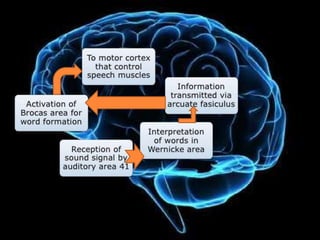
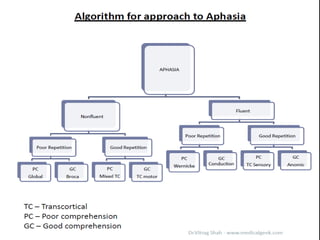
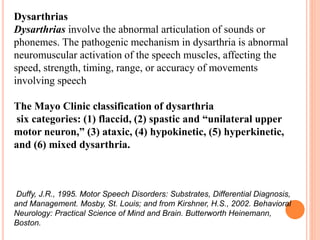
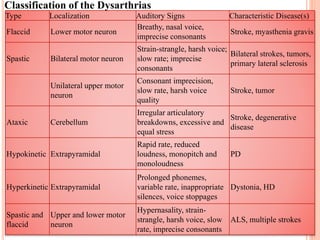
Dr. Surendra Ghintala presented on speech disorders. The presentation covered topics such as external versus inner speech, the central language zones of the brain including the receptive and executive areas, the anatomy of language functions, and the components and structure of language including phonology, morphology, syntax, semantics, and pragmatics. Classification systems for aphasia were discussed including the Boston Aphasia Classification System which recognizes eight subtypes of aphasia. Clinical features of different aphasia syndromes were outlined. Motor speech disorders including apraxia and dysarthria were also covered along with other conditions that can cause aphasia such as dialysis dementia syndrome.