Downloaded 1,139 times





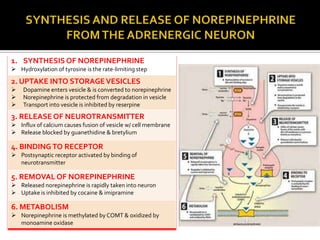

























The document discusses adrenergic drugs and their mechanisms of action. It notes that some adrenergic drugs act directly on adrenergic receptors to activate them, while others block receptor action. It provides tables listing examples of direct-acting, indirect-acting, and mixed-action adrenergic agonists. The document then discusses specific adrenergic drugs in more detail, including epinephrine, norepinephrine, isoproterenol, dopamine, dobutamine, oxymetazoline, phenylephrine, methoxamine, and clonidine. It explains their structures, receptor selectivities, and physiological effects.



































































