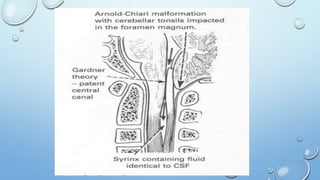
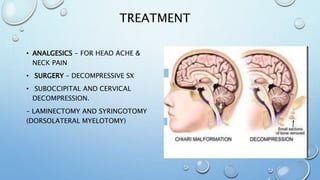
Syringomyelia is a condition where a cyst, called a syrinx, develops in the spinal cord. It most commonly affects the lower cervical spine. It is often associated with abnormalities of the skull or spinal column. The majority of cases are linked to Chiari malformation type 1, where the cerebellar tonsils are displaced into the spinal canal. Symptoms vary depending on the location of the syrinx but can include pain, loss of sensation, muscle weakness or atrophy, and autonomic dysfunction. Diagnosis is made using imaging like MRI. Treatment involves surgery to decompress pressure on the spinal cord like laminectomy with the goal of resolving the syrinx.