Downloaded 375 times
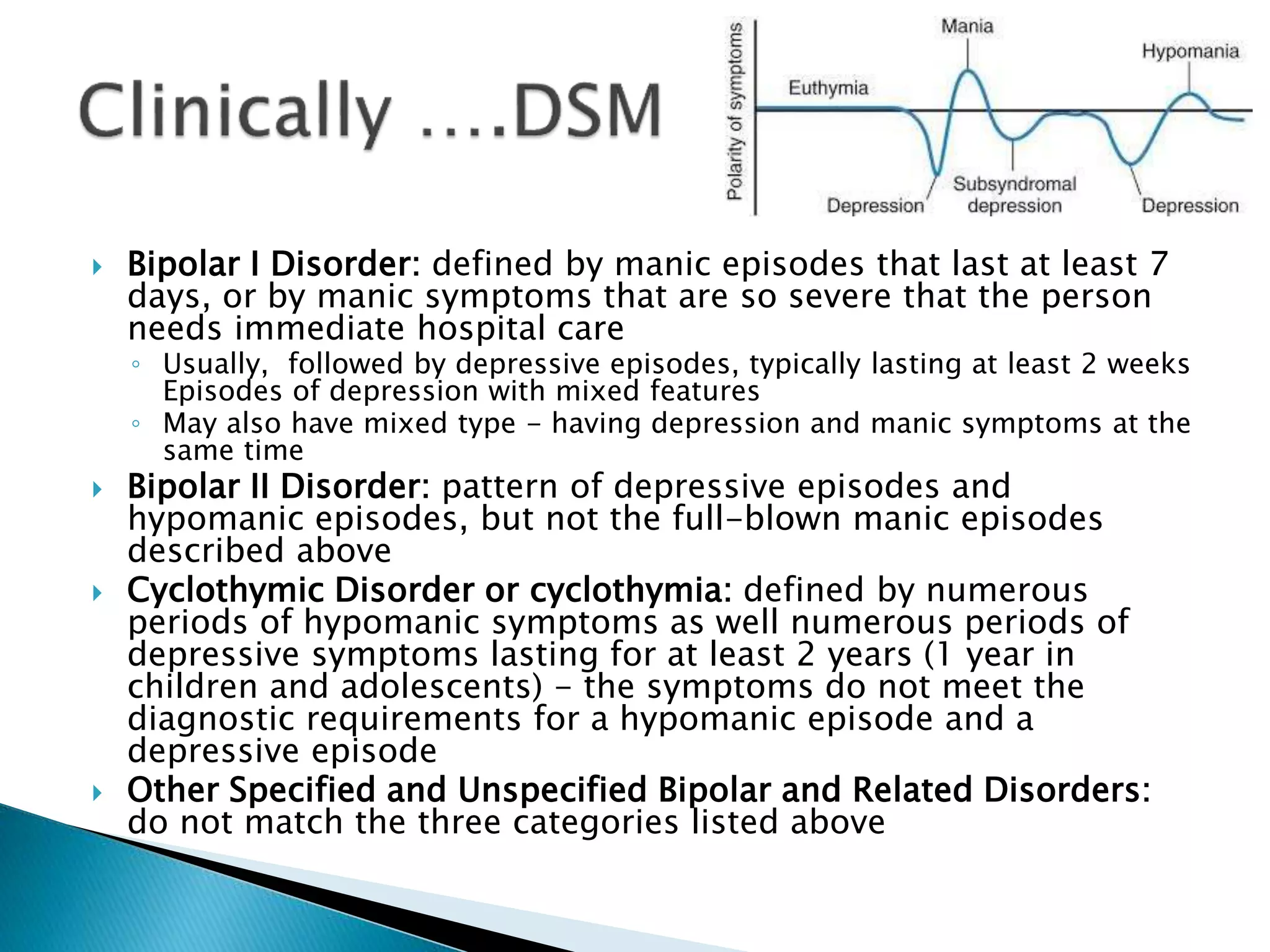












The document provides an overview of bipolar disorders, including types such as Bipolar I, Bipolar II, and cyclothymic disorder, characterizing them by their mood fluctuations. It discusses treatment options including lithium carbonate, mood stabilizers, and alternative drugs, detailing their mechanisms, dosages, side effects, and interactions. The document also highlights the importance of monitoring lithium levels due to its narrow margin of safety and outlines the efficacy of various medications in the management of bipolar episodes.























































































