Downloaded 1,085 times

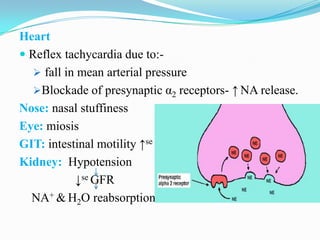
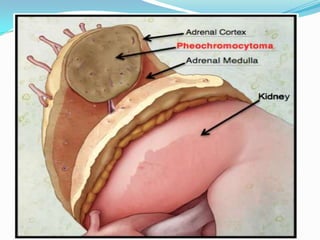


This document summarizes the classification, mechanisms of action, pharmacokinetics, and clinical uses of α-adrenergic receptor antagonists (α-blockers). It discusses non-selective α-blockers that block both α1 and α2 receptors like phentolamine and phenoxybenzamine, as well as selective α1-blockers like prazosin, doxazosin, tamsulosin, and selective α2-blockers like yohimbine. The major uses of α-blockers include treatment of pheochromocytoma, hypertension, peripheral vascular disease, benign prostatic hyperplasia, migraine, and congestive heart failure. Common side effects include hypotension





























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











