Downloaded 96 times
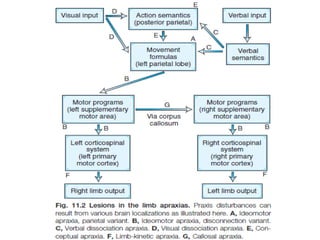


Apraxia is an inability to correctly perform learned skilled movements as a result of damage to the brain regions involved in motor planning and programming. There are two main types - ideomotor apraxia which affects pantomiming and imitating gestures on command, and ideational apraxia which affects the sequencing of multi-step actions. Apraxia is assessed using tests of pantomime, imitation, gesture knowledge, and sequencing tasks. The underlying causes and neuroanatomical correlates of different apraxic syndromes provide insight into the neural systems supporting skilled voluntary movement.























































































