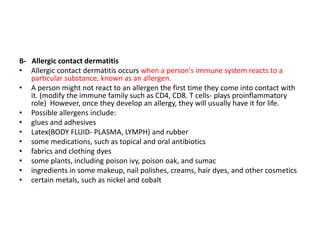
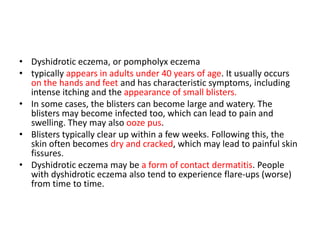
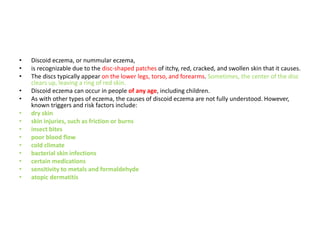
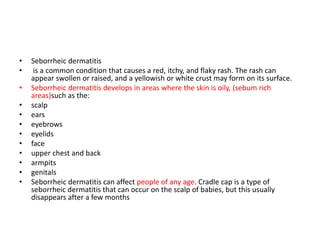
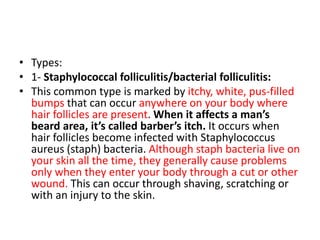
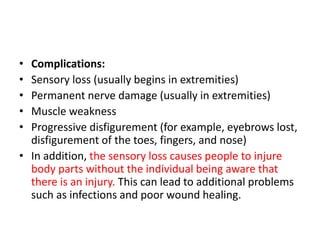
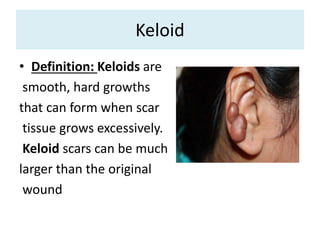
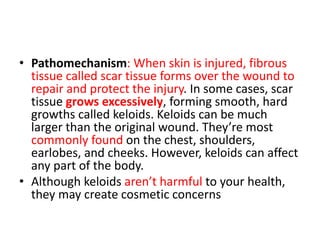
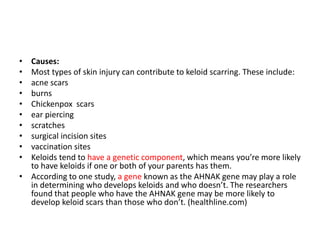
The document discusses different types of skin diseases, focusing on eczema. It defines eczema as a group of conditions that cause red, itchy, and inflamed skin. The document outlines several types of eczema including atopic dermatitis, contact dermatitis, dyshidrotic eczema, discoid eczema, seborrheic dermatitis, and varicose eczema. It describes the symptoms, causes, diagnosis, and potential complications of each type of eczema. The causes discussed include genes, environmental triggers, allergens, hormones, and immune system overactivity. Diagnosis involves medical history, physical examination, and sometimes patch testing.

















![• Treatment:
• Corticosteroid injections (intralesional steroids): These are safe but
moderately painful. Injections are usually given once every four to eight
weeks into the keloids) and usually help flatten keloids; however, steroid
injections can also make the flattened keloid redder by stimulating the
formation of more superficial blood vessels. (These can be treated using a
laser. The keloid may look better after treatment than it looked to start
with, but even the best results leave a mark that looks and feels quite
different from the surrounding skin.
• Laser: The pulsed-dye laser can be effective at flattening keloids and
making them look less red. Treatment is safe and not very painful, but
several treatment sessions may be needed. These may be costly, since
such treatments are not generally covered by insurance plans.
• [The pulsed-dye laser for treatment of cutaneous conditions, PDL uses a
concentrated beam of light that targets blood vessels in the skin]](https://image.slidesharecdn.com/4thproff-3-190511195615/85/Skin-Diseases-155-320.jpg)