Downloaded 1,160 times






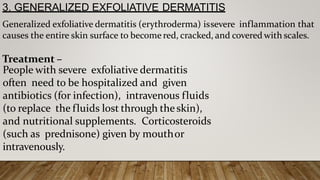







![CONCLUSIONS–
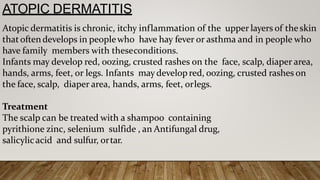
Atopic dermatitis can be treated by following a few basic rules
regarding skin hydration, use of a moisturizer, and topical steroid applications
to reduce inflammation. The distinction between the various types of contact
dermatitis is based on a number of factors. these findings have been
acknowledged not to distinguish [9], and even positive patch testing does not
rule out the existence of an irritant form of dermatitis as well as an
immunological one. It is important to remember, therefore, that the
distinction between the types of contact dermatitis is often blurred, with, for
example, certain immunological mechanisms also being involved in a case of
irritantcontactdermatitis.](https://image.slidesharecdn.com/dermatitis-200821072520/85/Dermatitis-ppt-52-320.jpg)


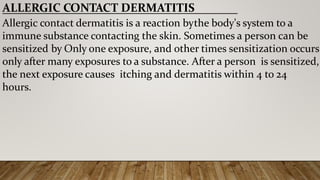
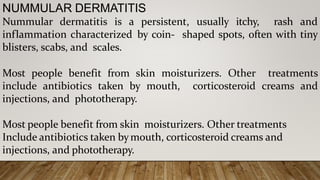
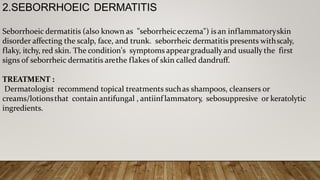
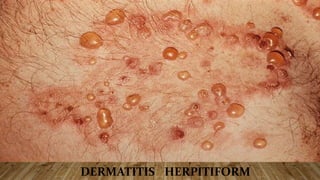
Dermatitis is an inflammation of the skin that causes redness, swelling and itchiness. There are many types of dermatitis including atopic dermatitis, contact dermatitis and seborrheic dermatitis. Contact dermatitis occurs when the skin comes into contact with an irritant or allergen and can be either irritant or allergic in nature. Symptoms vary depending on the type but may include a rash, blisters, dry cracked skin and itchiness. Treatment involves identifying and avoiding triggers, using moisturizers and topical or oral medications like corticosteroids and antihistamines.























































































