Downloaded 1,360 times






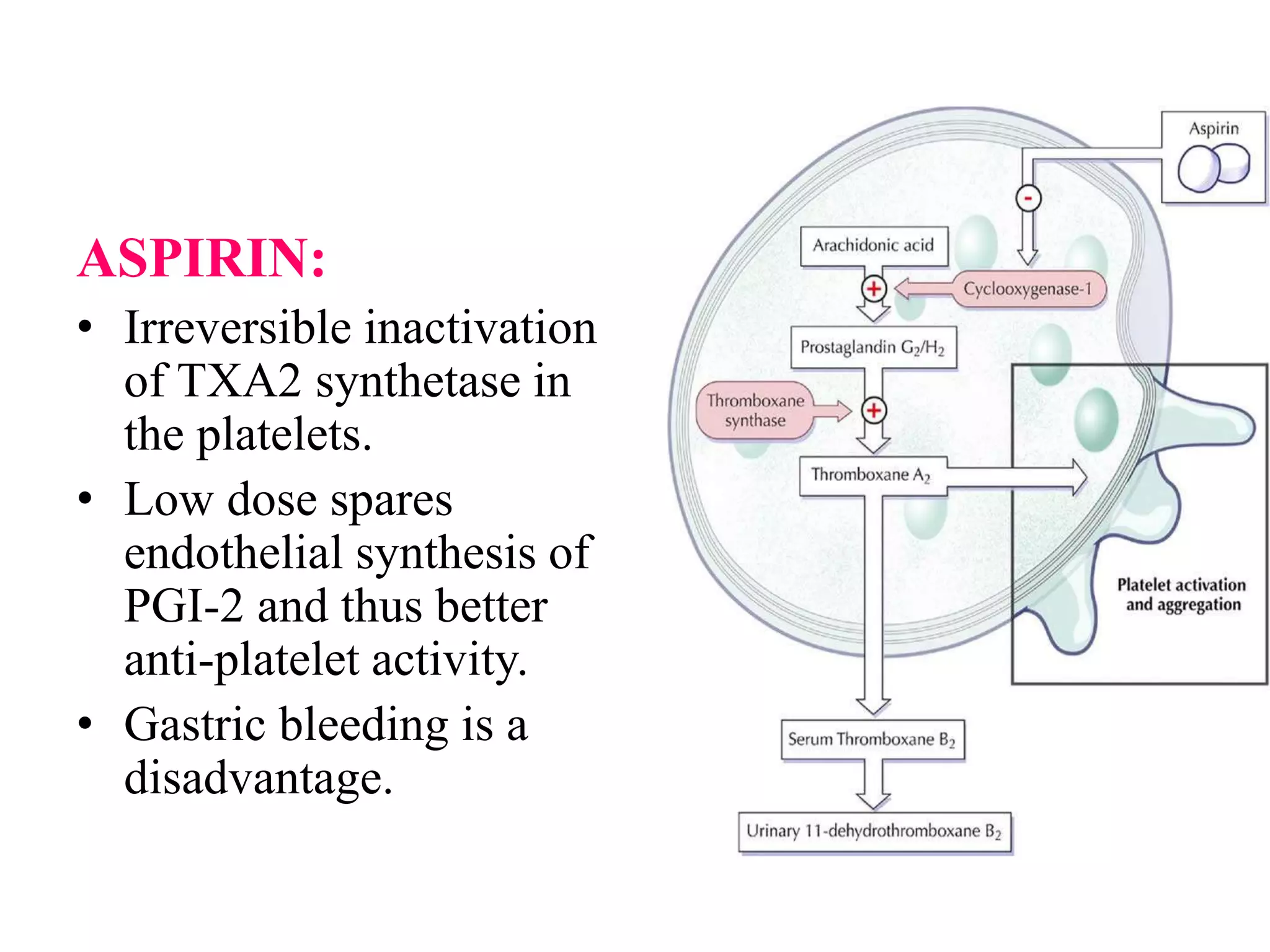
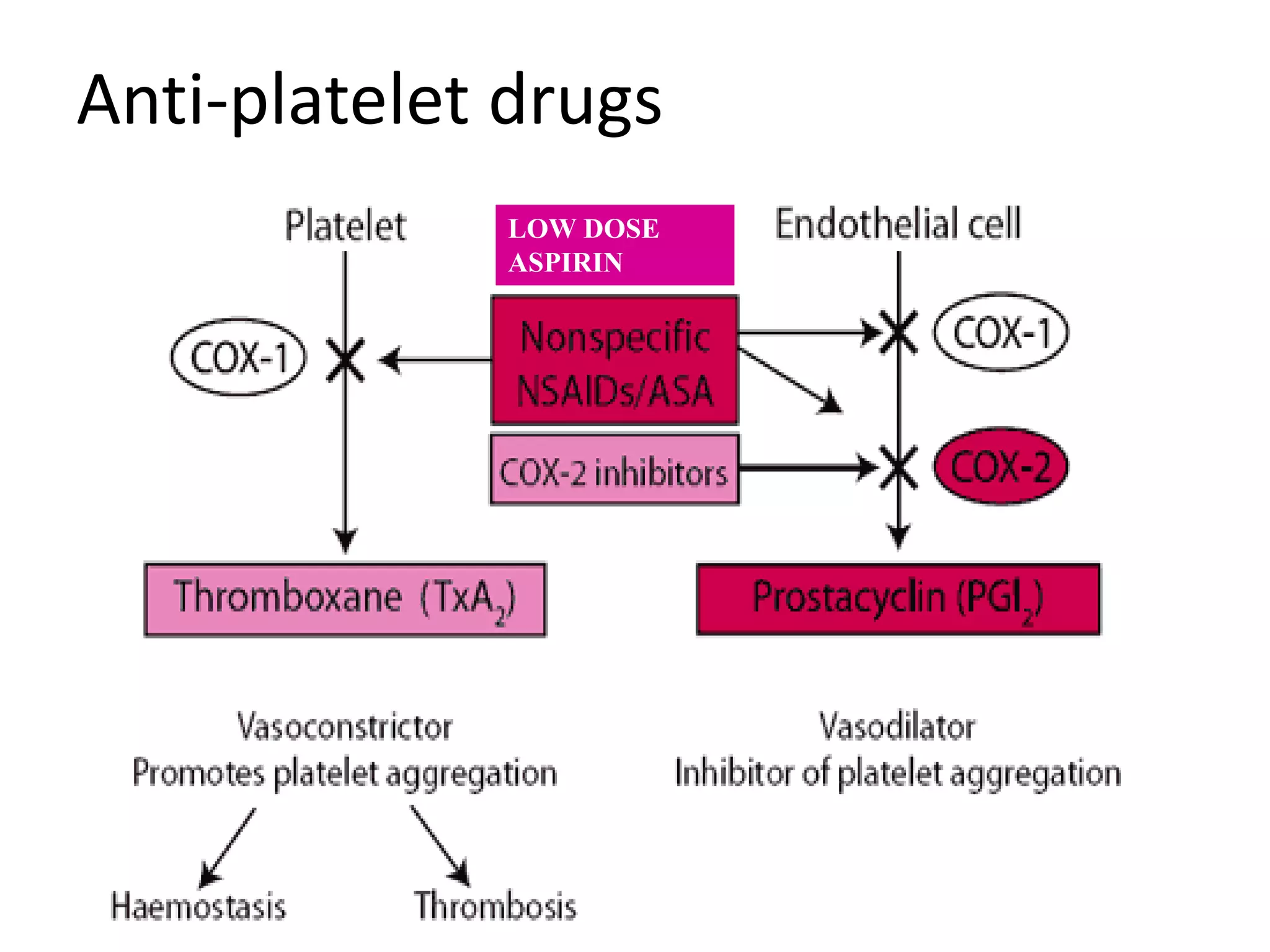
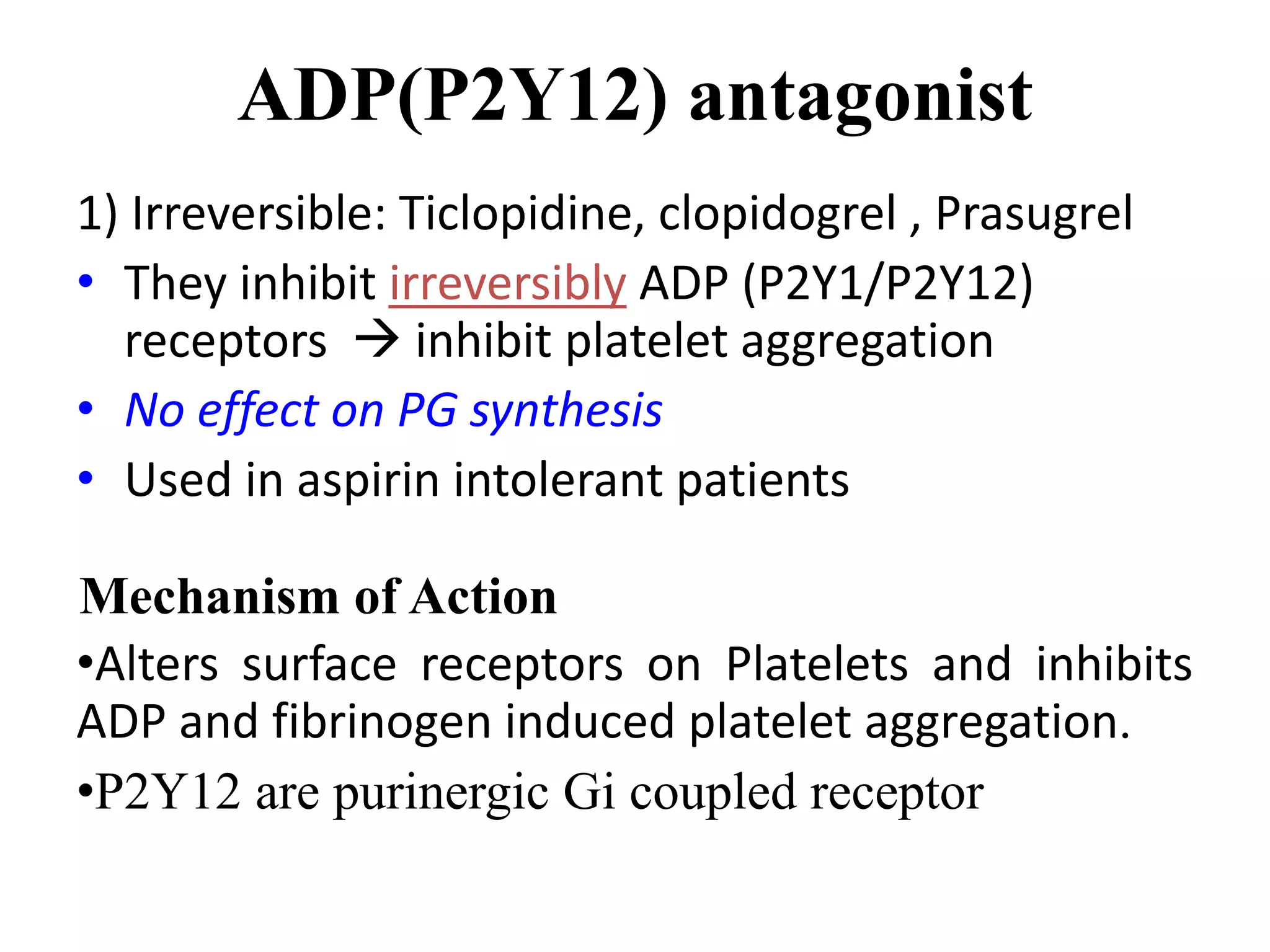




















Antiplatelet drugs reduce platelet aggregation and thrombus formation, playing a vital role in preventing life-threatening conditions like myocardial infarction and stroke. Major classes include cyclooxygenase inhibitors (e.g., aspirin), ADP receptor inhibitors (e.g., clopidogrel), and glycoprotein IIb/IIIa inhibitors, each with different mechanisms and uses. Aspirin irreversibly inhibits thromboxane A2 synthesis in platelets, while newer agents provide alternatives for patients with aspirin intolerance or specific coronary disease scenarios.









































































