Acne vulgaris
•
22 likes•13,037 views

This document provides information on acne vulgaris (acne), including its definition, incidence, anatomy and physiology of the skin, etiology, types, pathophysiology, clinical manifestations, assessment, medical and surgical management, and nursing management. It defines acne as a common skin disease characterized by areas of skin with seborrhea, comedones (blackheads and whiteheads), papules, pustules, nodules and possible scarring. It affects many adolescents and young adults due to increased hormonal activity during puberty which can overstimulate sebum production in hair follicles, sometimes leading to follicular blockage and inflammation. Treatment involves reducing bacteria, sebum production, inflammation and scarring

Recommended
More Related Content
What's hot
Similar to Acne vulgaris
Similar to Acne vulgaris (20)
More from OM VERMA
More from OM VERMA (20)
Recently uploaded
Recently uploaded (20)
Acne vulgaris
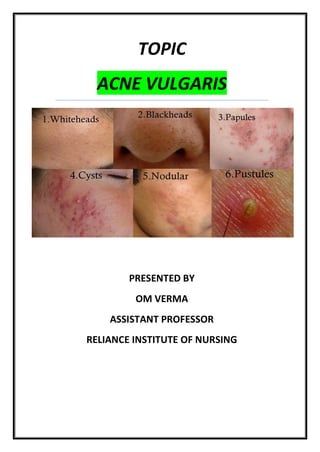
- 1. TOPIC ACNE VULGARIS PRESENTED BY OM VERMA ASSISTANT PROFESSOR RELIANCE INSTITUTE OF NURSING
- 2. ACNE VULGARIS INTRODUCTION :- Acne vulgaris is a common human skin disease that affects the areas of skin with the denset population of sebaceous follicles,these areas includes the face,the upper part of the chest & the back. DEFINITION :- 1) “ Acne vulgaris is a common human skin disease,characterized by areas of skin with Seborrhea (scaly red skin),Comedones (Blackheads & whiteheads), papules (pinheads),Pustules (pimples),Nodules (large papules) & possibly scarring.” - en.wikipedia.org/wiki/Acne_vulgaris 2) “ Acne vulgaris is a common follicular disorders affecting susceptible hair follicles,most commonly found on the face,neck & upper trunk.It is characterized by Comedones,both closed & open & by papules,pustules, nodules & cysts.” - Brunner & Suddarth’s 3) “ Acne vulgaris is a inflammatory disease of skin,caused by chronic sebaceous gland inflammation,characterized by comedones,papules & pustules of sebaceous areas i.e. face,chest,back & resolving with scaring reaction.” - Medical_dictionary.thefreedictionary.com INCIDENCE :- Acne affects 40-50 million people in the United States.Acne is the most commonly encountered skin condition in adolescents & young adults between ages 12 & 35.Both genders are affected equally,although onset is slightly earlier for girls,reach puberty at a younger age than boys.
- 3. ANATOMY & PHYSIOLOGY OF SKIN :- The skin has a surface area of about 1.5-2 meter square In adults & it containes glands,hair & nails. There are 2 main layers : Epidermis & Dermis. FIG. : THE STRUCTURE OF SKIN EPIDERMIS :- The epidermis is the most superficial layers of the skin & it is the thikest on the palms of the hands & the soles of the feet. There are no blood vessels or nerve endings in the epidermis. These are several layers (strata) of cells in the epidermis,which extend from the deepest Germinative layer to the surface Stratum corneum (a thicks horny layer). The cells on the surface are flat,non-nucleated,dead cells or squames in which cytoplasm has been replaced by the fibrous protein keratin. The colour of the skin is affected by the 3 main factors :- 1. Melanin :- A dark pigment derived from the amino acid,tyrosine & secreted by Melanocytes in the deep germinative layers.It protects the skin from the harmful effects of sunlight. 2. The level of oxygenation of hemoglobin & the amount of blood circulating in the dermis give the skin its pink colour.
- 4. 3. Bile pigment in blood & Caratenes in subcutaneous fat give the skin a yellowish colour. DERMIS :- The dermis is tough & elastic. It is formed from connective tissue & the matrix contain collagen fibres interlaced with elastic fibres fibroblasts,macrophages & mast cells are main cells found in the dermis. The structure in dermis are :- 1. BLOOD VESSELS :- Arterioles from a fine network with capillary branches supplying sweat glands,sebaceous glands,hair follicles & the dermis.The epidermis has no blood supplies. 2. LYMPH VESSELES :- These form a network throughout the dermis. 3. SENSORY NERVE ENDINGS :- Sensory receptors which are sensitive to touch, change in temp.,pressure & pain are widely distributed in the dermis. 4. SWEAT GLANDS :- It is widely distributed throughout the skin & are most numerous in the palms of the hands,soles of the feet,axillae & groins.They are composed of epithelial cells.Some ducts open into the skin surface or pores & other open into the hair follicles. 5. HAIR :- These are formed by a down growth of epidermal cells into the dermis called hair follicles. 6. THE SEBACEOUS GLANDS :- These consist of secretory epithelial cells derived from the some tissue as the hair follicles.They secrete an oily substances,sebum into the hair follicles. FUNCTION’S OF THE SKIN :- 1. Protection 2. Regulation of body temperature 3. Control of body temperature 4. Formation of vitamin-D 5. Sensation 6. Absorption 7. Excretion
- 5. ETIOLOGY :- The main causes of acne is multi-factorial.Acne develops as a result of blockage in follicles.Formation of plug of keratin & sebum is the earliest change. --- Various factors that may cause acne such as : (1) Hormonal :- Hormonal activity such as Menstrual cycles, Puberty,Pregnancy & such disorders like polycystic ovary syndrome,may contribute to the formation of acne. The male hormone androgen, can over stimulate the production of sebum in some people. (2) Genetic or Heredity (3) Infectious :- Bacteria in the pores. Propionibacterium acnes is the anaerobic bacterium that causes acne. (4) Diet :- A high glycemic load diet & cow’s milk have been associated with worsening acne. (5) Drugs :- Certain drugs like corticosteroids,glucocorticoides,corticotrophin, Phenobarbital,phenytoin,lithium,isoniazid & halogens can cause acne. (6) Other precipitating factors are :- - Exposure to industrial compounds. - Trauma or rubbing from tight clothing. - Cosmetics - Emotional stress - Oil from skin care products & cosmetics - Cooking oil - High humidity or pollution
- 6. TYPES :- The two main types of lesions are Non-inflammatory and Inflammatory. (1) NON-INFLAMMATORY :- These lesions are called comedones and can result in whiteheads or blackheads. WHITEHEADS BLACKHEADS (2) INFLAMMATORY :- These are consists of pimples,papules,pustules, nodules & cysts.Nodules are large, painful, solid lesions that are lodged deep within the skin. Cysts also lay deep within the skin but are filled with pus.Both types can produce scarring. PAPULES PUSTULES
- 7. NODULES CYST PATHOPHYSIOLOGY:- During childhood,the sebaceous glands are small & non- functioning.These glands are under endocrine control,especially by the androgens. During puberty,androgens stimulate the sebaceous glands,causing them to enlarge & secrete a natural oil,sebum.which rises to the top of the hair follicles & flows out onto the skin surface. During puberty Stimulation of androgen Stimulation of sebaceous glands Enlarged glands Secretion of natural oil,sebum Flows out onto the skin
- 8. CLINICAL MANIFESTATION :- (1) The primary lesions of acne are comedones. Closed comedones i.e. whiteheads are obstructive lesions formed from lipids or oils & keratin that plug the dilated follicles.They are small & whitish papules. Open comedones i.e. blackhead,in which the contents of the ducts are in open communication with the external environment.It result not from dirt but from an accumulation of lipid,bacterial & epithelial debris. Some closed comedones may rupture,resulting in an inflammatory reaction caused by leakage of follicular contents like sebum,keratin or bacteria into the dermis. (2) Propionibacterium acne,that live in the hair follicles. (3) Erythmatous papules : mild papules heal on their own without treatment & deeper papules may result in scarring of the skin. (4) Inflammatory pustules (5) Inflammatory cysts : cyst may result in scarring of the skin. ASSESSMENT & DIAGNOSTIC FINDINGS :- The diagnosis of acne is based on the history & physical examination,evidence of lesions characteristic of acne & age. Acne does not occur until puberty. Oilyness is more prominent in the midfacial area. When there are numerous lesions,some of which are open,the person may exude a distinct sebaceous odour. Women may report a history of flare-ups a few days before menses. MEDICAL MANAGEMENT :- The goal of management are to reduce bacterial colonies,decreased sebaceous glands activity,prevent the follicles from becoming plugged,reduced inflammation,combat secondary infection,minimize scaring & eliminate factors that predispose the person to acne. The therapeutic regimen depends on the type of lesions like comedones,papules,pustules & cyst. There is no predictable cure for the disease but combinations of therapies are available that can effectively control its activity.
- 9. NUTRITION & HYGIENE THERAPY :- The restrictions of a specific food or food product associated with a flare-up of acne such as chocolate,cola,fried foods or milk products should be promoted. Maintenance of good nutrition equips the immune system for effective action against bacteria & infection. For mild case of acne,washing twice each day with a cleansing soap may be all that is required. These soaps can remove the excessive skin oil & comedo in most cases.Oil free cosmetics & creams should be chosen by the patient. TOPICAL PHARMACOLOGICAL THERAPY :- BENZOYL PEROXIDE :- Benzoyl peroxide preparations are widely used because they produce a rapid & sustained reduction of inflammatory lesions. They depress sebum production & promote breakdown of comedo plugs. They also produce an antibacterial effects by suppressing Propionibacterium acnes. Initially Benzoyl peroxide causes redness & scaling but the skin usually adjusts quickly to its use. Benzoyi peroxide,Benzoyl erythromycin & Benzoyl sulfer combination are available. Vitamin A acid applied topically is used to clear the keratin plugs. Improvement may take to 12 weeks. The patient is cautioned against sun exposure while using the topical medication because it may cause sunburn. TOPICAL ANTIBIOTICS :- Topical antibiotics suppress the growth of Propionibacterium acnes,reduce superficial free fatty acid levels,decreased comedones,papules & pustules & produce no systemic side effects. Common topical preparation includes Tetracycline,Clindamycin & Erythromycin.
- 10. SYSTEMIC PHARMACOLOGICAL THERAPY :- ANTIBIOTICS :- Oral antibiotics such as tetracycline,doxycycline,penicilline & minocycline, administered in small doses over a long period are very effective. Therapy may continue for months to year. The tetracycline is contraindicated in children younger than age 12 & in pregnant women. During pregnancy they can affect the development of teeth in infants. Side effects of tetracycline includes photosensitivity,nausea,diarrhea, coetaneous infection & vaginitis in women. In some women,broad spectrum antibiotics may suppress normal vaginal bacteria. ORAL RETINOIDS :- Synthetic vitamin A compounds i.e. Retinoids are used in patients with nodular cystic acne. Isotretinoine is also used for active inflammatory pustular acne that has a tendency to scar. It reduces sebaceous gland size & inhibit sebum production. The most common side effects are cheilitis (inflammation of the lips). HORMONE THERAPY :- Estrogen therapy including progesterone estrogen preparations suppresses sebum production & reduce skin oiliness. Estrogen is not administered to male patients because of undesirable side effects such as enlargement of breast & decrease in body hairs. surgical MANAGEMENT :- It consist of comedo extraction,injections of corticosteroids into the inflamed lesions & incision & drainage of large,fluctuant or nodular cystic lesions. Cryosurgery (i.e. freezing with liquid nitrogen)may be used for nodular & cystic acne. Patients with deep scars may be treated with abrasive therapy ( i.e. dermabrassion ),in which epidermis & some superficial dermis are removed. Comedo may be removed with a comedo extractor.
- 11. NURSING MANAGEMENT :- Major nursing activities include patient education,particularly in proper skin care techniques & managing potential problems related to the skin disorders or therapy. PREVENTING SCARING :- Prevention of scaring is the ultimate goal of therapy. The chances of scaring increases the grade of acne increases. Grade III & IV ( 25 to more than 50 comedones,papules or pustules ) usually require longer term therapy with systemic antibiotics. Patient should be warned that discontinuing these medications can increase the chances of deep scaring. Hyperpigmentation or hypopigmentation also may affect the tissue involved. PREVENTING INFECTION :- Female patient receiving long term antibiotic therapy with tetracycline should be advised to watch sign & symptoms of oral or vaginal candidiasis,a yeast like fungal infection. PROMOTING HOME & COMMUNITY BASED CARE :- Patients are instructed to wash the face & other affected areas with mild soap & water twice each day to remove surface oils. They are cautioned to avoid scrubbing the face because acne is not caused by dirt & cannot be washed away. Mild abrasive soaps & drying agents are prescribed to eliminate the oily feeling. Patient are instructed to avoid excessive abrasion because it causes minute scratches on the skin surface. All forms of friction & trauma are avoided,including propping the hands against the face,rubbing the face & wearing tight collars & helmets. Patients are instructed to avoid manipulation of pimples or blackheads. Cosmetics,shaving creams & lotions can aggravate acne,these substances are best avoided.
- 12. THANK YOU CLASS