INTRODUCTION
• The frontallobe is one of the four major lobes of
the cerebral cortex.
• Located at the front of each cerebral hemisphere and
positioned anterior to parietal lobe.
• Superior and anterior to the Temporal lobes.
• Separated from the parietal lobe by a space between
tissues called the central sulcus.
• Separated from the temporal lobe by a deep fold called the
lateral (Sylvian) sulcus.
3.
• The precentralgyrus, forming the posterior border of the
frontal lobe, contains the primary motor cortex, which
controls voluntary movements of specific body parts.
• In humans, the frontal lobe reaches full maturity around the
late 20s (Giedd et al., 1999)
• A small amount of atrophy, however, is normal in the aging
person’s frontal lobe.
• A decline in frontal lobe volume of approximately .5% every
year seemed to be average. (Fjell, 2009)
• These findings corroborate those of Coffey, who in 1992
indicated that the frontal lobe decreases in volume
approximately 0.5%-1% per year.
STRUCTURE OF FRONTALLOBE
• On the lateral surface of the human brain, the central
sulcus separates the frontal lobe from the parietal lobe.
• The lateral sulcus separates the frontal lobe from
the temporal lobe.
• The frontal lobe bottom can be divided into a
• lateral,
• polar,
• orbital (above the orbit; also called basal or ventral), and
• medial part.
7.
• Each ofthese parts consists of particular gyri and the gyri
are separated by sulci
• Lateral part: Precentral gyrus, lateral part of
the superior frontal gyrus, middle frontal gyrus, inferior
frontal gyrus.
• Polar part: Transverse frontopolar gyri, frontomarginal
gyrus.
• Orbital part: Lateral orbital gyrus, anterior orbital
gyrus, posterior orbital gyrus, medial orbital
gyrus, gyrus rectus.
• Medial part: Medial part of the superior frontal
gyrus, cingulate gyrus.
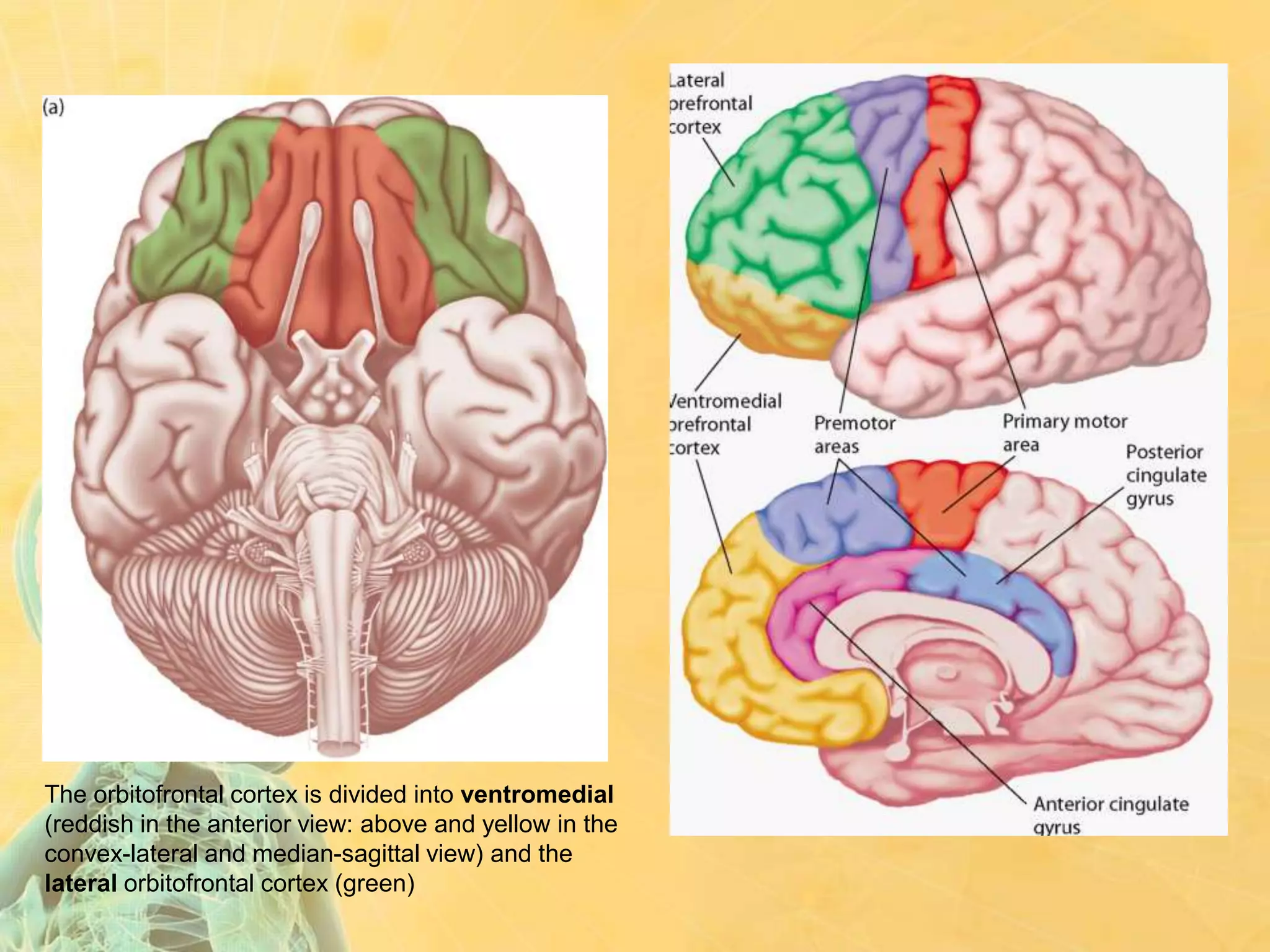
The orbitofrontal cortexis divided into ventromedial
(reddish in the anterior view: above and yellow in the
convex-lateral and median-sagittal view) and the
lateral orbitofrontal cortex (green)
11.
BLOOD SUPPLY ofFL – MCA and ACA
• The middle cerebral artery (MCA) is one of the three
major paired arteries that supply blood to the cerebrum.
• The MCA arises from the internal carotid and continues
into the lateral sulcus where it then branches and
projects to many parts of the lateral cerebral cortex.
• To the frontal lobe, it gives off 4 branches -
• Lateral frontobasal (orbitiofrontal)
• Prefrontal arteries
• Pre-Rolandic artery (precentral)
• Rolandic arteries (central)
14.
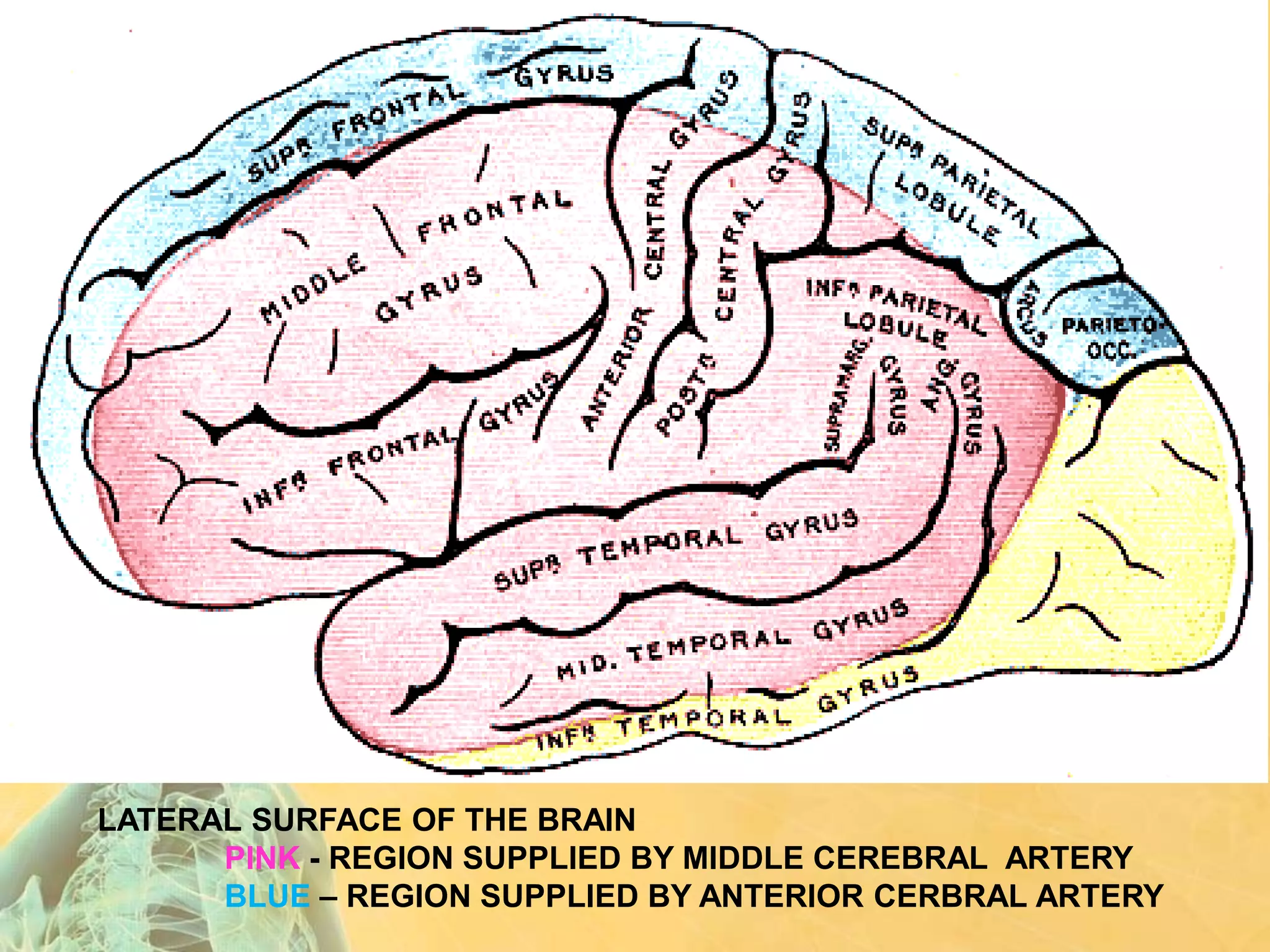
• The anteriorcerebral artery (ACA) is one of a pair of
arteries on the brain that supplies oxygenated blood to
most medial portions of the frontal lobes and superior
medial parietal lobes.
• The two anterior cerebral arteries arise from the internal
carotid artery and are part of the Circle of Willis.
• The ACA supplies the frontal lobe in the following areas –
- The medial surface of the frontal lobe by the medial
orbito-frontal artery.
- Approximately 1 inch of the lateral surfaces of FL
• Cytoarchitecture (Greekκύτος= "cell" + αρχιτεκτονική=
"architecture"), also known as cytoarchitectonics, is the
study of the cellular composition of the body's tissues under
the microscope.
• Refers to the arrangement and characteristic organization
of neuronal cell bodies in the brain and spinal cord.
• The birth of the cytoarchitectonics of the human cerebral
cortex is credited to the Viennese psychiatrist Theodor
Meynert (1833-1892)
19.
• Korbinian Brodmann(1868-1918) in Berlin, working on
the brains of diverse mammalian species, developed a
division of the cerebral cortex into 52 discrete areas (of
which 44 in the human, and the remaining 8 in non-human
primate brain.
20.
BROCA’S AREA
• Broca'sarea or the Broca area is a region in the frontal lobe of
one hemisphere (usually the left), named after Pierre Paul Broca.
• Broca's area in the left hemisphere and its homologue in the
right hemisphere are designations usually used to refer to pars
triangularis (PTr) and pars opercularis (POp) of the inferior
frontal gyrus.
• Represented in Brodmann's cytoarchitectonic map as
areas 44 and 45 of the dominant hemisphere.
• Leborgne was a patient of Broca's. Almost completely unable to
produce any words or phrases, he was able to repetitively produce
only the word tan. Lelong was another patient of Broca's. He also
exhibited reduced productive speech. He could only say five words,
'yes,' 'no,' 'three,' 'always,' and 'lelo'
21.
FUNCTIONS OF BROCA’sarea
• Language production and language comprehension/use syntax to determine
meaning of sentences.
• Plays a role in interpreting action of others – Action recognition and
production.
• Speech-associated gestures could possibly reduce lexical or sentential
ambiguity, comprehension should improve in the presence of speech-
associated gestures. As a result of improved comprehension, the involvement
of Broca's area should be reduced
22.
FRONTAL-SUBCORTICAL CIRCUITS
• Thereare 5 parallel, separate circuits (Alexander et
al, 1986)
1. a motor circuit originating in the motor cortex and
pre-motor cortex
2. an oculomotor unit originating in the frontal eye
fields
3. the dorsolateral prefrontal circuit, which underpins
executive functions
4. the anterior cingulate circuit which underpins
motivation
5. the orbitofrontal circuit which underpins impulse
control and social behavior.
Neurology
Psychiatry
Functional regions ofthe frontal lobes
I. Primary motor area
II. Premotor area
III. Frontal eye fields
IV. Dorsolateral prefrontal cortex
V. Orbital and basal areas
VI. Supplementary motor area and anterior cingulate gyrus
area
29.
I. Primary motorarea
• Brodmann area 4
• Input from ventral lateral
thalamic nucleus, primary
somatosensory area in
parietal lobe
• Output to internal capsule
• Pyramidal motor functions
• Although designated a
“motor” cortex, this area is
also involved with
somatosensory perception
30.
CORTICAL HOMUNCULUS (Primarymotor)
• A cortical homunculus is a pictorial representation of
the anatomical divisions of the primary motor cortex.
31.
Primary motor dysfunction
•Initially flacid hemiparesis or
hemiplegia on contralateral
side
• Later spastic hemiparesis or
hemiplegia
32.
Bedside tests forPrimary motor cortex:
1. Motor strength of hand grip -
The patient is asked to grip the examiners fingers.
• Strength should be roughly equal, with greater strength on
the dominant side.
• It should be difficult for the examiner to free her/his fingers.
2. Motor speed as in finger tapping has also been listed as a
useful test (Malloy & Richardson, 1994) but such tests do not
discriminate from the premotor cortex.
• Diagnostically, poor performances suggest local lesions
such as vascular or neoplastic pathology, or
• a generalized lesion such as a degenerative disease.
(Peripheral nerve lesion must, of course, be excluded.)
33.
II. Premotor area
•Brodmann area 6
• Input from ventral anterior
thalamic nucleus and secondary
somatosensory area
• Output to motor area and
connections via corpus callosum
to contralateral premotor area
• Integration of sensory and motor
information
• Praxis
34.
Premotor dysfunction
• Apraxia
•Preserved postural praxis via
basal ganglia
• Contralateral fine motor
deficits
• Difficulty using sensory
feedback
35.
Bedside tests forpremotor cortex:
1. Sensorimotor abilities are tested by asking the patient
touch each finger to the thumb in succession as rapidly
as possible. Watch for speed and dexterity.
2. Apraxia can be tested by asking the patient to "blow a
kiss" / demonstrate the use of a shovel / draw a cube /
draw a star / light a cigarette etc.
Poor performance carries the diagnostic implications as for
the motor cortex above. (i.e. the area is affected by
vascular insult/neoplasm)
36.
EFFECTS of LESIONSAFFECTING BOTH Primary motor
and Premotor cortex
• Motor – Contralateral spastic paresis; loss of fine motor
control
• Reduced verbal fluency
• Impaired spelling
• Others effects – (GROUPS)
1. Gegenhalten/Paratonia
2. Primitive reflexes (grasp/sucking/palmar-
mental/glabellar tap)
3. Optic atrophy (Ipsilateral)
4. Urinary incontinence
5. Perseveration
6. Seizures (Jacksonian)
37.
III. Frontal eyefield
• Brodmann area 8 (posterior
portion of middle frontal gyrus),
with some area 9 and 6
• Volitional eye movement in
contralateral visual field
• Active visual search
• Voluntary eye movements are of
two types -
• Pursuit movement occurs when
the eyes to follow moving
objects.
• Saccadic eye movements are
used to follow imaginary points.
38.
Frontal eye fielddysfunction
• Failure to move eyes
volitionally to contralateral
visual field
• Intact passive eye
movement
• Poor visual search
39.
Bedside test forfrontal eye field:
1. Ask the patient to follow the movement of a finger from
left to right and up and down.
2. Ask the patient to look from left to right, up and down (with
no finger to follow).
• Note inability to move or jerky movement.
• Brodmann areas46,45,47,8,9,10. A compromise position is that the
DLPFC is composed of Brodmann area 9 and the lateral aspect of 10
and most of area 46.
• Executive functions - (“Executive” in frontal lobe means cognitive
system that controls and manages other cognitive processes. )
• Integration of multimodal sensory information
• Generation of multiple reponse alternatives to environmental
challenges
• Selection of most appropriate response, self evaluation of
responses and selection of a replacement response if first response
fails
• Maintenance of task set, persistence
• Sequential ordering of data
• Set shifting, flexibility
• Spatial working memory
FUNCTIONS OF DLPFC
42.
• The executivefunctions largely determine the ability of the
individual to cope with the continuous, but ever changing
challenges of the environment.
• Thus, the patient’s ability to make an appointment and to
arrive on time is valuable information.
• So too,is the ability of the patient to give a comprehensive
account of her/himself and the reasons for the
consultation.
• It is believed by some authors that formal thought disorder
arises from a lack of executive planning and editing
(McGrath, 1991).
• In thought disorder there are frequent examples of failure
to maintain set (distractibility), sequentially order
information, and to ensure that the listener is
comprehending.
Note - formal thought disorder is also known to involve the left superior temporal sulcus
and the left temporal pole (Horn et al, 2010).
43.
Dorsolateral PFC dysfunction
•Difficulty integrating sensory
information
• Generation of few,
stereotyped response
alternatives
• Poor judgement in response
selection
• Impersistence
• Perseveration
44.
• Head injuryand dementing illnesses may result in severe
impairment of the executive functions.
• Schizophrenia often has thought disorder as a major
feature and the executive functions tests are usually also
affected.
• Depressive disorder may be associated with poor
performance on verbal fluency tests during the acute
phase, which normalizes with remission (Trichard, et al.,
1995).
45.
Bedside tests forDLPFC:
1. Is the patient able to make an appointment and arrive on time?
2. Is the patient able to give a coherent account of current problems and
the reason for the interview? Is there evidence of thought disorder?
3. Digit span, days of the week or months of the year backwards. Here
the patient has to retain the task and simultaneously manipulate
information.
4. Controlled oral word association test (COWAT): the patient is
asked to produce as many words as possible, in one minute, starting
with F,then A, then S. Proper nouns and previously used words with a
different suffix are prohibited (Benton, 1968).
5. Other categorical fluency tests include naming animals, fruits and
vegetables (Monsch et al, 1992).
46.
6. Alternating handsequences. These can be devised by the examiner.
One example is that one hand is placed palm upwards and the other is place
palm downwards, and the patient is then asked to reverse these positions as
rapidly as possible.
Another example is that the backs of the hands are both placed downwards,
but one hand is clenched and the other is open, then the patients is asked to
close the open hand and open the closed hand, and keep reversing the posture
of the hands as rapidly as possible.
A final example is that the patient taps twice with one fist and once with the
other, then after the rhythm is established, the patient is asked to change over
the number of beats (the fist which first tapped twice now taps only once).
Patients with frontal lobe deficits usually perform poorly on these tests, often
being unable to follow the relatively simple instructions
7. Formal neuropsychological may be necessary where uncertainty remains.
Commonly employed tests include Controlled Oral Word Association Test
(Benton, 1968) and the Wisconsin Card Sorting Tests (Heaton, 1985).
V. Orbital andBasal areas
• Brodman areas 10,11,12,13,14
• Input from limbic and olfactory
systems (amygdala, temporal
pole, entorhinal cortex,
olfactory nerve); inferotemporal
lobe areas, ventral visual
pathways
• Output to autonomic
musculature and endocrine
system (basal forebrain
cholinergic system, caudate,
and autonomic system)
53.
FUNCTIONS OF OFC
•Modulation of affective and social behavior; “...preservation of
behavioral regulation by external stimuli and its dissolution in
the absence of external stimulation.”
• It mediates empathic, civil and socially appropriate behavior
(Mega and Cummings, 1994).
• Working memory for feature information
• Integration of memory and emotional valence
• Smell discrimination
• Much of the personality change described in cases of frontal
lobe injury (Phineas Gage being the most famous) is due to
lesions in this area.
• Patients may become irritable, labile, disinhibited and fail to
respond to the conventions of acceptable social behavior
OFC dysfunction
• Disinhibition,socially inappropriate
behavior
• Failure on feature working memory
tasks
• Anosmia
• Confabulation
• Increased concern about social
behavior and contamination has
been associated with increased
orbitofrontal and caudate
metabolism. This has been reported
with lesions of the globus pallidus
and in obsessive compulsive
disorder.
57.
Bedside tests forOFC:
1. Does the patient dress or behave in a way which suggests lack of
concern with the feelings of others or without concern to accepted
social customs? (Frontal Systems Behavior Scale – FrSBe can be
used)
2. Test sense of smell - coffee, cloves etc. (UPSIT can be used)
3. Go/no-go Test. The patient is asked to make a response to one
signal (the Go signal) and not to respond to another signal (the no-go
signal). The most basic is to ask the patient to tap their knee when the
examiner says, “Go” and to make no response when the examiner
says, “Stop”.
Note - The task may be made more demanding by reversing the
customary meaning of signals. An example is to ask the patient to tap
the knee when the examiner says "Stop" and not to tap when the
examiner says "Go" (Malloy and Richardson, 1994).
58.
4. The StroopTest (Stroop, 1935). This is a
neuropsychological test which examines the ability of the
patient to inhibit responses. Patients are asked to state
the color in which words are printed rather than the words
themselves.
Failure of response inhibition is seen in -
• Head injury, other destructive lesions (including dementing processes)
and schizophrenia.
• Impulse control and personality disorder (particularly of the antisocial
type)
• Depressive disorder may manifest irritability, and has been associated
with poor performance on the Stroop Test (Trichard et al, 1995).
• Obsessive compulsive disorder in which there is excessive concern
and caution is associated with increased metabolism in the
orbitofrontal cortex (which may result from subcortical pathology;
Hampson et al, 2012).
Prefrontal region andits importance
• Dorsolateral + Basomedial area = Prefrontal region
• Damage to prefrontal region can impair Intelluctual functions
(Sequencing, Processing, attention, concentration and execution) as
well as cause Personality changes (Pseudosychopathic or
Pseudodepressive)
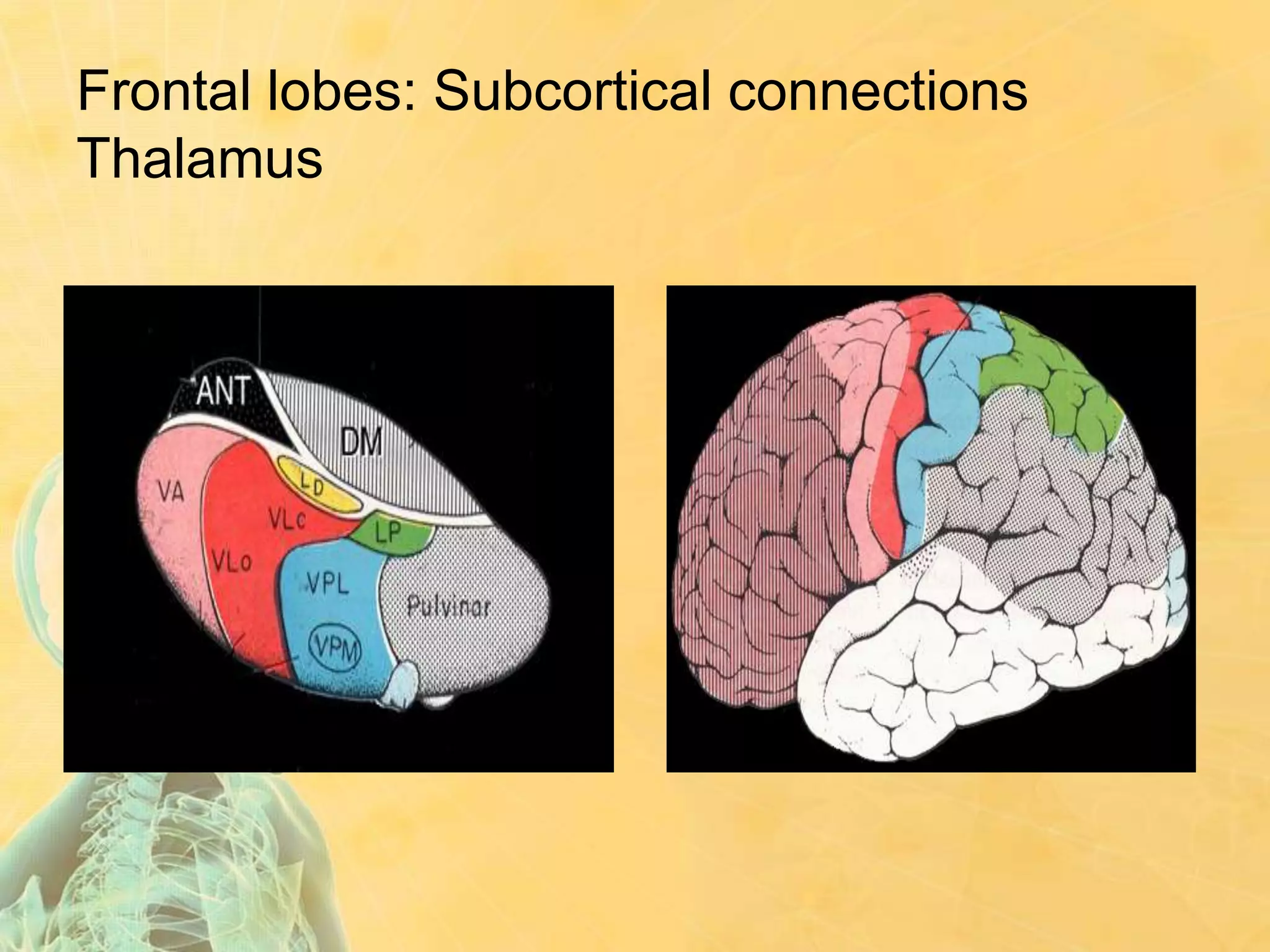
• Connections with thalamus
1. Magnocellular region (medial part of dorsomedial nucleus of
thalamus ) to Basomedial/OF region (damage can cause
Pseudopsychopathic syndrome)
2. Parvicellular region (lateral part of dorsomedial nucleus of
thalamus) to Dorsolateral region of PFC (damage can cause
Pseudodepressive syndrome)
VI. SMA/Cingulate area
•SMA – medial aspect of BA 6
and and Ant. Cingulate gyrus is
BA 24, 32
• These areas are involved in
drive and motivated behavior
(Mega and Cummings, 1994),
initiation and goal-directed
behavior (Devinsky et al, 1995)
• Connections with older cortical
and deep limbic structures
• Environmental exploration
• Complex attention
66.
Cingulate/SMA dysfunction
• Akineticmutism occurs with gross lesions (e.g., meningioma) of the
anterior cingulate. Such patients are profoundly apathetic, generally
mute and eat and drink only when assisted. They do not respond to
pain and are indifferent to their circumstances.
• Lesions of the supplementary motor area are associated with the
alien hand syndrome (Goldberg & Bloom, 1990).
• The apathy of schizophrenia and the immobility of depressive
disorder may be associated with defects in associated circuits.
• At present there are no office or neuropsychological tests to
measure the functional status of these areas.
FRONTAL LOBE SYNDROME
•Dysexecutive syndrome consists of a number of symptoms which tend
to occur together (hence it being described as a syndrome). Broadly
speaking, these symptoms fall into three main categories; cognitive,
emotional and behavioural.
• Cognitive - Short attention span, Poor working memory, Poor short
term memory, Difficulty in planning and reasoning, Environmental
dependence syndrome
• Emotional - Difficulty in inhibiting emotions, anger, excitement,
sadness etc., Depression, Occasionally, difficulty in understanding
others' points of view, leading to anger and frustration.
• Behavioural - Utilization behaviour, Perseveration behaviour
Inappropriate aggression, Inappropriate sexual behaviour,
Inappropriate humour and telling of pointless and boring stories
(Witzelsucht)