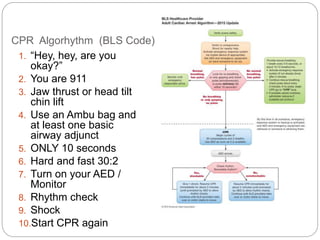
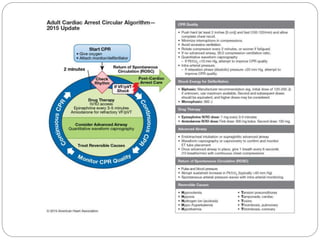
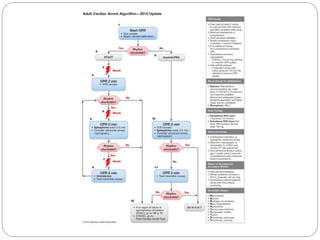
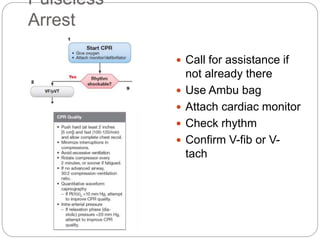
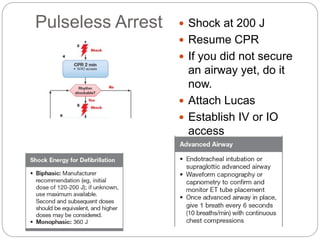
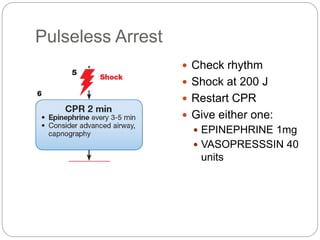
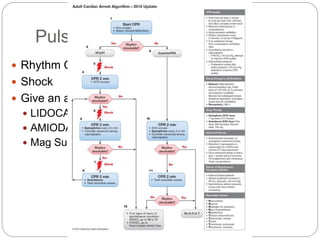
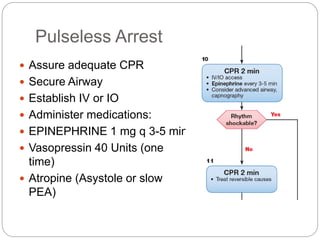
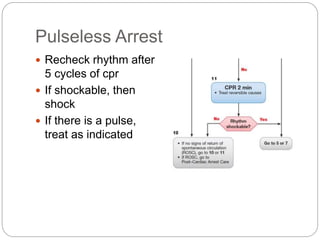
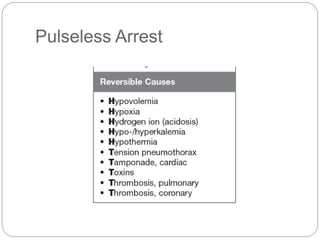
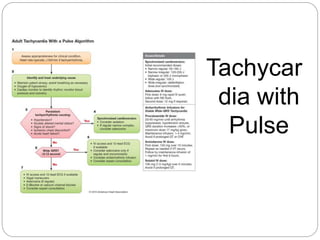
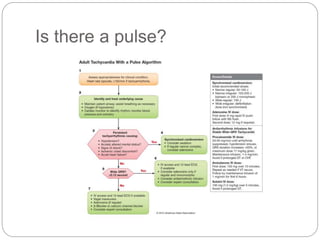
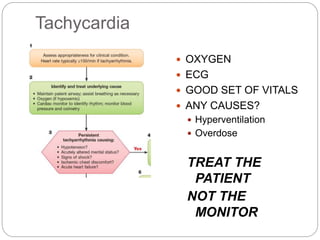
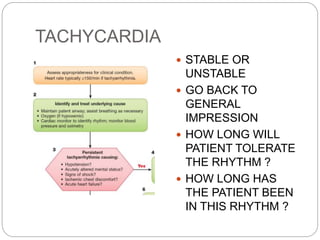
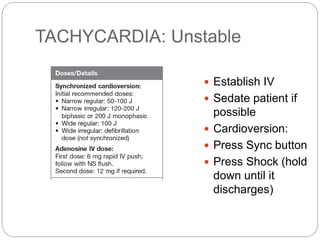
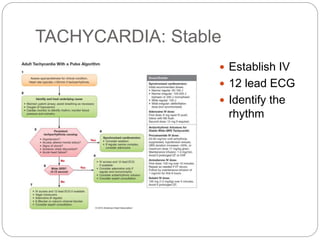
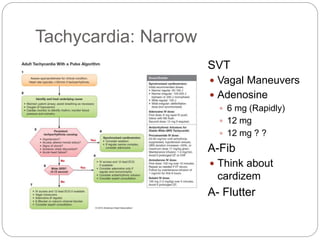
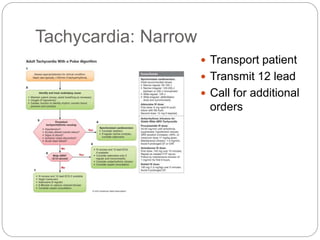
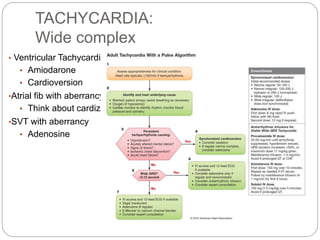
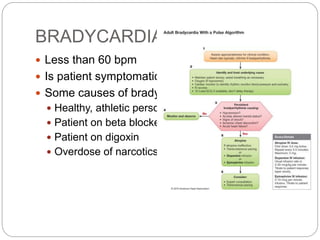
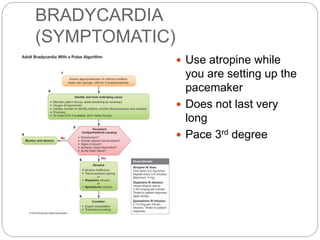
This document provides guidelines and algorithms for paramedics on Advanced Cardiac Life Support (ACLS). It outlines the main algorithms for cardiopulmonary resuscitation (CPR), pulseless arrest, tachycardia with a pulse, bradycardia, and return of spontaneous circulation (ROSC). For each condition, it lists the steps for assessment, treatment, and medications. Key treatments include defibrillation, cardioversion, intubation, intravenous access, pacing, epinephrine, amiodarone, atropine, and addressing reversible causes. The goal is to follow standardized procedures to properly diagnose and treat life-threatening cardiac arrhythmias or arrest.







































































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)




