Downloaded 1,070 times
![Classification
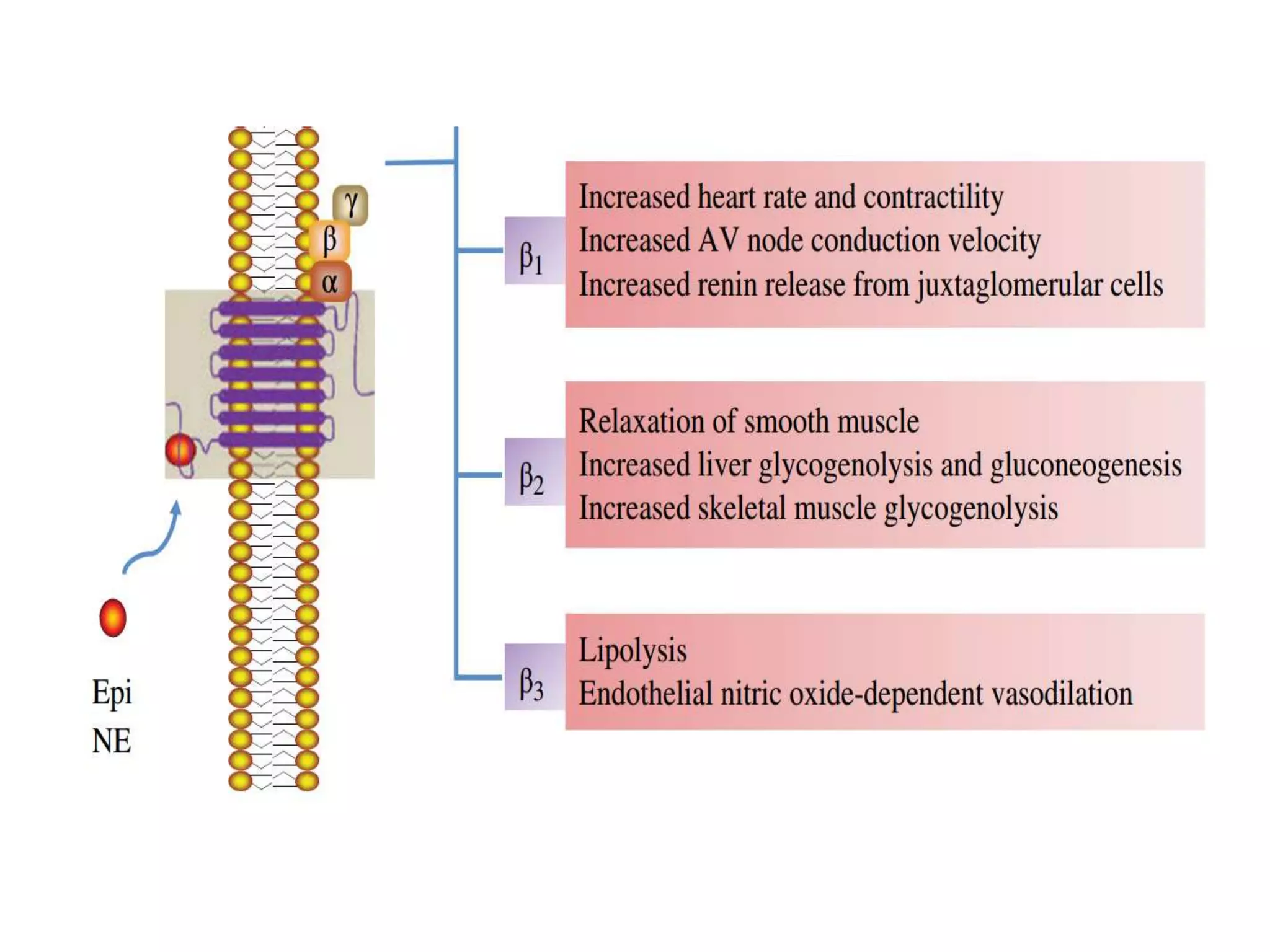
I. Nonselective (β1 and β2)
a. Without ISA* Propranolol, Sotalol, Timolol.
b. With ISA* Pindolol
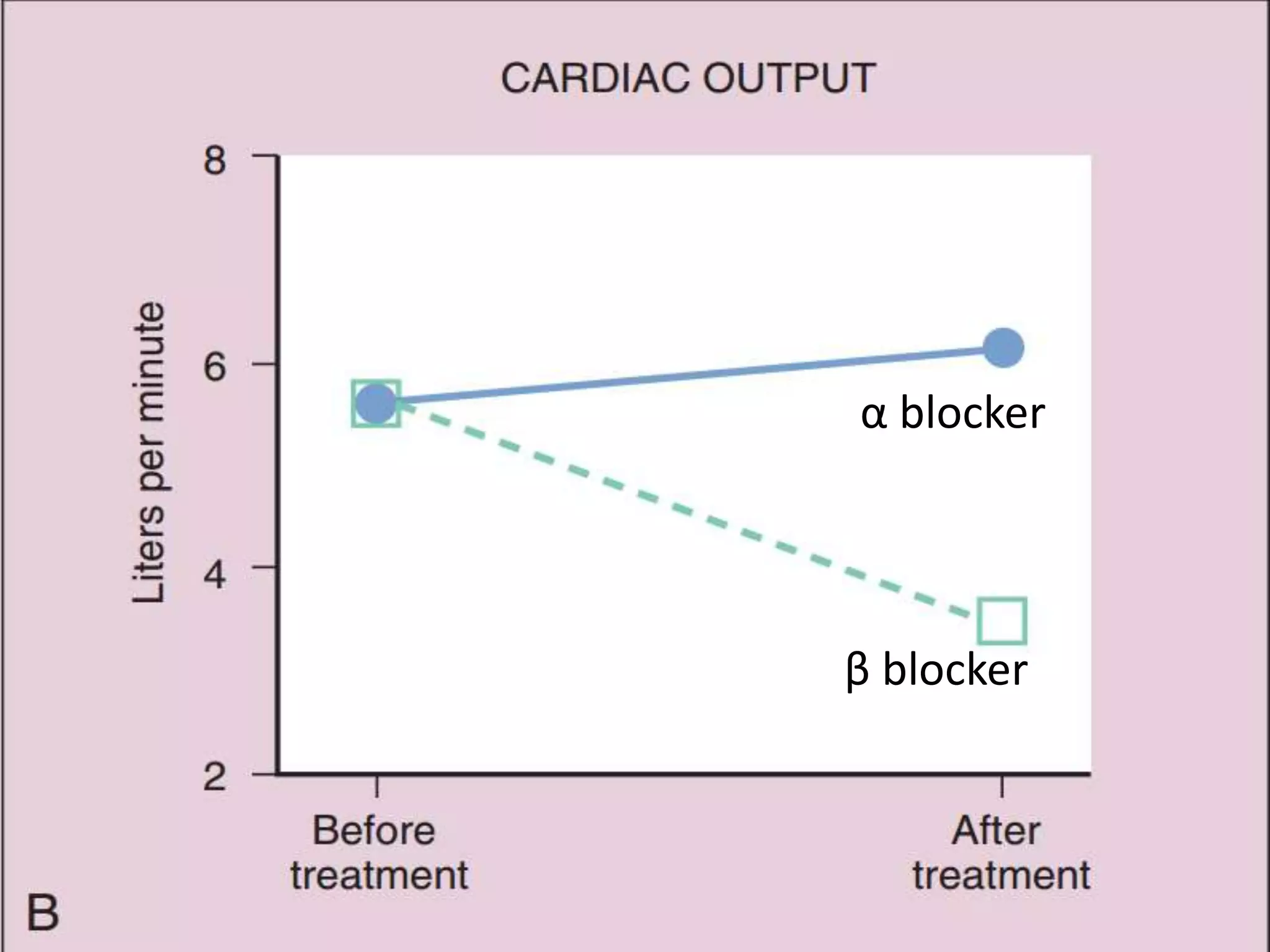
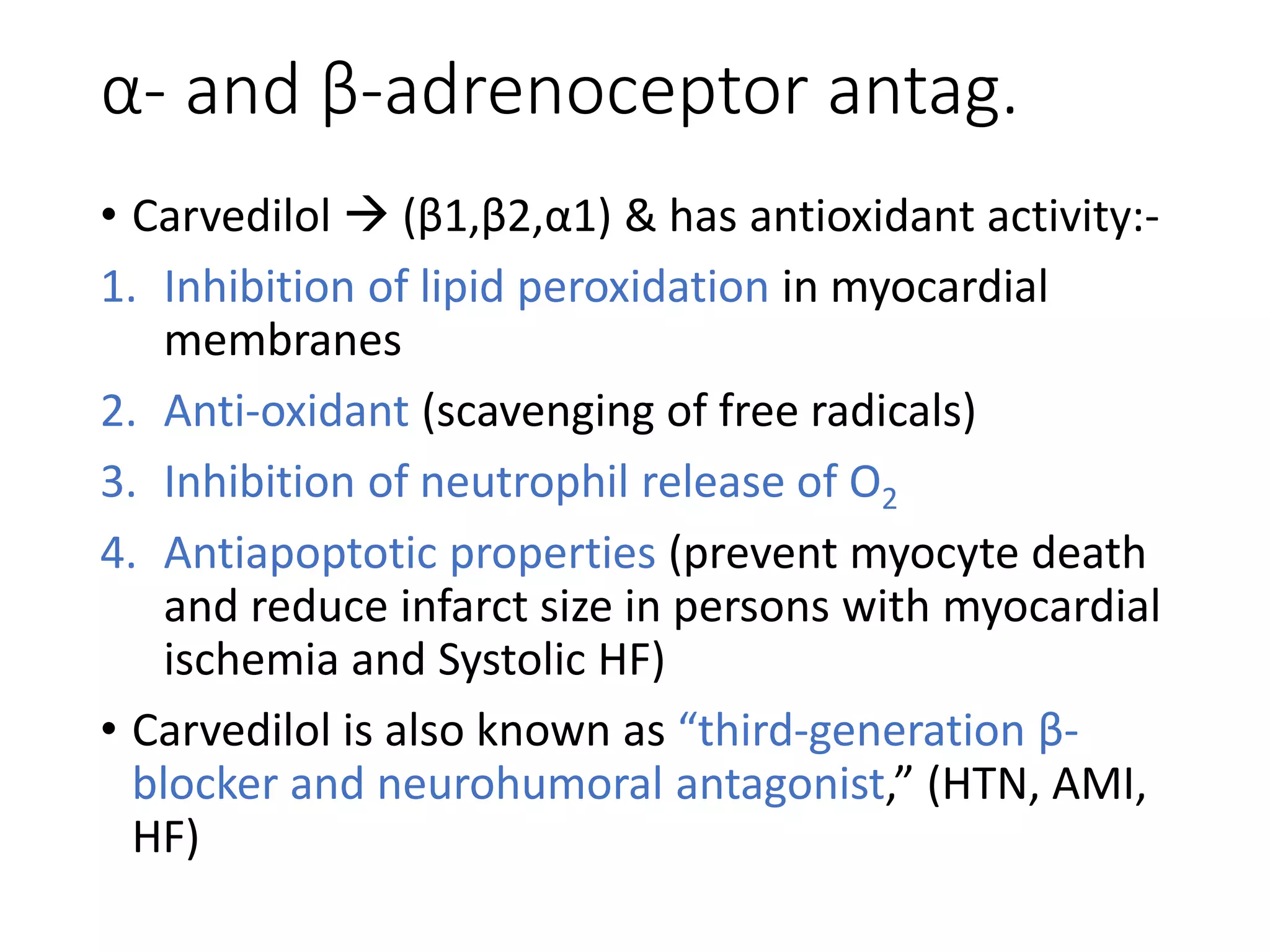
c. Addnl. α blocking property Labetalol, Carvedilol
II. Cardioselective (β1) [safe in asthmatics]
Metoprolol, Atenolol, Acebutolol, Bisoprolol,
Esmolol, Betaxolol, Celiprolol, Nebivolol
*ISA - intrinsic sympathomimetic activity](https://image.slidesharecdn.com/betaadrenergicblockers-150412052808-conversion-gate01/75/Beta-adrenergic-blockers-7-2048.jpg)
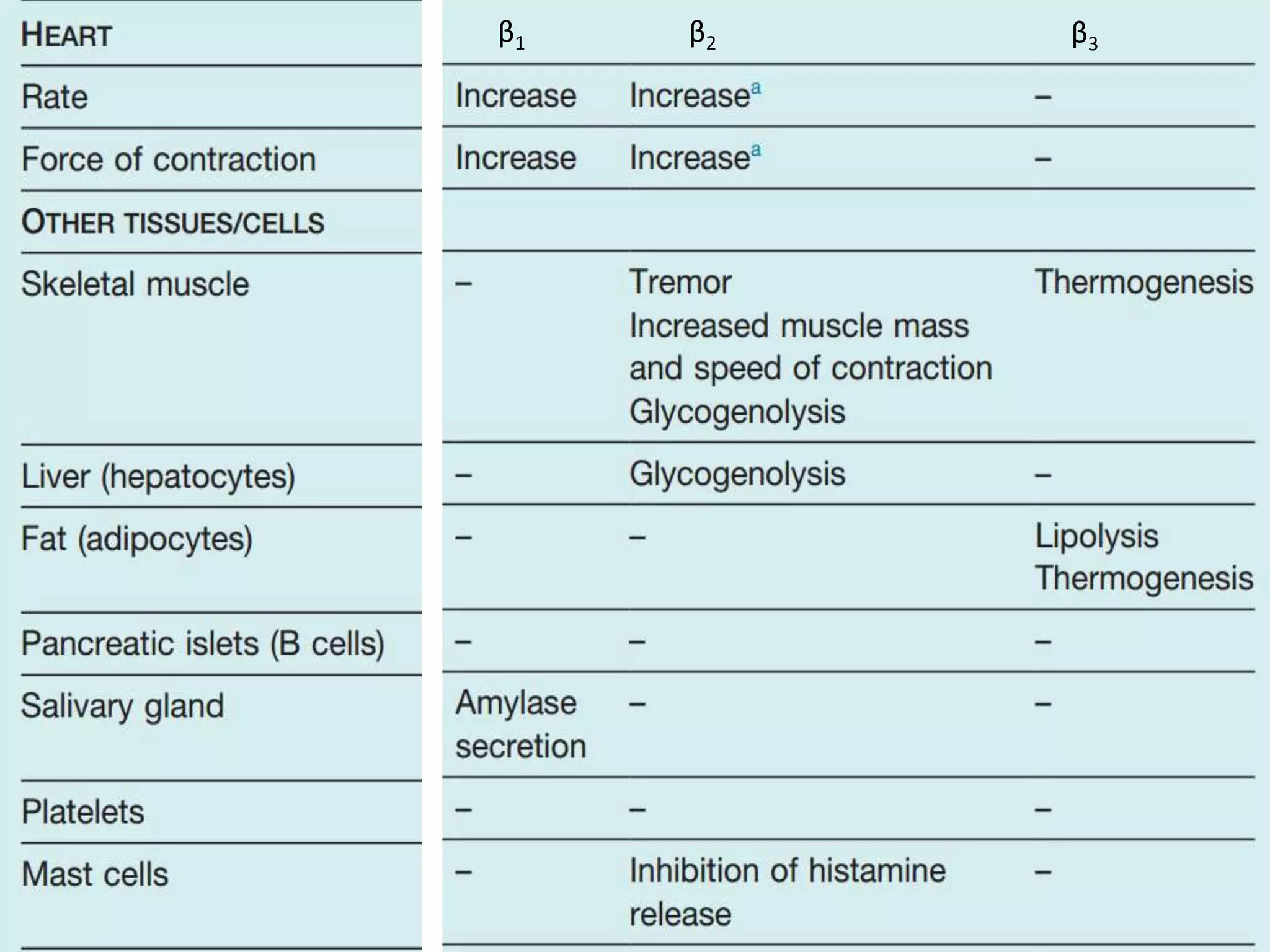
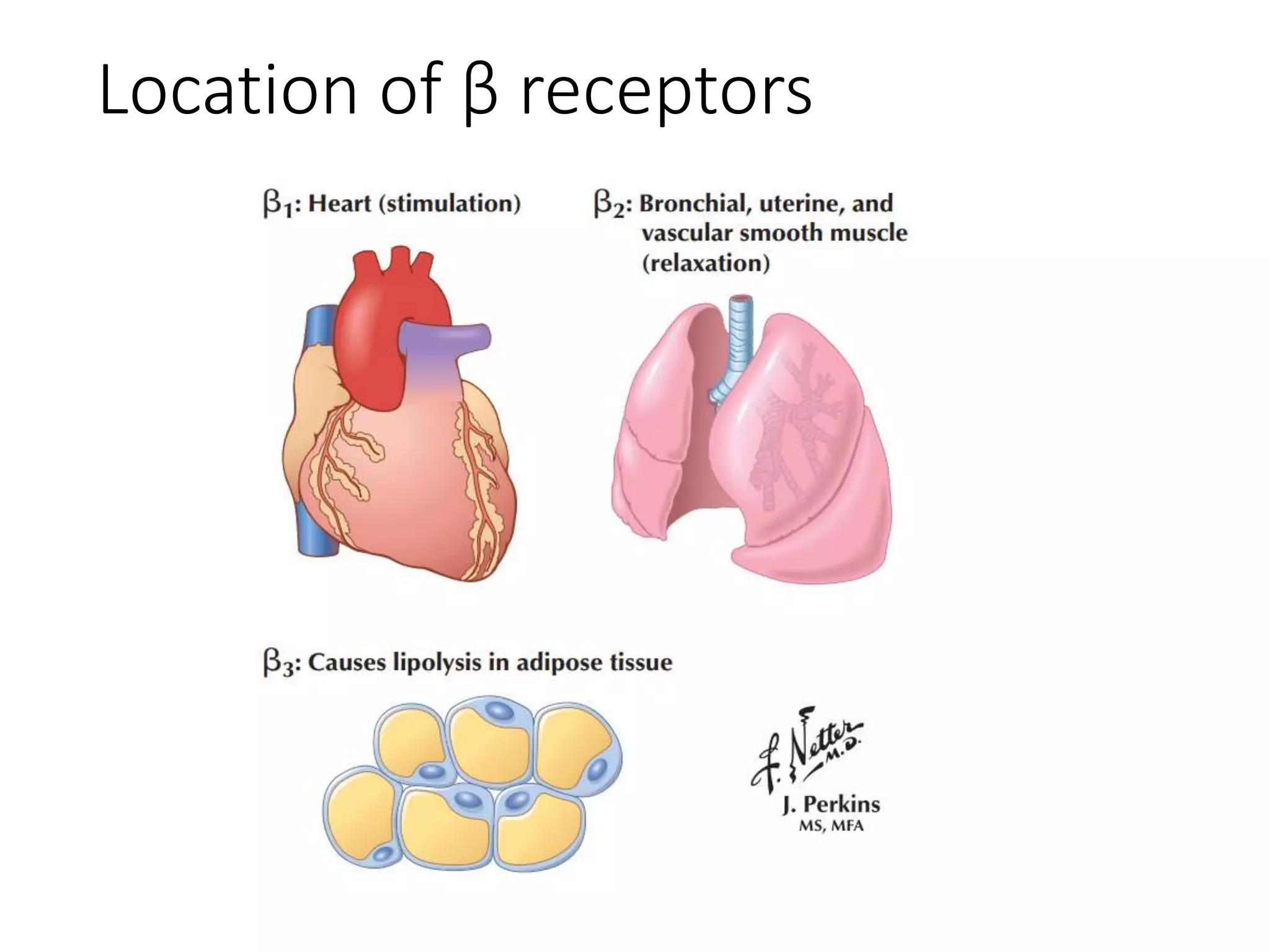
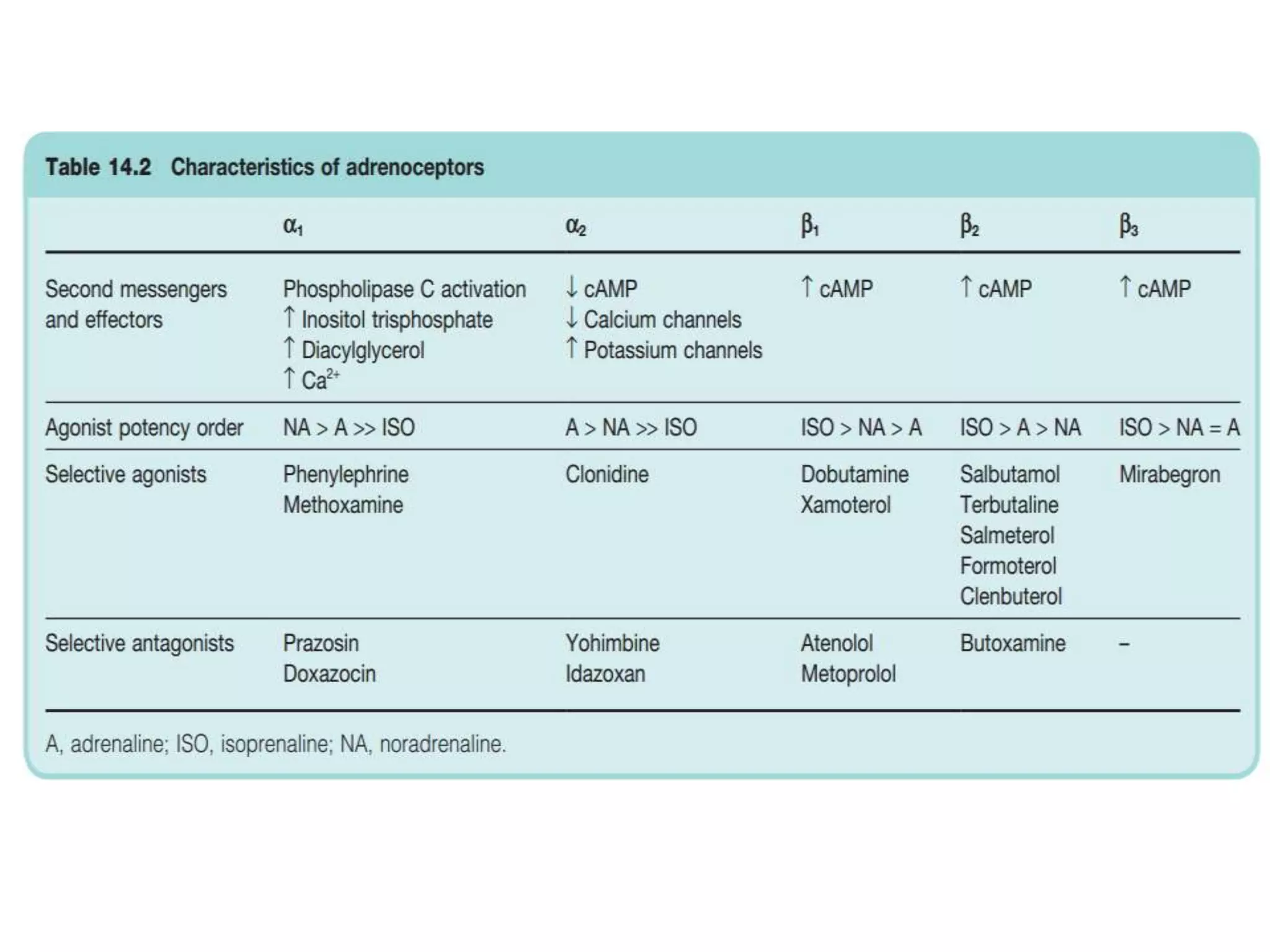
![Effect on respiratory tract
• Blockade of β2 rec. in bronchial smooth muscle
↑ airway resistance (asthma)
• Patients with chronic obstructive pulmonary
disease (COPD) tolerate these drugs quite well &
benefits outweigh the risks (Albouaini et al., 2007)
• Patients with COPD discharged with β-blockers
after an MI had a lower all-cause mortality
compared to patients not prescribed β-blockers
(Andell et al., 2015) [JAHA, 2015]](https://image.slidesharecdn.com/betaadrenergicblockers-150412052808-conversion-gate01/75/Beta-adrenergic-blockers-18-2048.jpg)





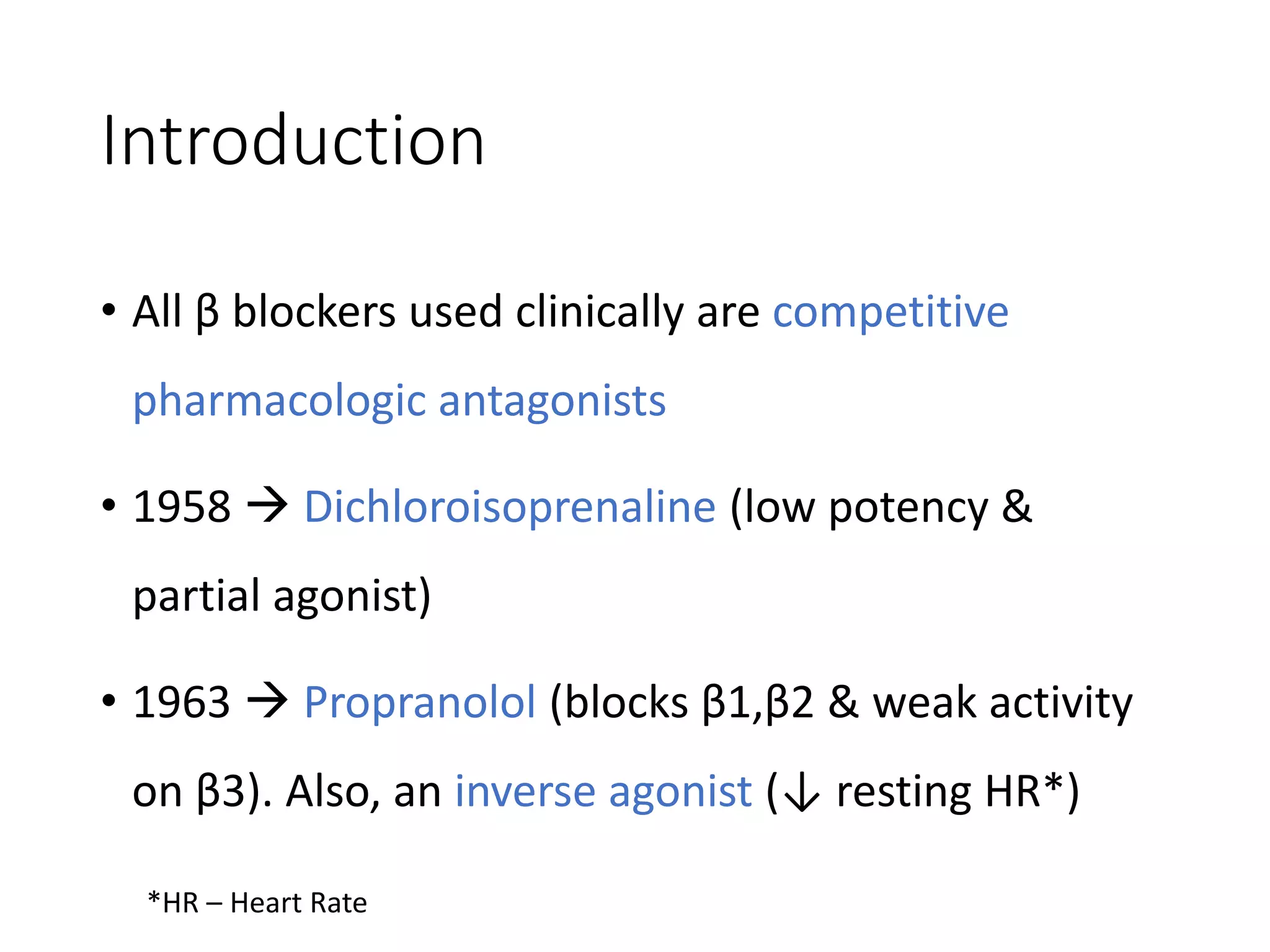
![• Abrupt withdrawal of BB should not be done (ppt.
angina attack & acute MI due to sudden ↑
sympathetic tone of heart; upregul. Of beta rec.
(tapered over 2-3 days)]
• ↑ EDV & ↑ ejection time (↑ MOD) blunts
beneficial effects of BB if used as a single drug
therapy for angina](https://image.slidesharecdn.com/betaadrenergicblockers-150412052808-conversion-gate01/75/Beta-adrenergic-blockers-32-2048.jpg)



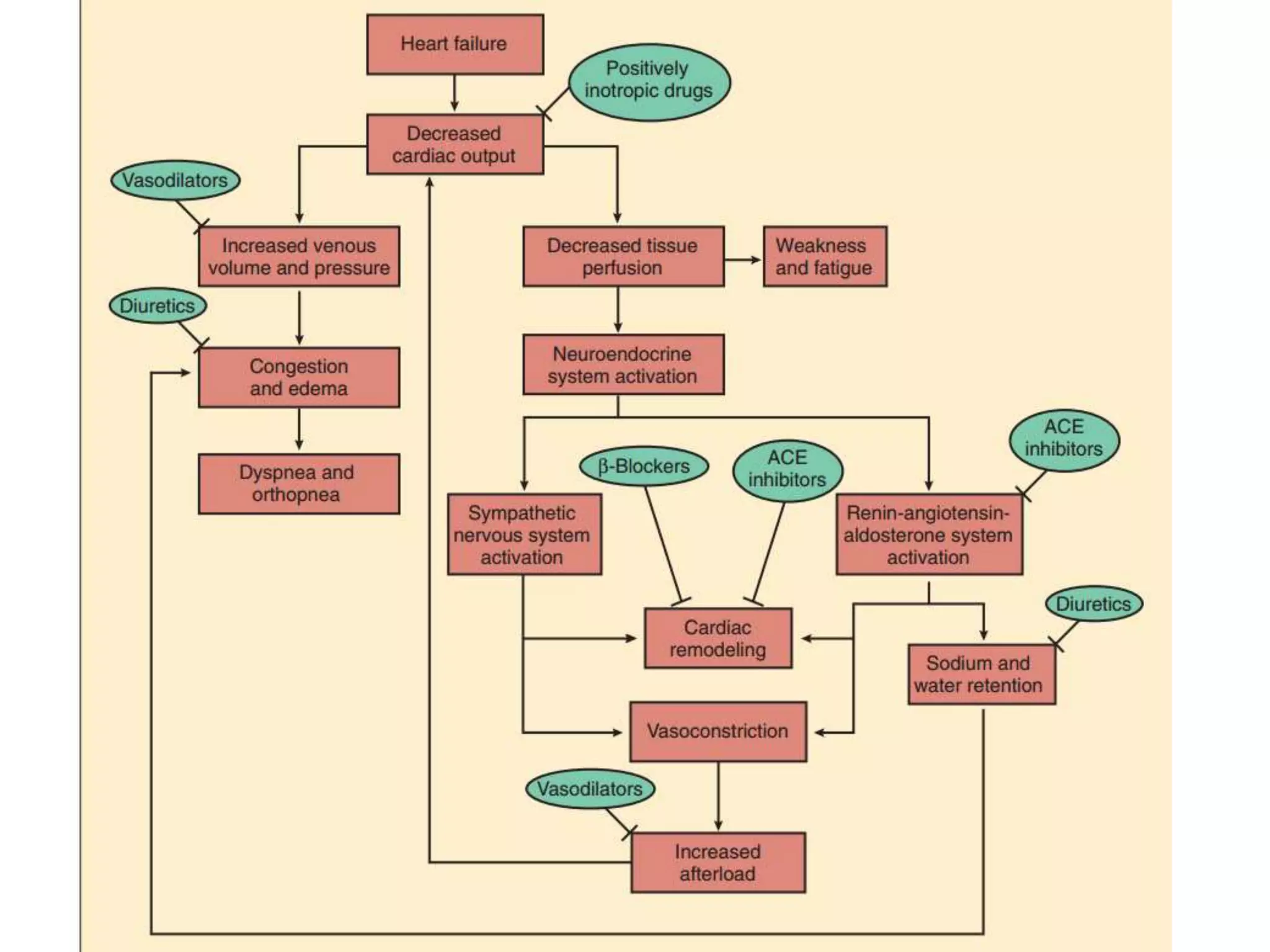
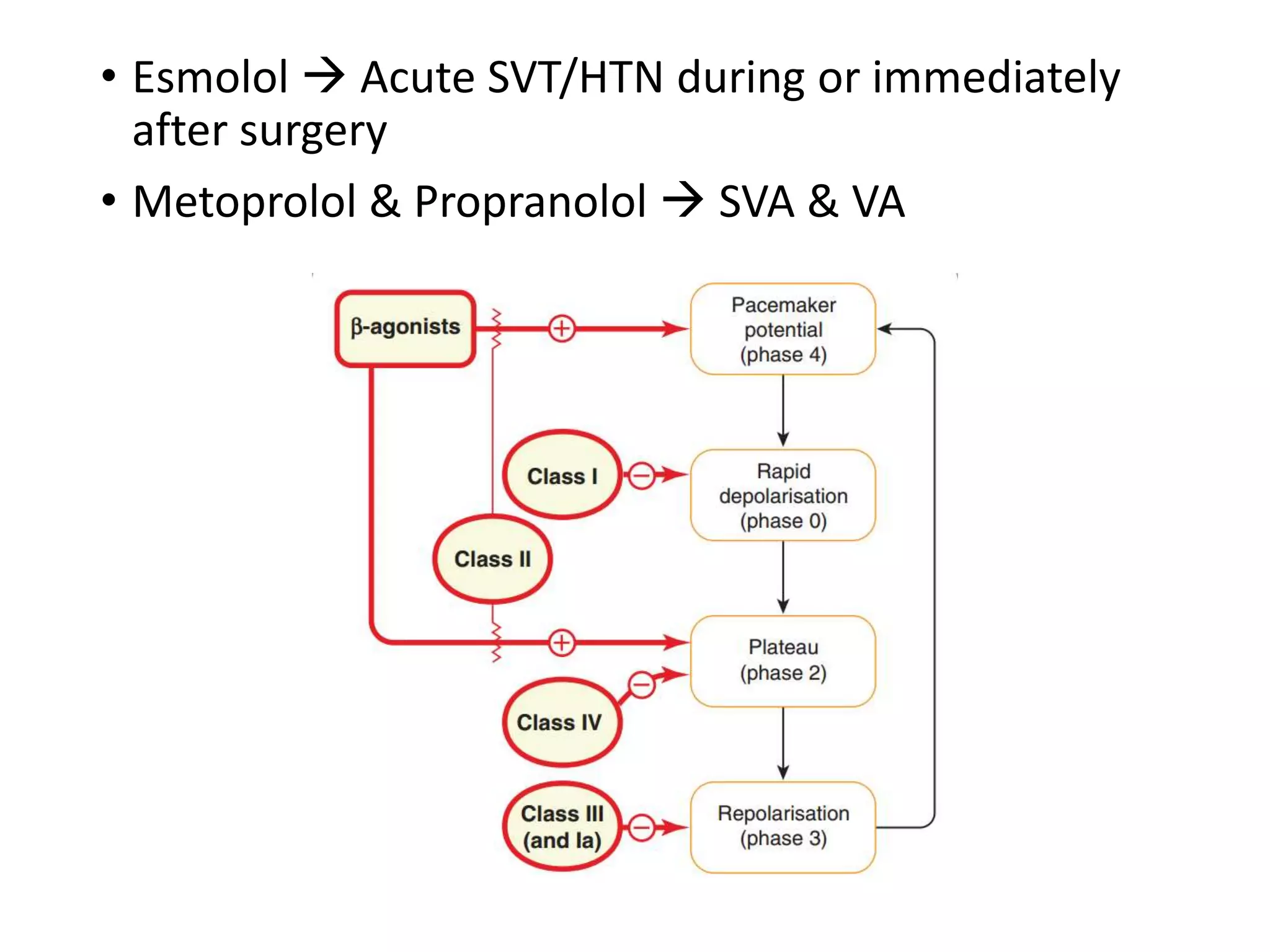


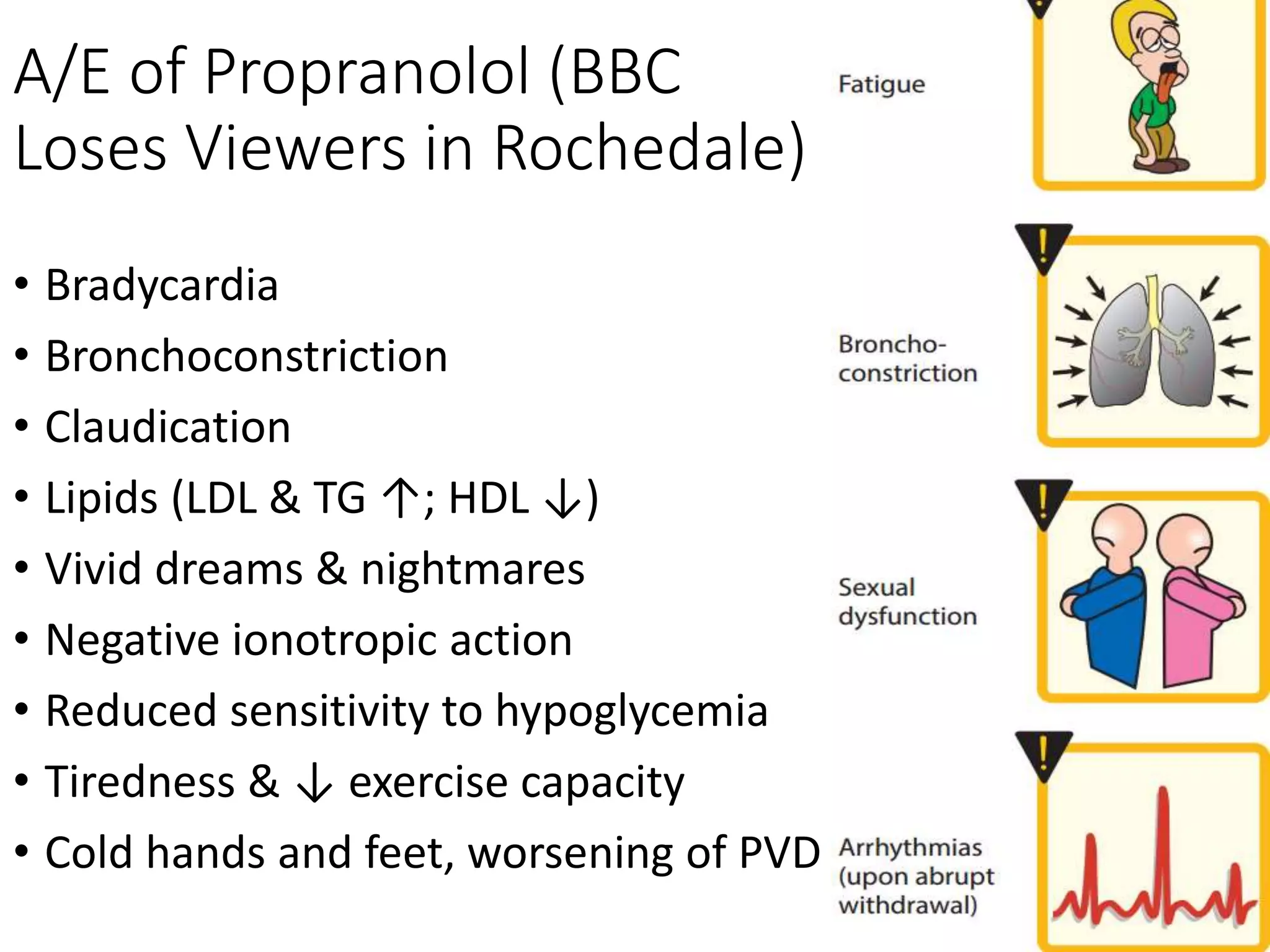


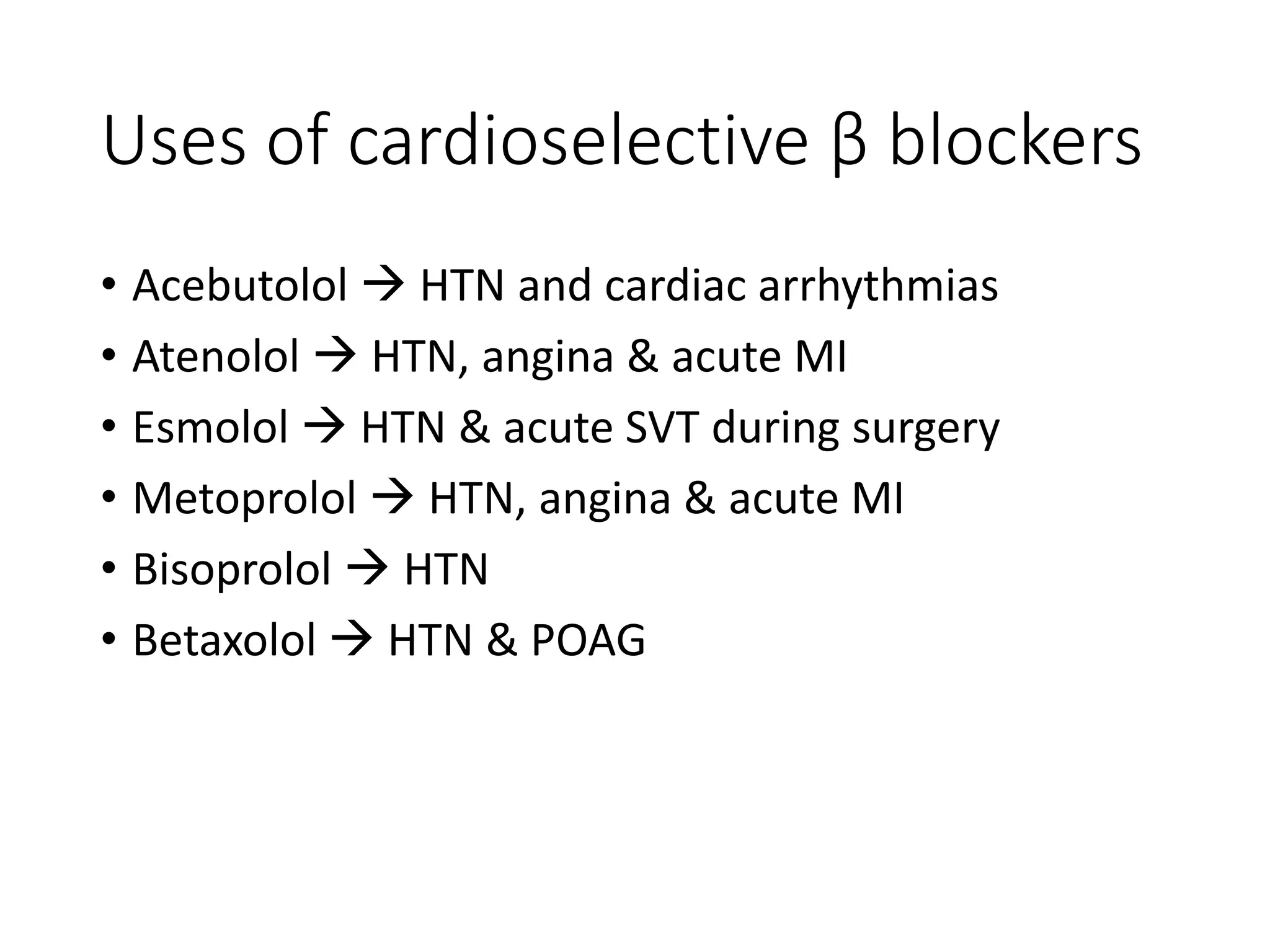



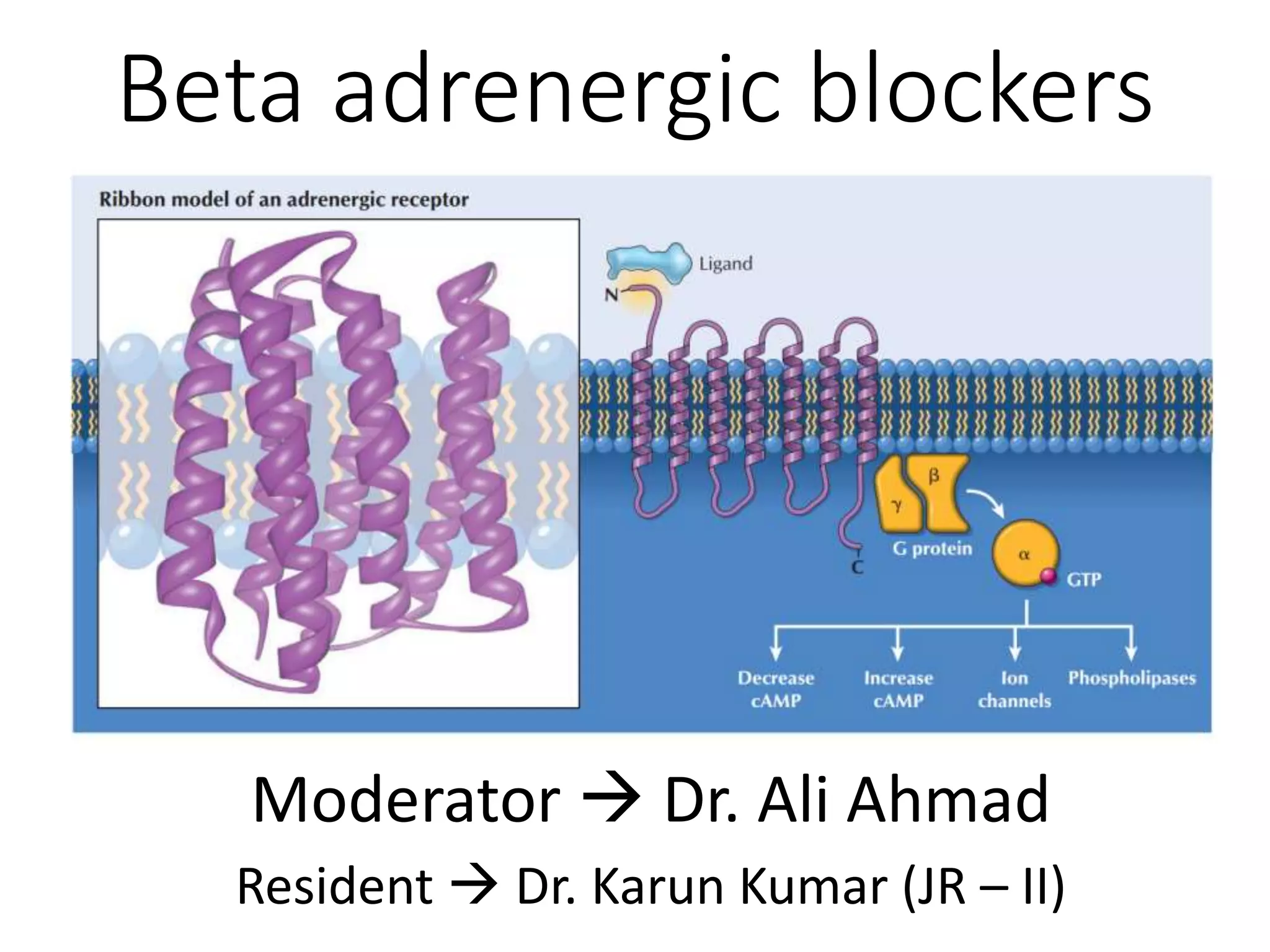
The document provides a comprehensive overview of beta adrenergic blockers, detailing their classification, pharmacokinetics, pharmacodynamics, and clinical applications. It discusses the effects of both nonselective and cardioselective beta blockers on various systems including the cardiovascular and respiratory systems, as well as their therapeutic uses in conditions such as hypertension, heart failure, and cardiac arrhythmias. The document also addresses the adverse effects, contraindications, and drug interactions associated with these medications.