Download as PDF, PPTX
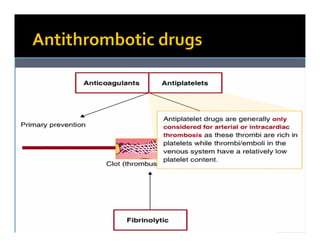
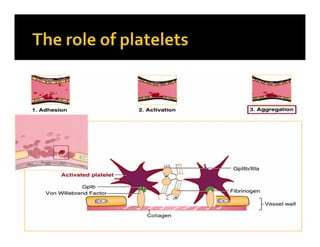
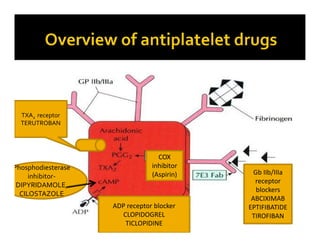


This document discusses various antiplatelet and antithrombotic drugs used to prevent thrombosis. It describes the mechanisms and indications for aspirin, clopidogrel, ticlopidine, cilostazol, abciximab, eptifibatide, tirofiban, terutroban, and dipyridamole. It also briefly mentions prasugrel and ticagrelor, newer P2Y12 receptor antagonists with more rapid onset of action than clopidogrel. The document lists common indications for antiplatelet therapy as myocardial infarction, unstable angina, coronary artery bypass grafts, prosthetic heart valves, venous thromboembolism, and transient ischemic











































































































