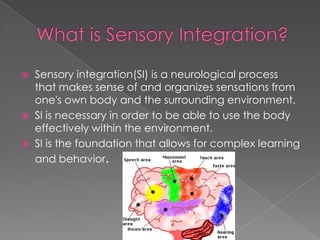
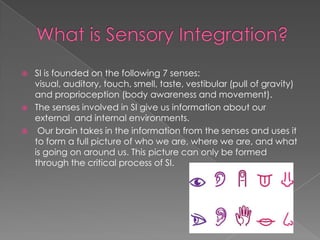
Sensory integration is a neurological process that allows individuals to make sense of sensations from their body and environment. Sensory integration disorder occurs when this process is not functioning properly, making it difficult for individuals to respond appropriately. Sensory integration therapy aims to stimulate the senses through activities involving movement, touch, sound, and vision to help brains better process sensory information. Research suggests this therapy can help brains of children with sensory integration disorder change and develop through rich sensory experiences.