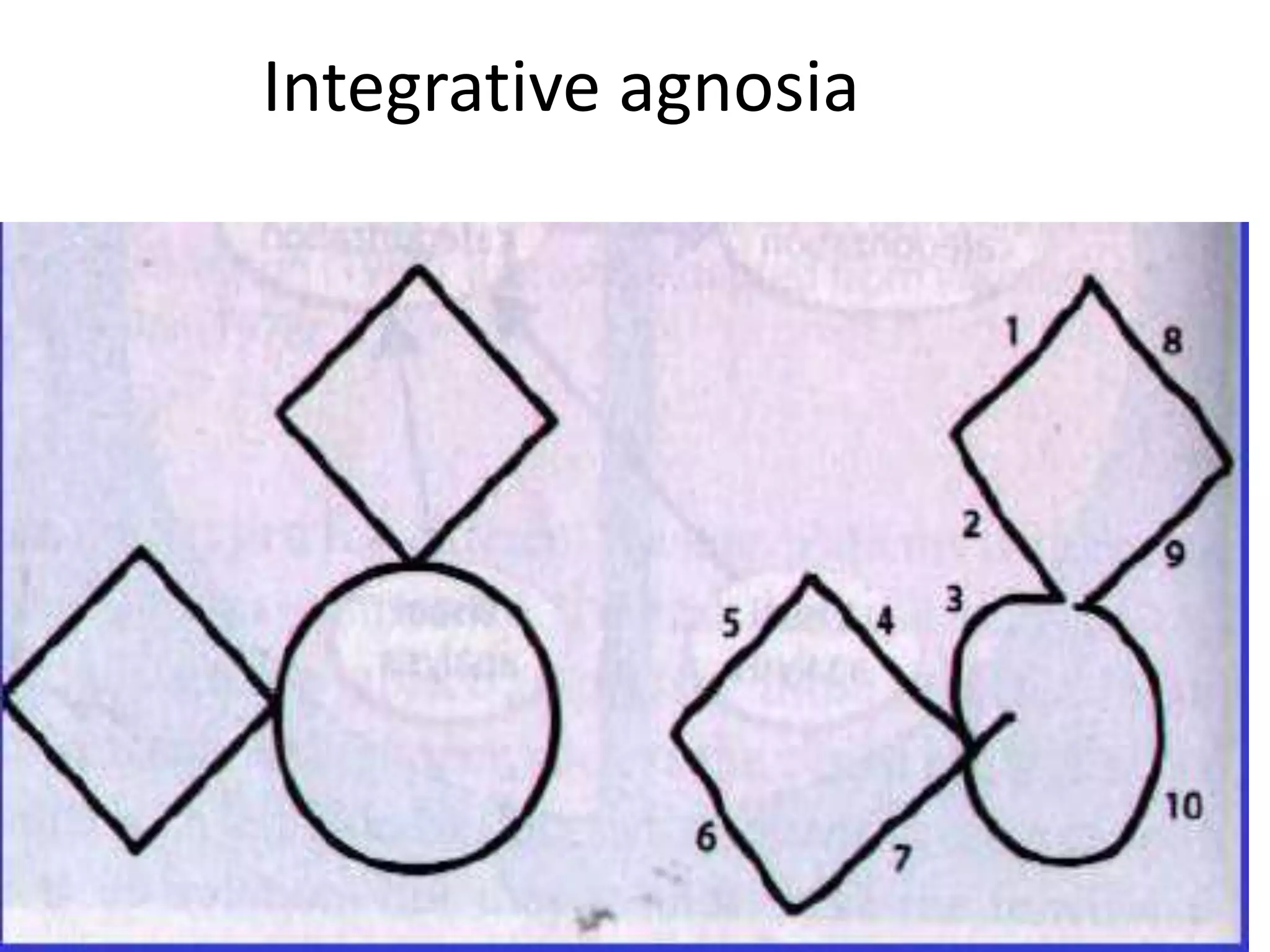
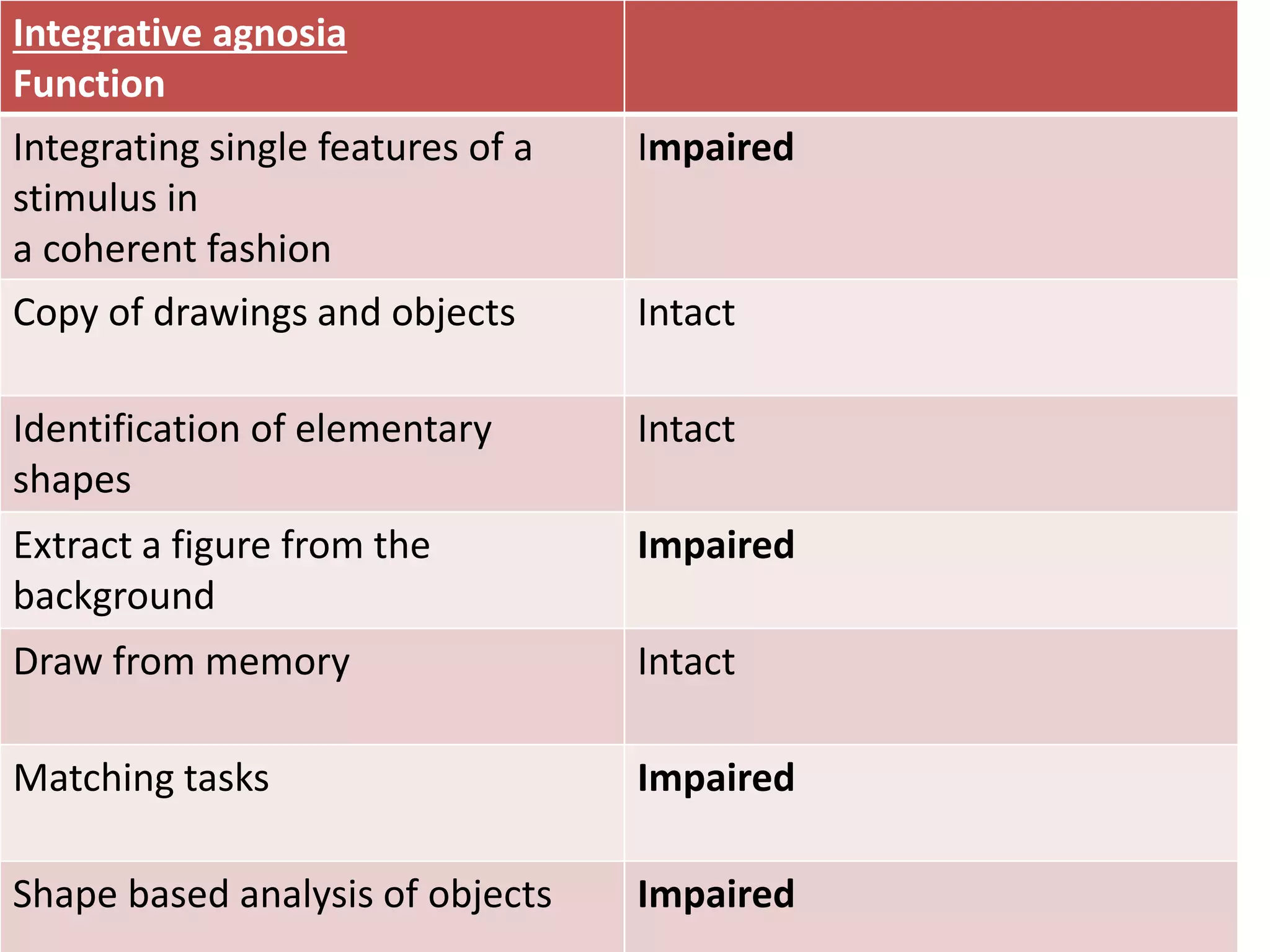
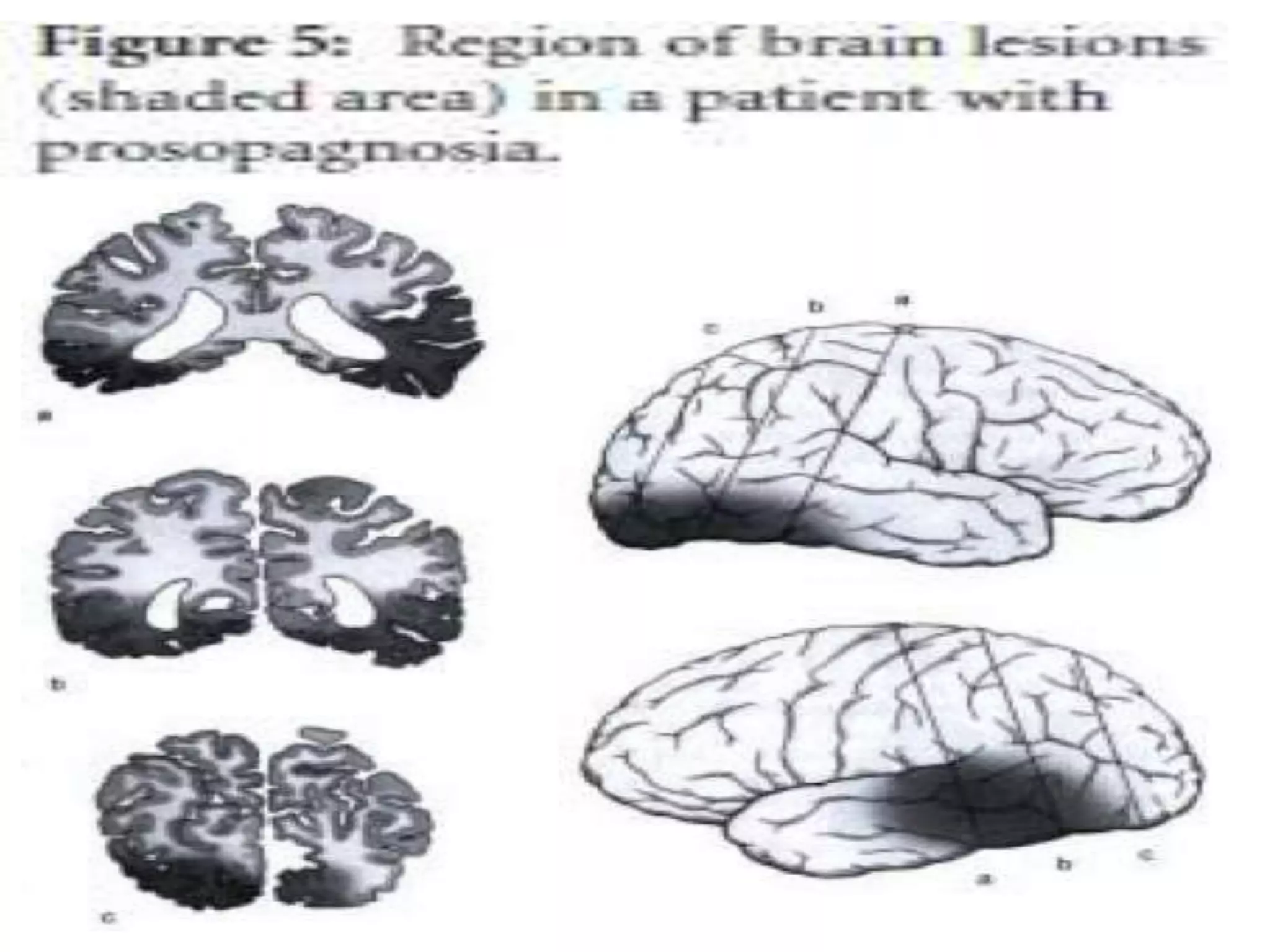
Outlines clinical features of associative visual agnosia, apperceptive agnosia, and integrates testing methods.Explains integrative agnosia and prosopagnosia, detailing their characteristics and recognition challenges.
Explains Simultanagnosia, types, and Balint’s syndrome, including symptoms and effects on recognition.Details finger agnosia and color agnosia, explaining symptoms and localization of underlying issues.
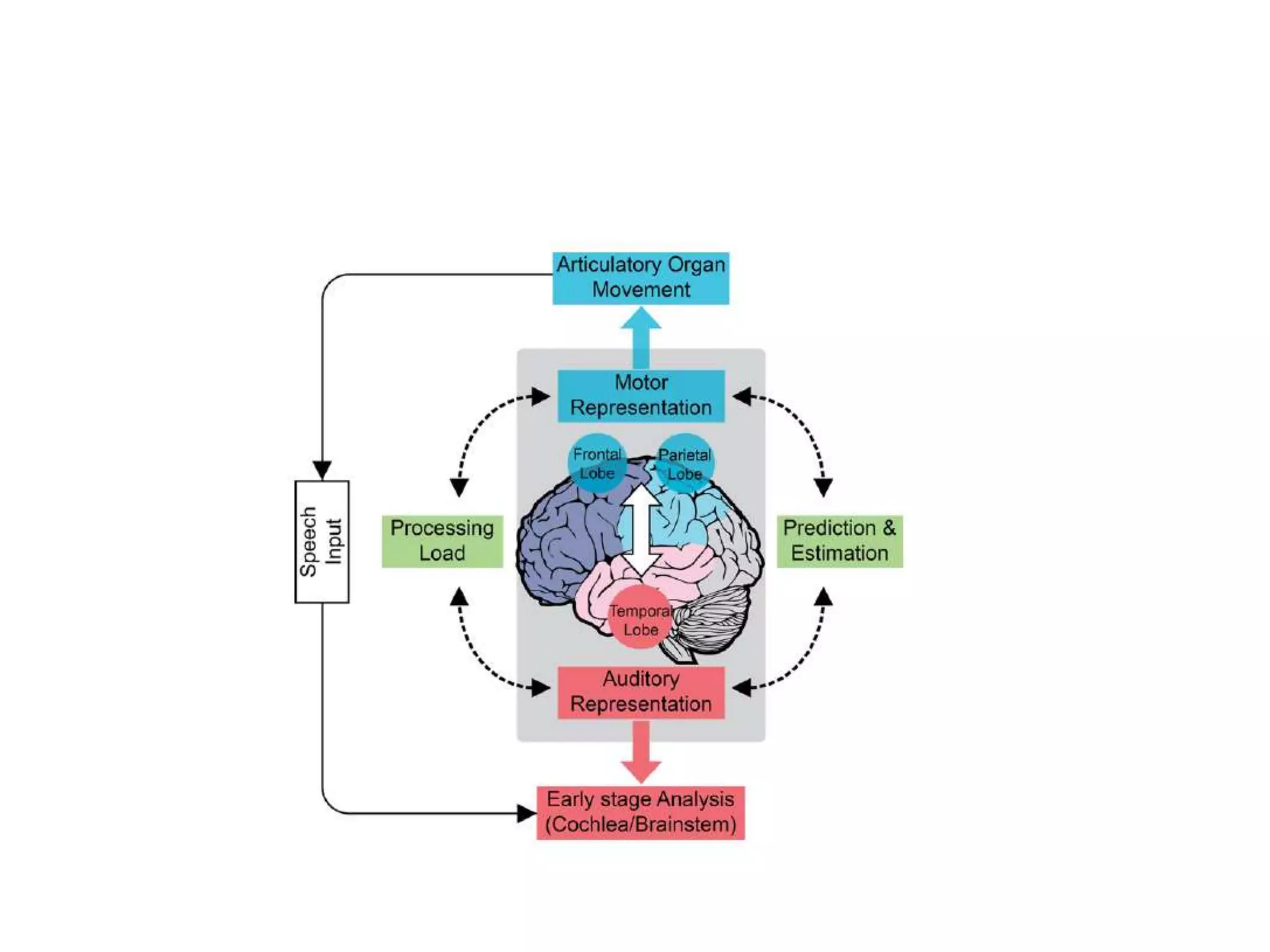
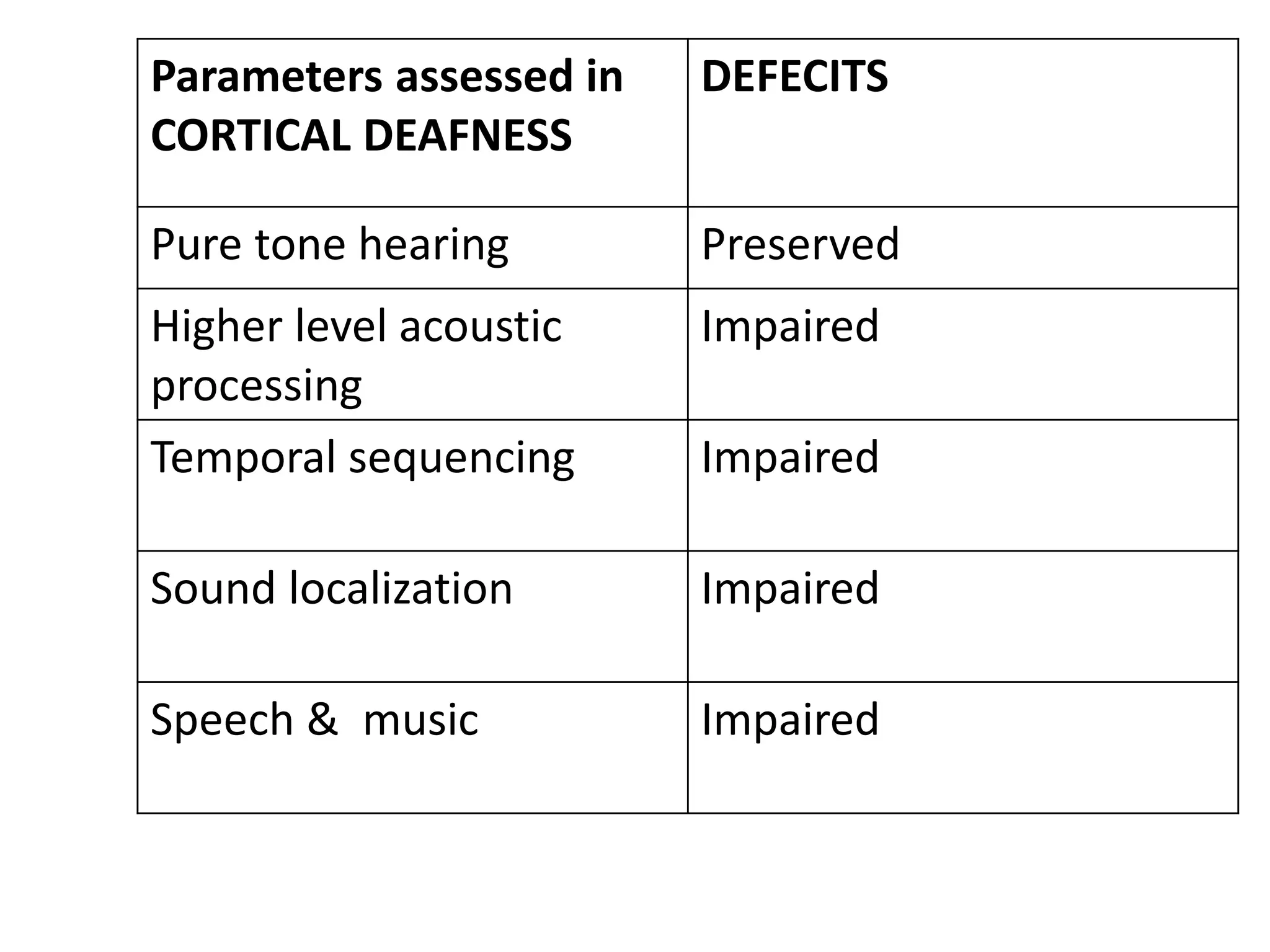
Defines optic aphasia and auditory agnosias, discussing features and impairments related to auditory stimuli.
Reviews tactile agnosias, clinical assessments for various types, and unique syndromes such as Anton’s syndrome.
Concludes the discussion on agnosias, summarizing key points and thanking the audience.