Downloaded 2,215 times
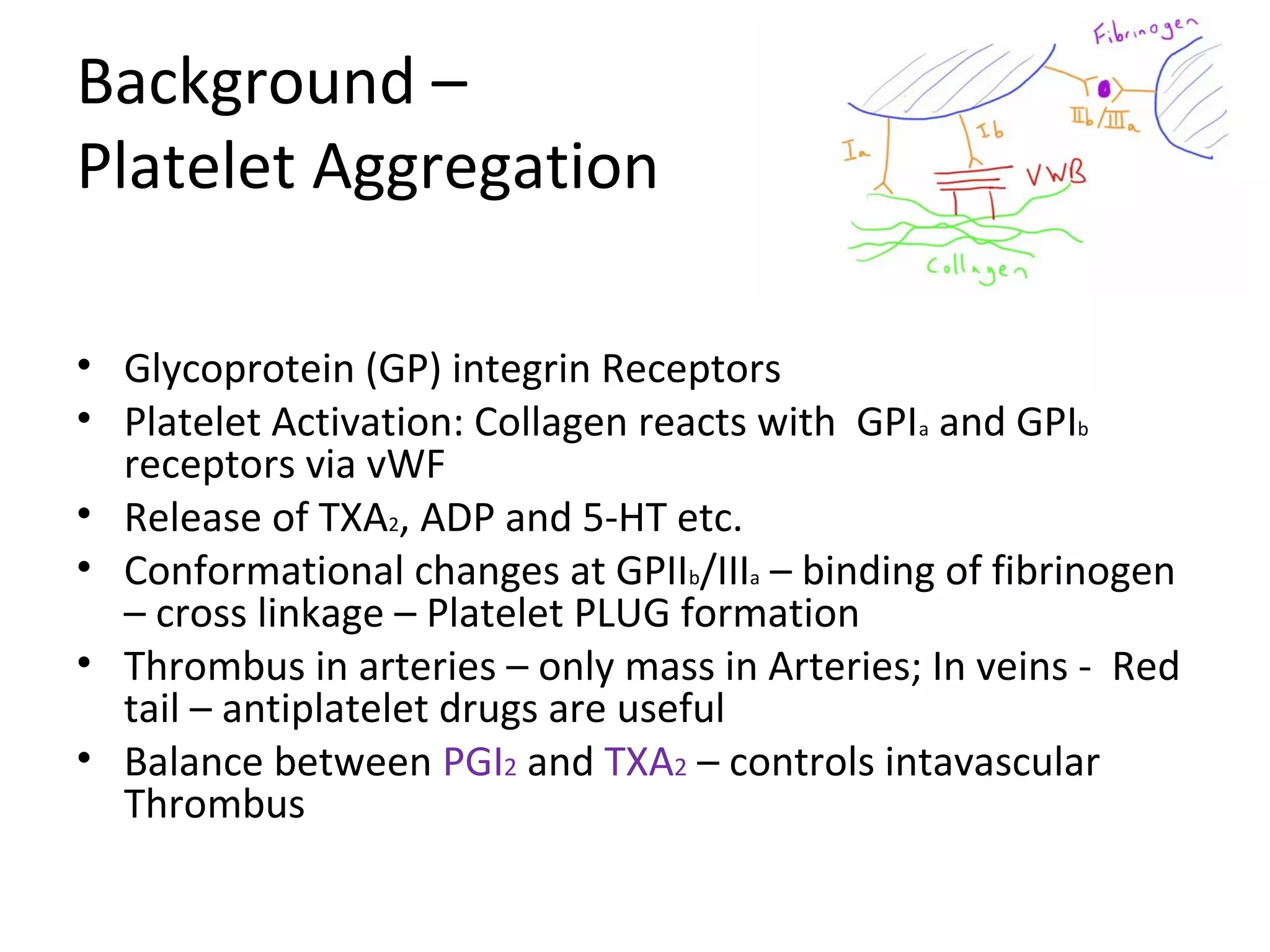
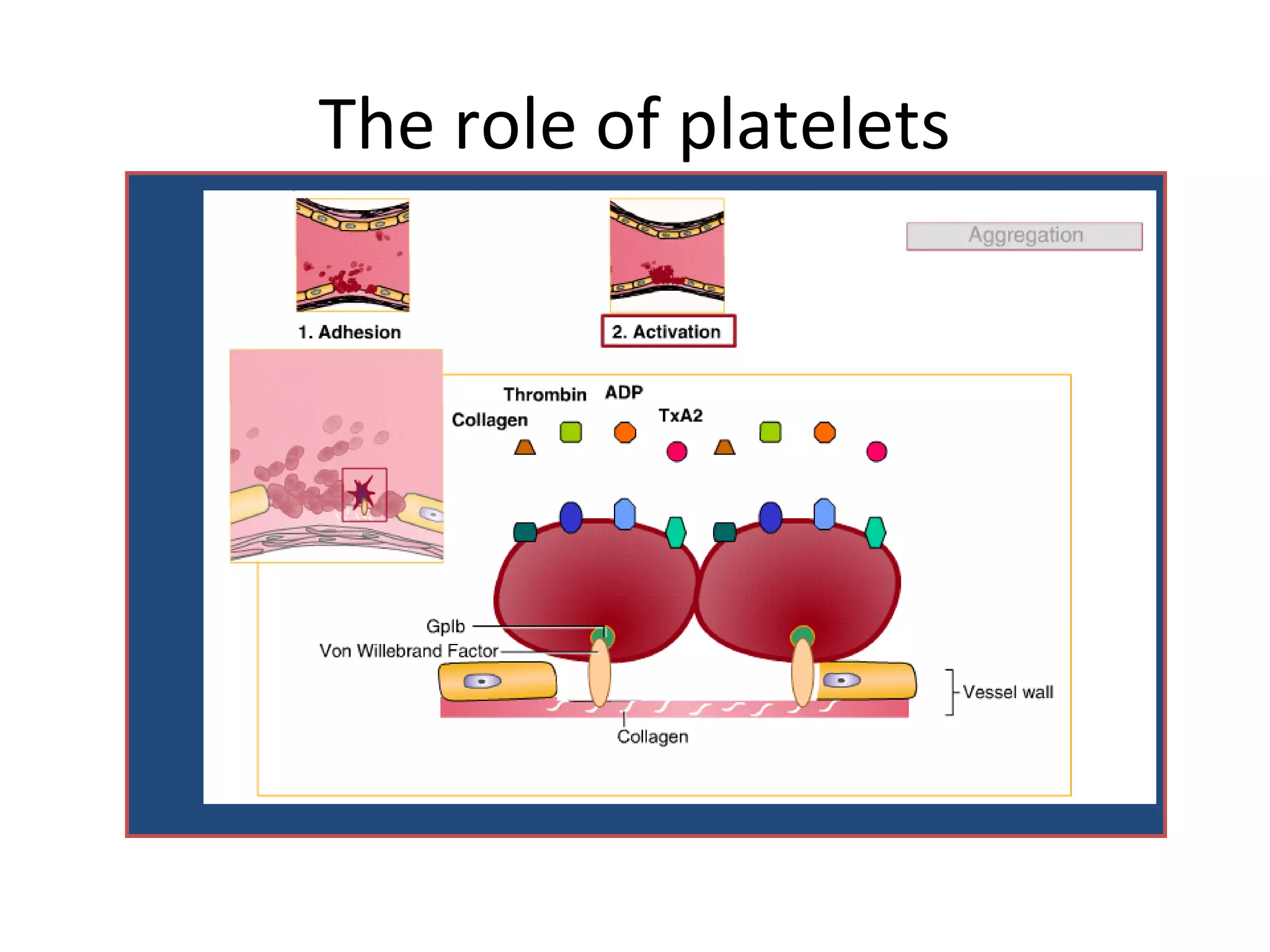
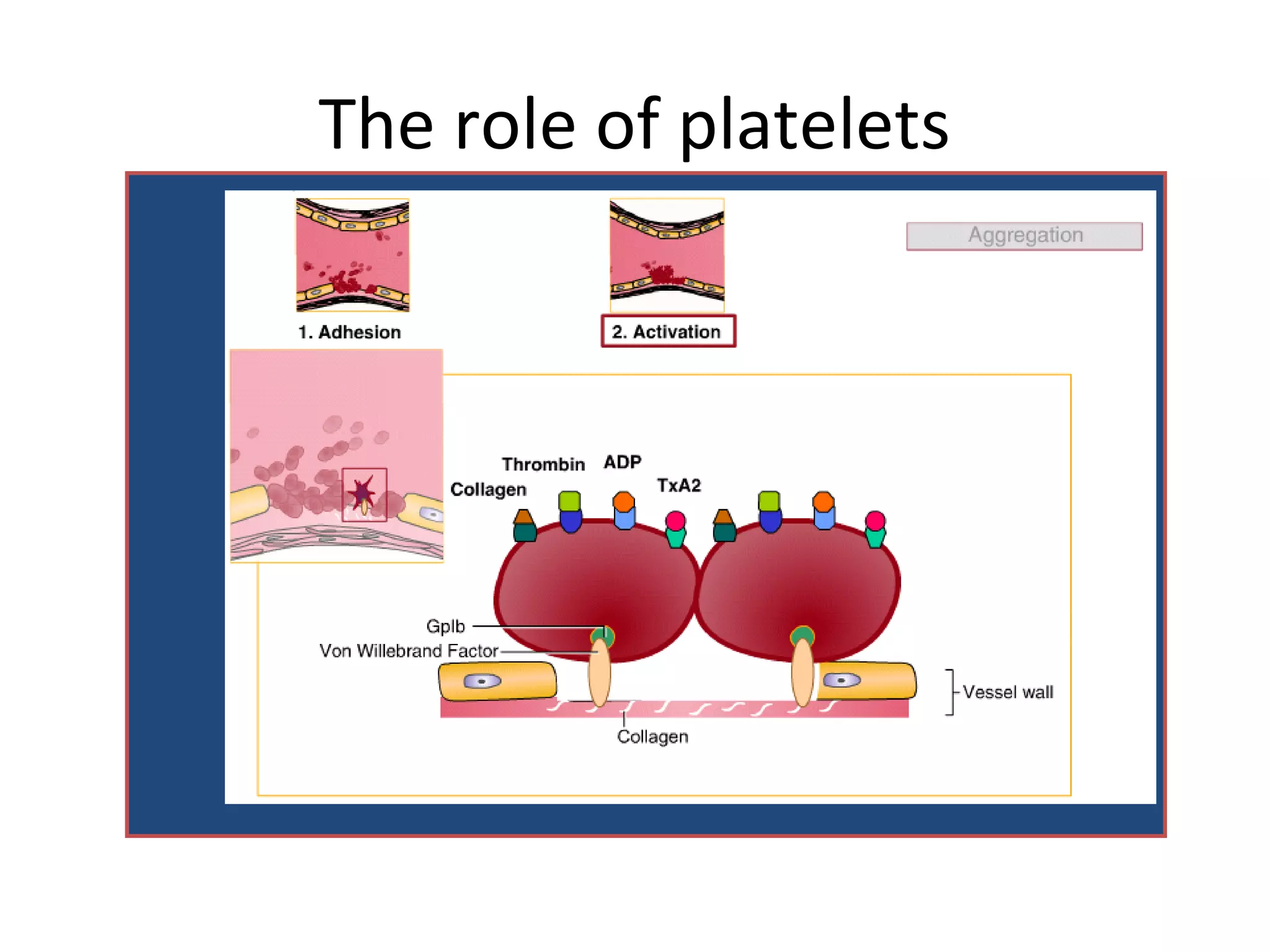
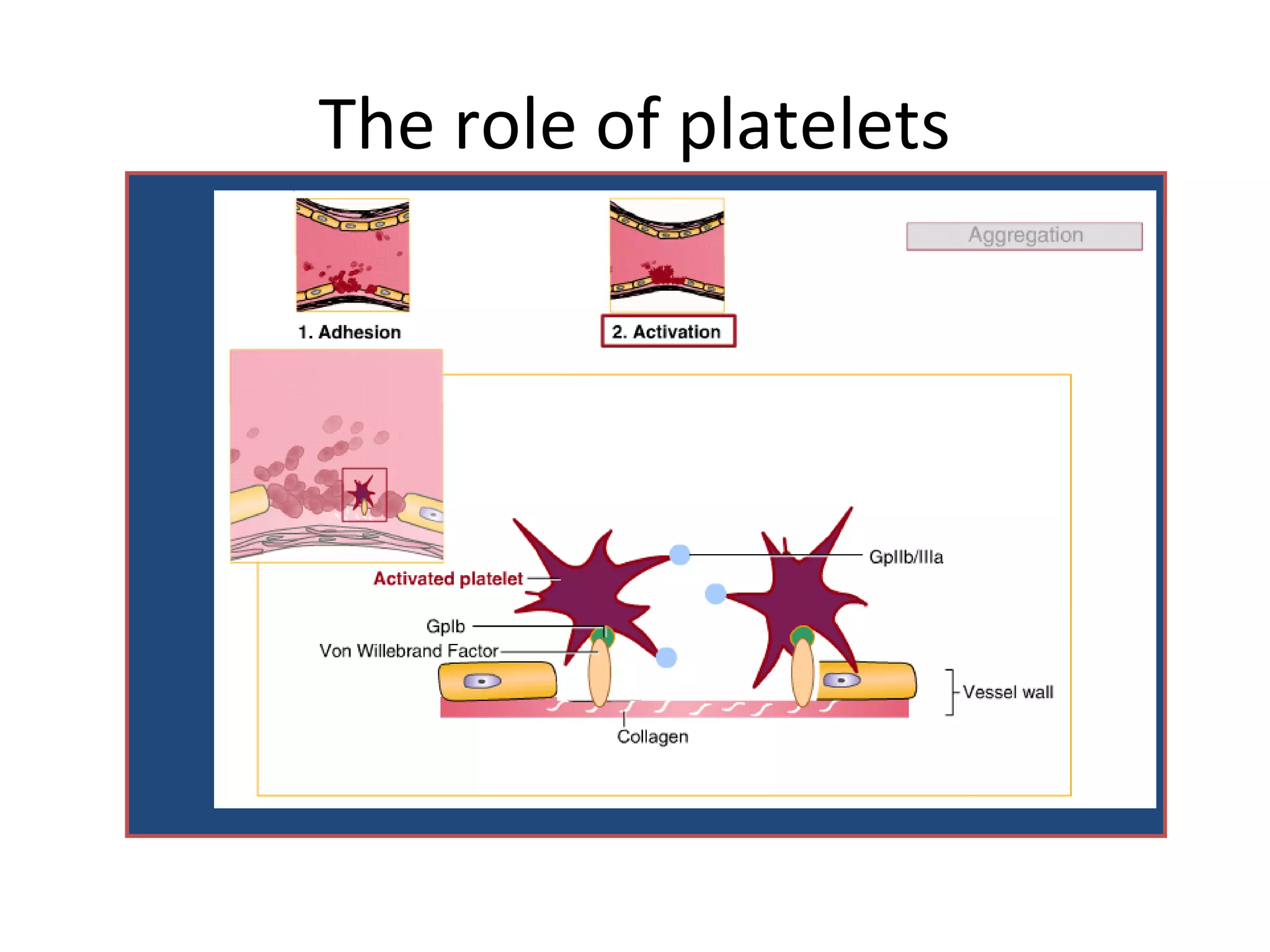

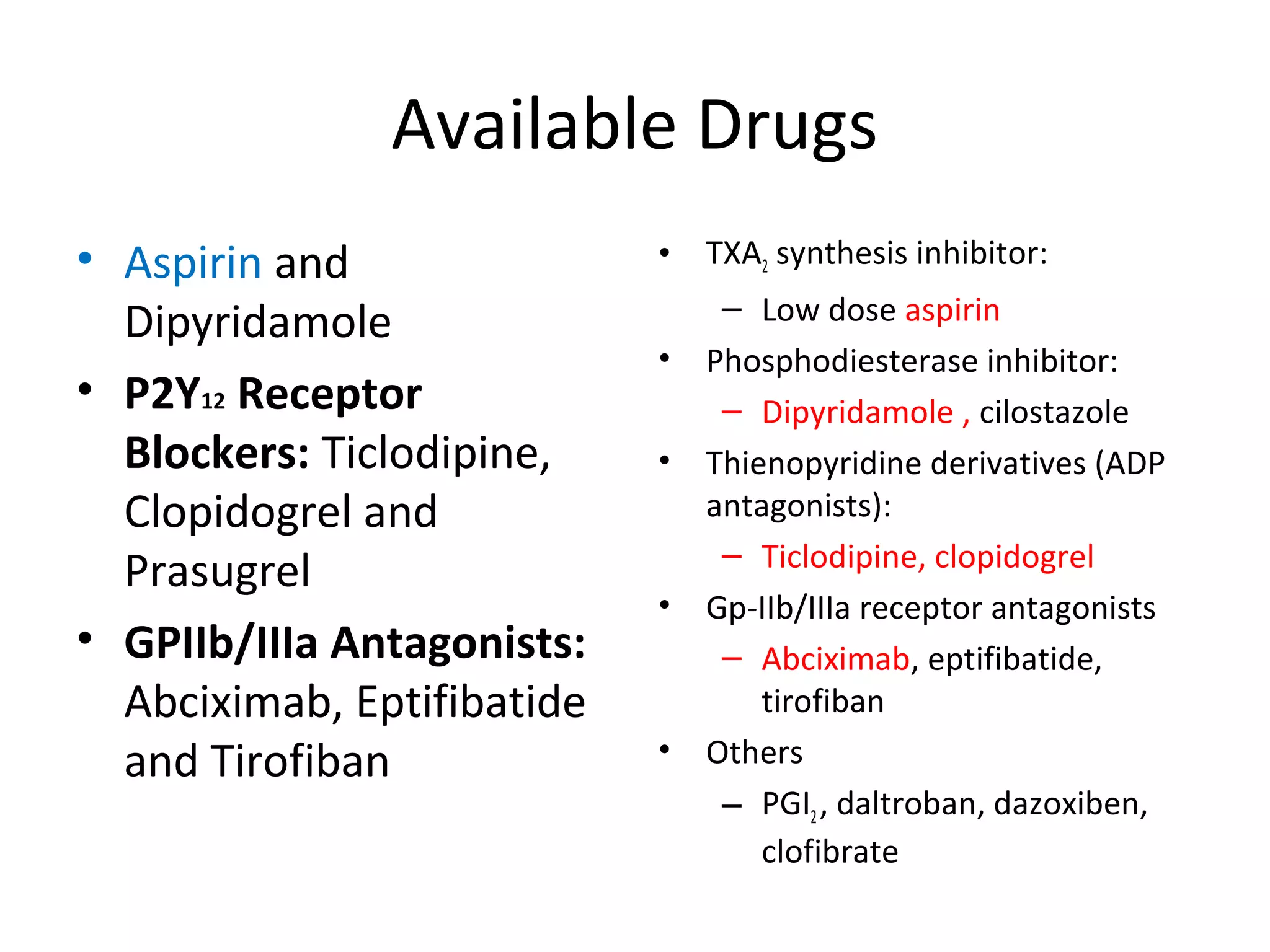


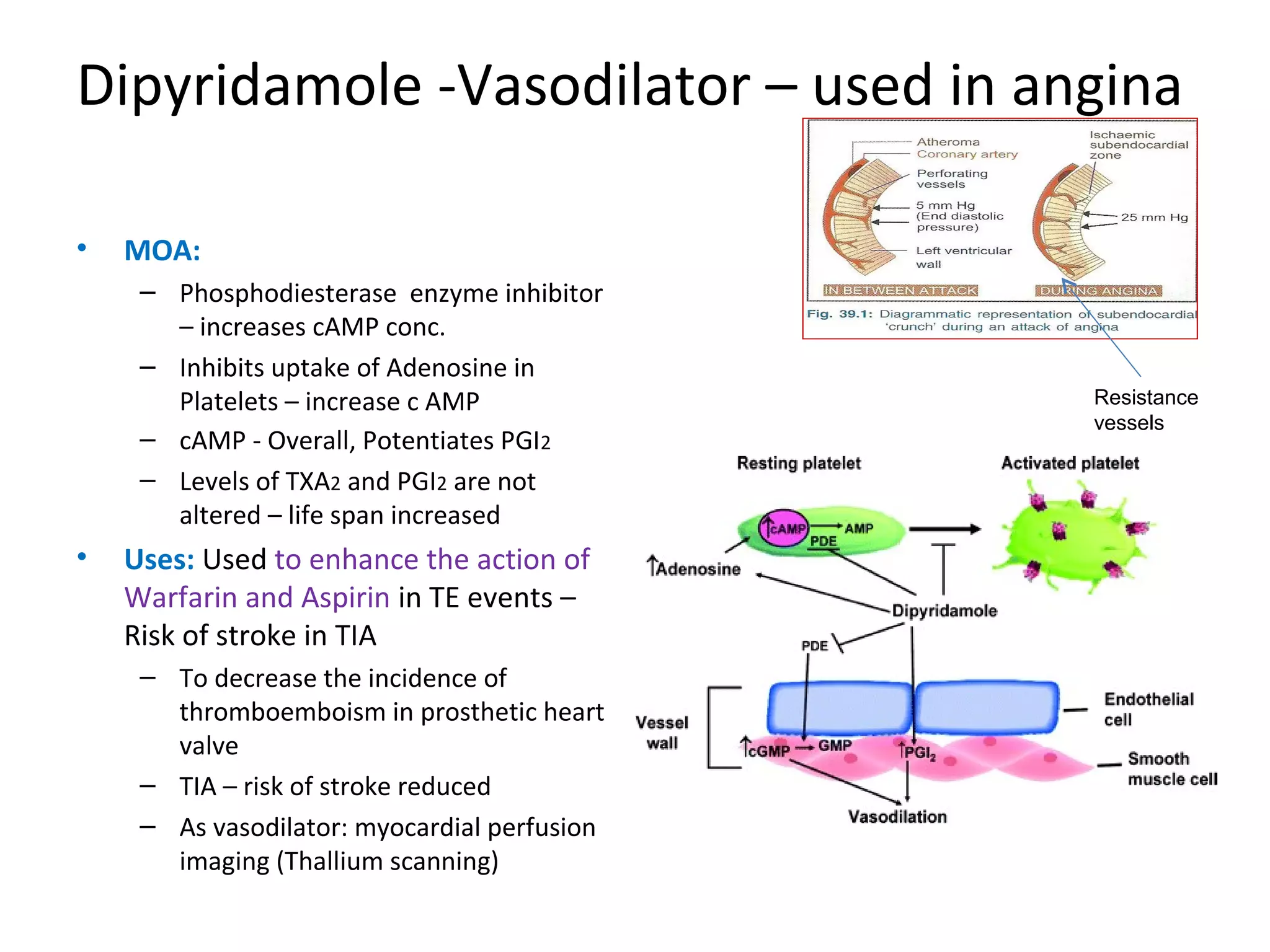
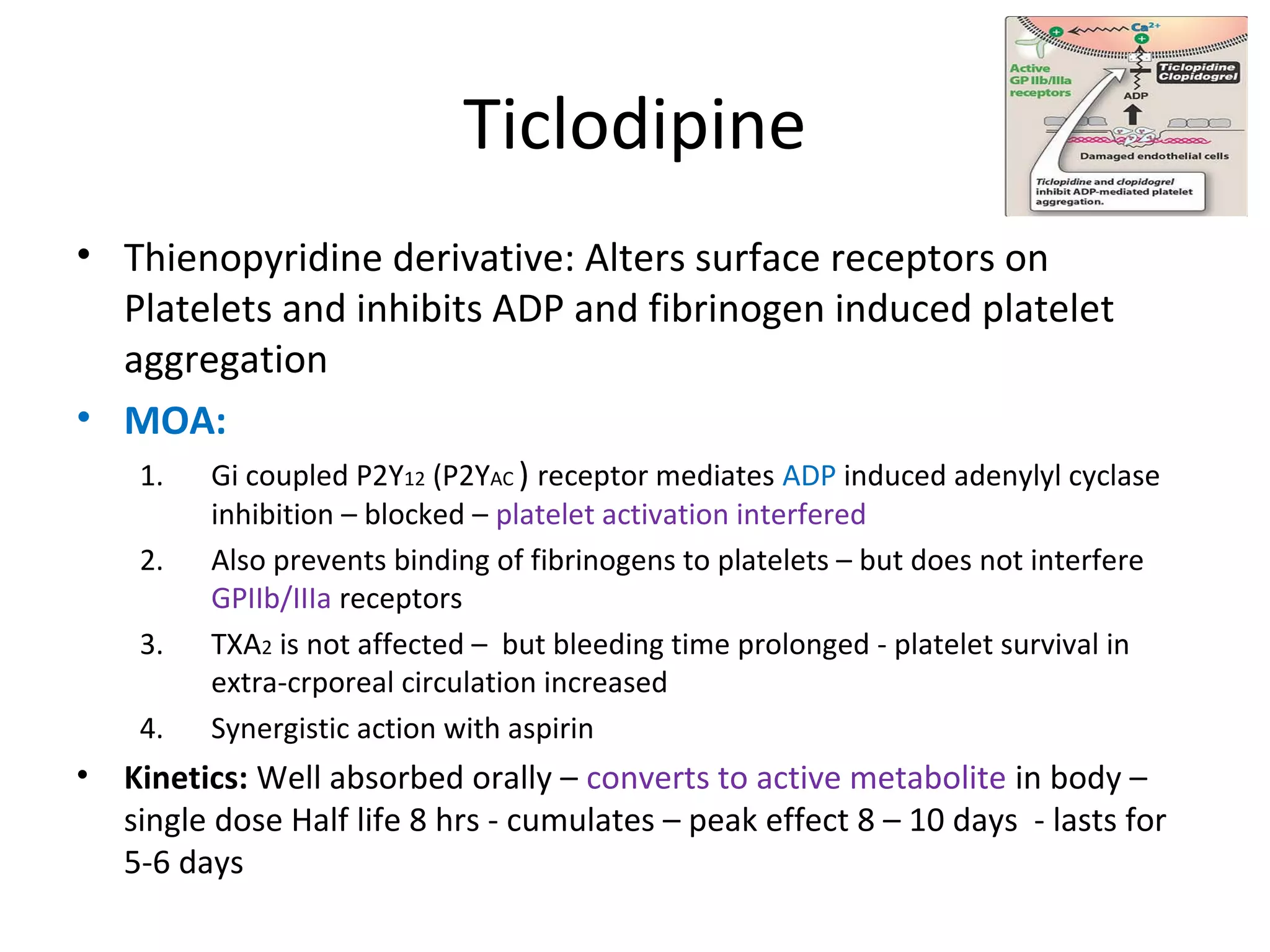



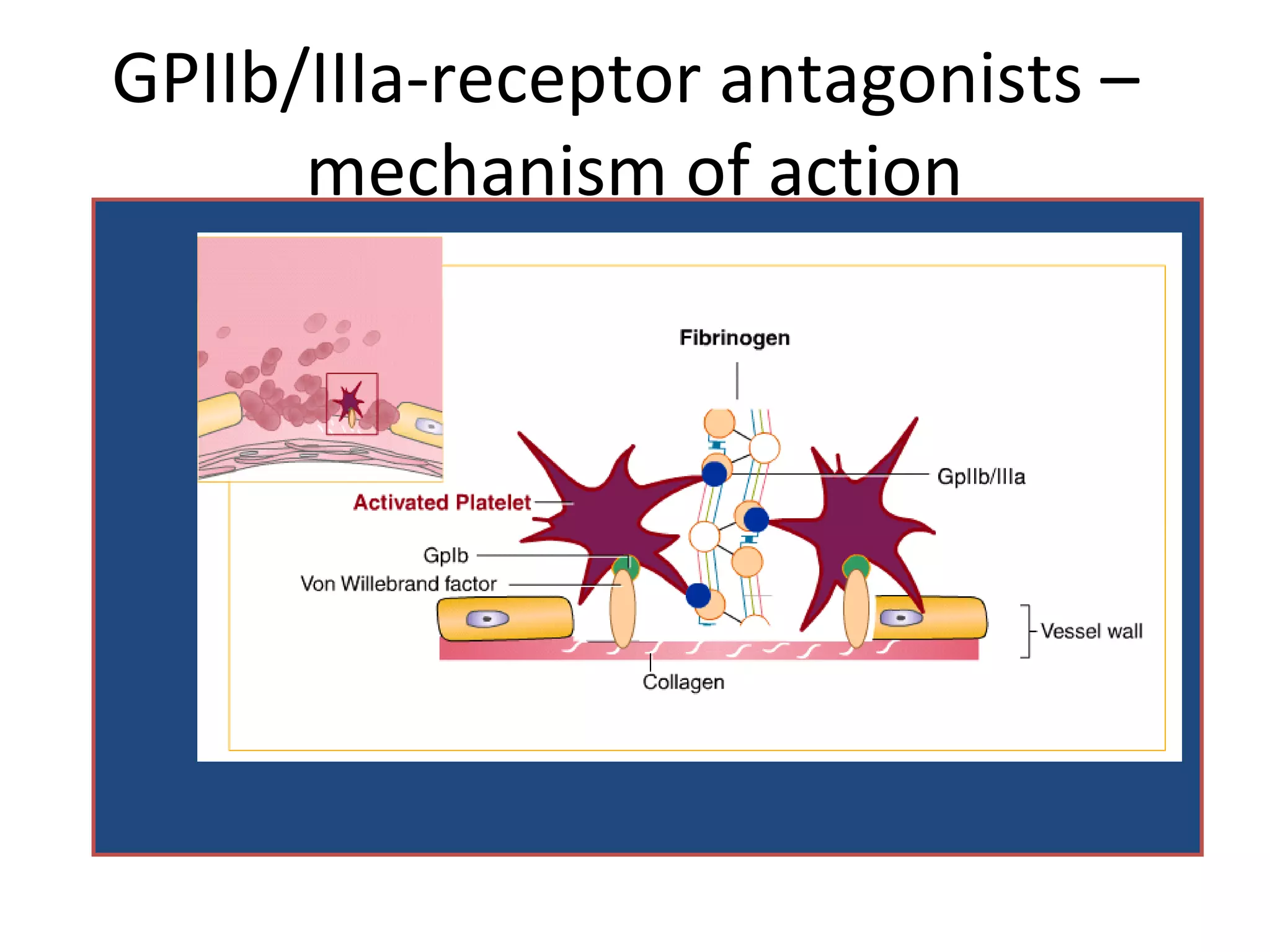


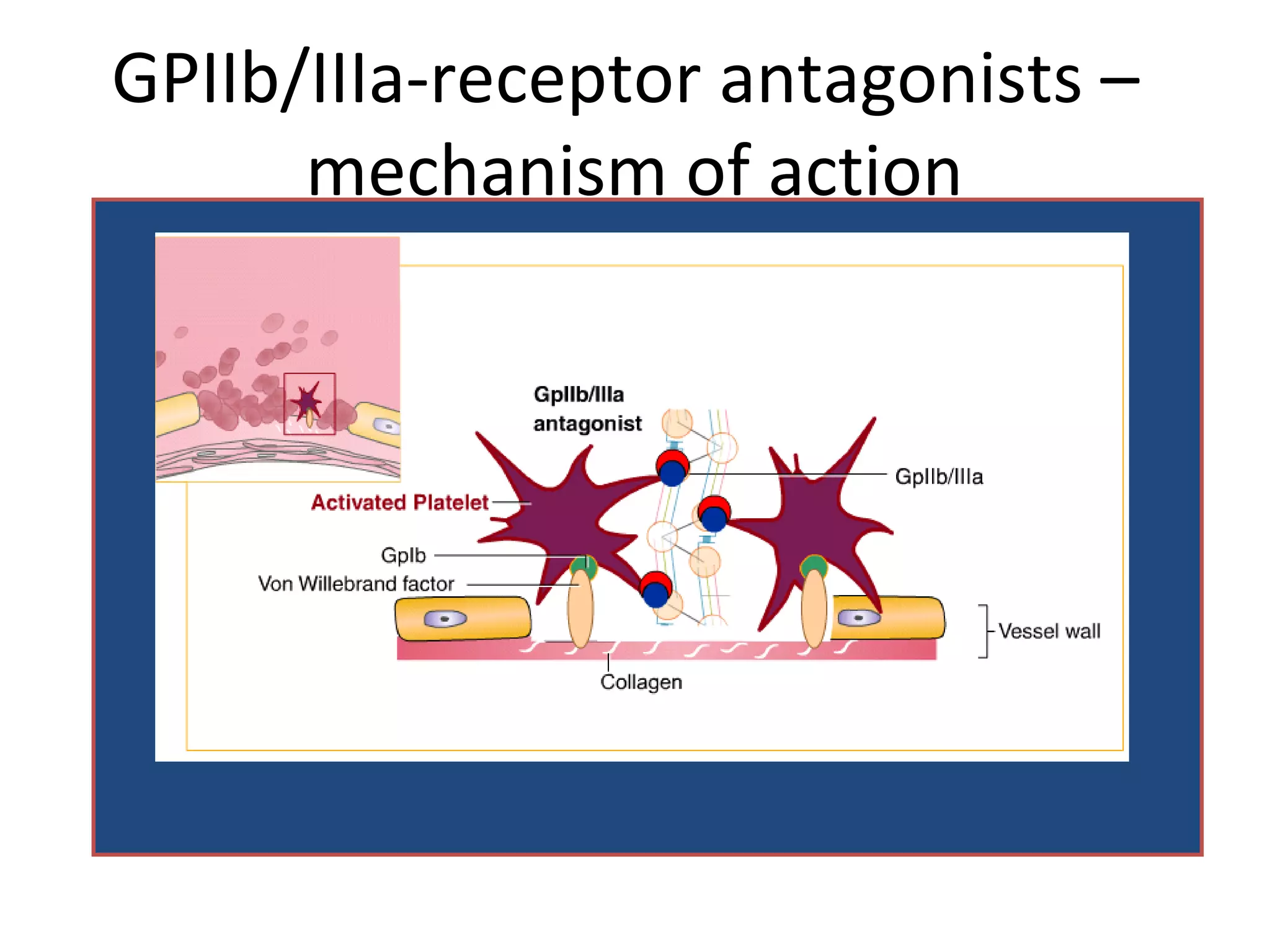


Dr. D. K. Brahma discusses antiplatelet drugs, which interfere with platelet function and are useful for preventing thromboembolic disorders. The document defines antiplatelet drugs and describes the role of platelets in thrombosis formation. It then discusses the mechanisms of various antiplatelet drugs including aspirin, dipyridamole, ticlodipine, clopidogrel, prasugrel, and GPIIb/IIIa receptor antagonists like abciximab. The uses of these antiplatelet drugs for conditions like heart attacks, strokes, angioplasty and stents are summarized.























































































