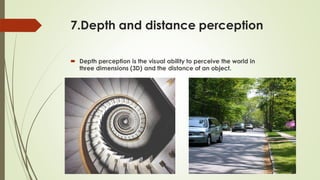
This document discusses various perceptual disorders including body scheme disorders, spatial relation disorders, agnosia, and apraxia. Body scheme disorders include unilateral neglect, anosognosia, somatoagnosia, and finger agnosia. Spatial relation disorders involve impairments in figure-ground discrimination, spatial relations, position in space, topographical disorientation, depth and distance perception, and vertical disorientation. Agnosia is an inability to recognize objects, people, or sounds through senses and includes visual agnosia and auditory agnosia. Apraxia is an impairment of voluntary skilled movement and includes ideomotor apraxia and ideational apraxia. Various tests are used to evaluate these conditions including line