Downloaded 20 times
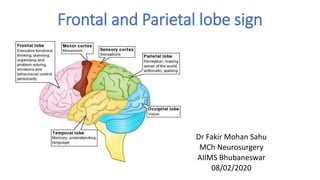
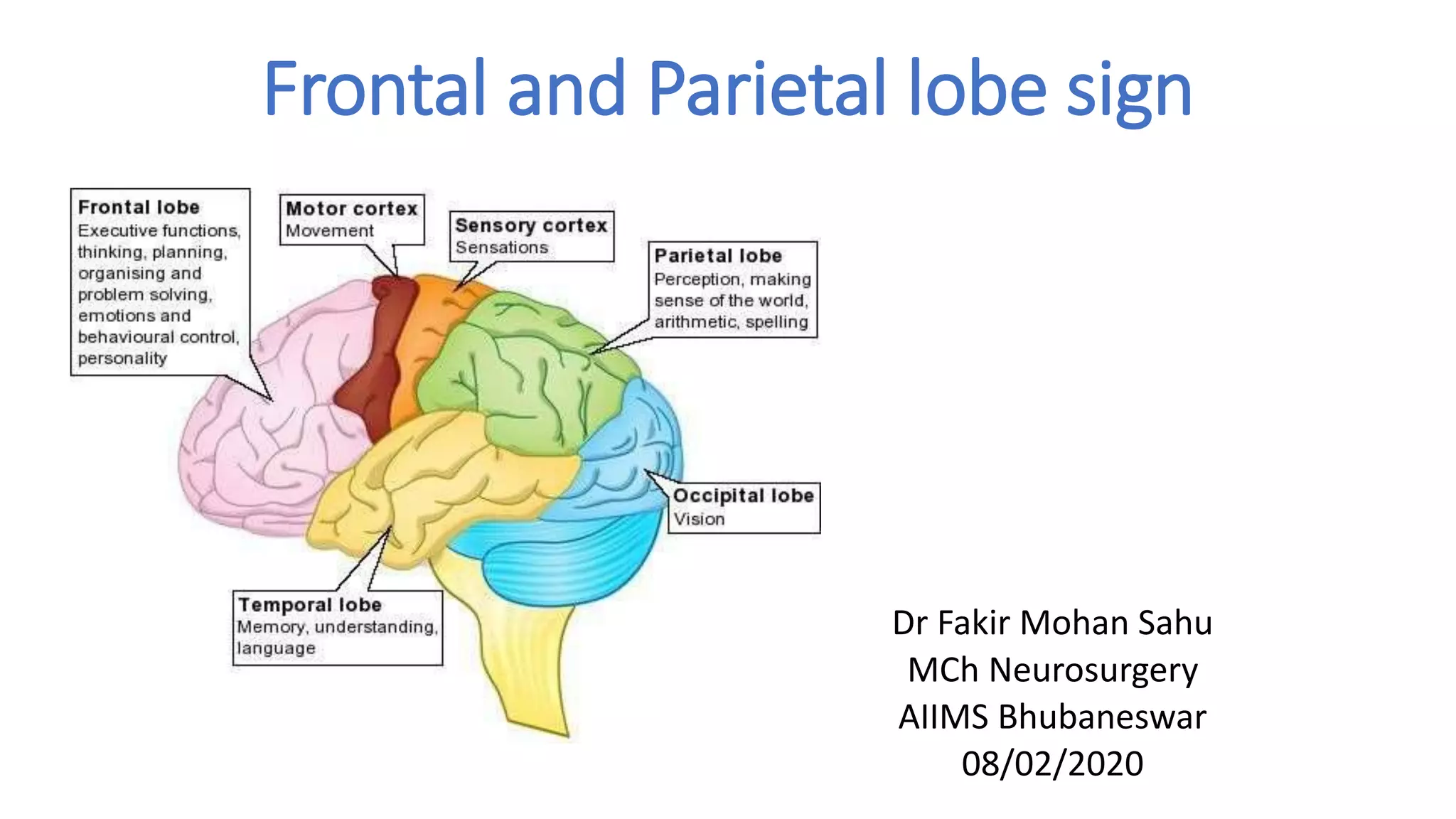
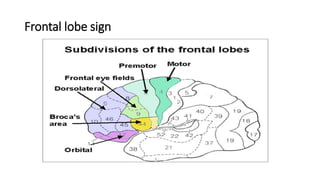
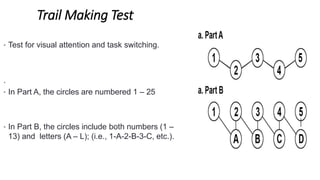
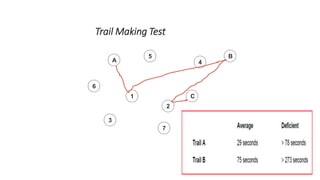

1) The document discusses signs associated with lesions in the frontal and parietal lobes. Tests are described to assess functions localized to these regions like motor skills, memory, attention, and language abilities. 2) Parietal lobe signs include sensory deficits, agnosias like finger agnosia, and apraxias involving how to complete tasks. Tests evaluate two-point discrimination, graphesthesia, and stereognosis. 3) Both lobes are involved in executive functions and attention. Tests mentioned include the Wisconsin Card Sorting Test, Trail Making Test, and Stroop Test.





































































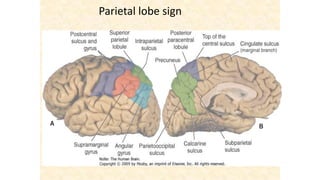
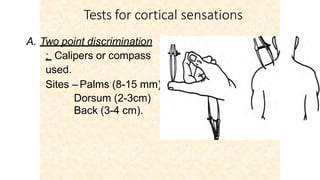
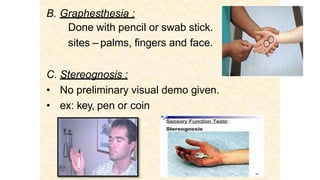
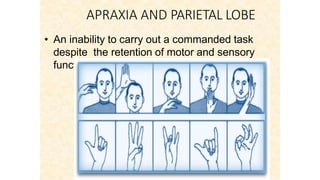
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















