#2 Lecture Outline
I. Introduction
A. The term cardiovascular disease (CVD) refers to a group of disorders of the heart and blood vessels.
1. Coronary heart disease (CHD) is a type of CVD that includes disease of the coronary arteries.
#3 Lecture Outline
2. AMI occurs when sudden narrowing or complete blockage of a coronary artery causes myocardial tissue death.
a. It is estimated that one person has an AMI in the United States about every 40 seconds.
#4 Lecture Outline
3. Cardiac arrest is the cessation of cardiac mechanical activity, as confirmed by the absence of signs of circulation.
a. In the United States, most out-of-hospital cardiac arrests (OHCAs) occur in a home or residence, followed by public settings, and then nursing homes.
#5 Lecture Outline
II. Anatomy and Physiology Review
A. Structure and function
1. Cardiovascular system
a. Composed of heart and blood vessels
b. Primary function is to deliver oxygenated blood and nutrients to cells in the body
i. Responsible for delivering hormones
ii. Transports metabolism waste products from cells to recycling or waste disposal sites
#6 Lecture Outline
B. The heart
1. The heart has four chambers.
#8 Lecture Outline
a. Right atrium
i. Receives blood low in oxygen from the superior vena cava, inferior vena cava, and the coronary sinus
b. Left atrium
i. Receives freshly oxygenated blood from the lungs by way of the right and left pulmonary veins
ii. The atria then contract, pumping blood through the AV valve into the ventricles.
#9 Lecture Outline
c. Right ventricle
i. Pumps deoxygenated blood to the lungs
d. Left ventricle
i. Pumps oxygenated blood throughout the body
ii. When the left ventricle contracts, it produces an impulse palpable at the apex of the heart (apical impulse).
(a) Also called the point of maximal impulse (PMI)
2. A septum separates the right and left sides of the heart.
a. The interatrial septum separates the right and left atria.
b. The interventricular septum separates the right and left ventricles.
#10 Lecture Outline
3. The septa separate the heart into two functional pumps.
a. The right atrium and right ventricle compose one pump.
i. Sometimes called the “right heart”
ii. A low-pressure system (pulmonary circulation)
b. The left atrium and left ventricle compose the other.
i. Sometimes called the “left heart”
ii. A high-pressure pump (systemic circulation)
#11 Lecture Outline
4. The myocardium is the middle layer of the heart wall.
a. Comprises mostly thick cardiac muscle tissue
b. Responsible for cardiac contraction and efficient ejection of blood from the heart
#12 Lecture Outline
5. There are two main coronary arteries that supply blood to the tissues of the heart.
a. The left main coronary artery (LMCA)
i. The largest in diameter and shortest of the myocardial blood vessels
ii. Divides into the left anterior descending artery (LAD) and the circumflex artery (Cx)
iii. The areas supplied by the coronary arteries differ among patients.
(a) The LAD supplies blood to the anterior surface of the left ventricle, part of the lateral surface of the left ventricle, and a portion of the interventricular septum in most patients.
(b) The Cx artery supplies the left atrium, part of the lateral surface of the left ventricle, the inferior surface of the left ventricle in about 15% of people, the posterior surface of the left ventricle in 15% of people, the sinoatrial (SA) node in about 40% of people, and the AV bundle in 10% to 15% of people.
b. The right coronary artery (RCA)
i. Branches supply blood to the walls of the right atrium and ventricle, a portion of the inferior part of the left ventricle, and portions of the conduction system (the SA node in about 60% of people and the AV bundle in about 85% to 90% of people).
#13 Lecture Outline
6. Cardiac cells have four important properties that help the heart function efficiently.
a. Automaticity
b. Excitability
c. Conductivity
d. Contractility
#14 Lecture Outline
7. The cardiac conduction system comprises six parts:
a. The SA node
b. The AV node
c. The bundle of His
d. The right bundle branches
e. The left bundle branches
f. The Purkinje fibers
#15 Lecture Outline
8. Sympathetic or parasympathetic nerves are stimulated.
a. Stimulation of sympathetic nerves
i. Strengthens the force of contraction
ii. Increases the heart rate
#16 Lecture Outline
b. Stimulation of parasympathetic nerves
i. Slows the rate of discharge of the SA node
ii. Slows conduction through the AV node
iii. Weakens the strength of atrial contraction
iv. Can cause a small reduction in the force of ventricular contraction
#18 Lecture Outline
A. Common reason to seek medical care
1. A patient with cardiovascular-related symptoms may be a young, middle-aged, or older adult.
2. A systematic approach to patient assessment is important.
B. Primary survey
1. The order of the steps for performing a primary survey differs depending on the type of cardiac patient.
2. The order of steps in the primary survey is usually ABCDE (assess airway, breathing, and then circulation, disability, and exposure).
a. If the patient is found unresponsive and is suspected of being in cardiac arrest, the order changes to CABDE.
#19 Lecture Outline
C. History taking
1. Acute coronary syndromes (ACSs) are a series of cardiac conditions that are caused by an abrupt reduction in blood flow through a coronary artery.
2. There are three major ACSs:
a. Unstable angina
b. Non–ST segment elevation myocardial infarction (NSTEMI)
c. ST segment elevation myocardial infarction (STEMI)
#20 Lecture Outline
3. Common chief complaints in the patient experiencing an ACS include chest discomfort, dyspnea, fainting, palpitations, and fatigue.
a. Chest pain or discomfort is often the presenting symptom in a patient with ACS.
i. The description of discomfort is for assessing its significance.
ii. OPQRST (Onset, Provocation/palliation, Quality, Region/radiation, Severity, Timing)
iii. If the patient has more than one chief complaint, ask the patient:
(a) Which symptom started first
(b) Which bothers them the most
b. Dyspnea is another chief complaint in ACS.
i. May vary in intensity
ii. Difficult to assess because it is a sign and not a symptom
iii. Ask the patient to rate the severity on a scale of 0 to 10.
iv. Dyspnea that develops suddenly suggests:
(a) Pulmonary embolism
(b) Pneumothorax
(c) Acute pulmonary edema
(d) Pneumonia
(e) Airway obstruction
v. Dyspnea that occurs on exertion or at rest suggests COPD or left ventricular failure (LVF).
vi. Orthopnea is a type of dyspnea that is relieved by a change in position.
vii. Paroxysmal nocturnal dyspnea (PND) is a sudden onset of difficulty breathing in which the patient suddenly awakens from sleep.
(a) Associated with LVF
(b) Usually begins 2 to 4 hours after the onset of sleep
(c) Often accompanied by coughing, wheezing, and sweating
(d) A feeling of suffocation upon awakening
(e) Usually improves after sitting up or standing for 15 to 30 minutes
4. If your patient has a cough, then find out whether it is dry or productive.
#21 Lecture Outline
5. If your patient has fainted, try to determine whether the patient fainted from cardiac or noncardiac causes.
a. Cardiac causes of syncope include dysrhythmias, increased vagal tone, and heart lesions.
b. Consider a cardiac cause if fainting occurs in a recumbent position, is provoked by exercise, is associated with chest pain, or if a family history of fainting or sudden death is present.
#22 Lecture Outline
6. Patients with cardiac problems may present with a chief complaint of palpitations.
a. Can be caused by:
i. Anxiety
ii. Lack of sleep
iii. Certain medicines
iv. Caffeine
v. Stress
vi. Cocaine or amphetamine use
vii. Heavy cigarette smoking
viii. Metabolic conditions (hyperthyroidism)
ix. Changes in the heart’s rhythm or rate, including fast rhythms (tachycardias) and early beats
7. Ask about the onset, frequency, and duration of this symptom and previous episodes of palpitations.
8. Ask about the presence of associated symptoms such as chest discomfort, dizziness, syncope, and dyspnea.
9. Fatigue is a common complaint in patients with impaired cardiovascular functions.
a. Ask when the patient’s fatigue began and how long it has been present.
b. Ask about associated symptoms such as chest discomfort, nausea, dyspnea, syncope, or palpitations.
#23 Lecture Outline
10. Patients may report a variety of other related symptoms including:
a. Feelings of impending doom
b. Nausea or vomiting
c. Trauma involvement
d. Hypoxia or poor perfusion
11. Inquire about pertinent aspects of the patient’s other medical history.
a. Medications
i. Is the patient taking as instructed?
ii. When did the patient last take them?
iii. Is the patient taking medications prescribed for someone else?
#24 Lecture Outline
12. Common cardiac medications include the following:
a. Antiarrhythmics such as digoxin (Lanoxin), procainamide (Procan, Pronestyl), amiodarone (Cordarone), and verapamil (Calan, Isoptin, Verelan)
b. Anticoagulants such as enoxaparin (Lovenox), clopidogrel (Plavix), and warfarin (Coumadin)
c. Angiotensin-converting enzyme inhibitors such as captopril (Capoten), enalapril (Vasotec), and lisinopril (Prinivil, Zestril)
d. Beta-blockers such as atenolol (Tenormin), metoprolol (Lopressor), and propranolol (Inderal)
e. Lipid-lowering agents such as gemfibrozil (Lopid), atorvastatin (Lipitor), fluvastatin (Lescol), lovastatin (Mevacor), pravastatin (Pravachol), rosuvastatin calcium (Crestor), and simvastatin (Zocor)
f. Diuretics such as furosemide (Lasix) or hydrochlorothiazide (HCTZ)
g. Vasodilators such as nitroglycerin (Nitrostat) or isosorbide (Isordil)
13. Ask about noncardiac medications.
a. Over-the-counter medications
i. Phosphodiesterase inhibitors such as sildenafil (Viagra), tadalafil (Cialis), or vardenafil (Levitra) combined with certain vasodilators can cause a sudden drop in blood pressure.
b. Herbal supplements
i. Can cause serious, and even fatal, interactions when taken with certain cardiac medications
c. Recreational drugs
#25 Lecture Outline
14. Ask specifically whether the patient has ever been diagnosed with any of the following:
a. Aneurysm
b. Atherosclerotic heart disease: angina, previous MI, hypertension, heart failure
c. Congenital anomalies
d. CAD
e. Diabetes
f. Inflammatory cardiac disease
g. Previous cardiac surgery (coronary artery bypass graft or valve replacement)
h. Pulmonary disease
i. Renal disease
j. Valvular disease
k. Vascular disease
#26 Lecture Outline
D. Secondary assessment
1. The physical exam for a patient with cardiac complaints should emphasize that condition.
2. Skin color and temperature may indicate circulation problems.
a. Patient with low CO and inadequate tissue perfusion may present with pale, mottled, or cyanotic skin
b. Flushed, warm skin may be a sign of infection such as pericarditis
#27 Lecture Outline
3. A physical exam includes the following steps:
a. Inspect the neck and tracheal position.
b. Inspect adjacent structures, such as neck veins.
i. To estimate jugular venous pressure:
(a) Place the patient in a semi-Fowler position with the head slightly rotated away from the vein.
(b) Observe the height of the distended fluid column in the vein.
(c) Note how far up the distention extends above the sternal angle.
c. Inspect and palpate the chest.
i. Look for surgical scars indicating previous cardiac surgery.
ii. Check for an NTG patch on the skin.
iii. Look for a pacemaker or implantable defibrillator.
iv. Check for chest enlargement or a barrel-chest (as in COPD).
v. Observe for any sign of crepitus.
#28 Lecture Outline
d. Listen to the chest with the stethoscope.
i. Crackles or wheezes may indicate LVF with pulmonary edema.
e. Inspect and lightly palpate the patient’s abdomen for distention and pulsations.
i. Strong pulsations in the epigastric area may be a sign of an abdominal aortic aneurysm.
f. Check for swelling in the patient’s arms, hands, legs, feet, ankles, and sacral area.
i. Bilateral pitting edema may be a sign of right ventricular failure (RVF).
ii. Pitting edema limited to one side of the body suggests a blockage in a major vein.
#29 Lecture Outline
g. Use the following monitoring devices:
i. Cardiac monitor, waveform capnography, and pulse oximeter
#30 Lecture Outline
E. Pulse findings in cardiac patients
1. Determine if there is a pulse deficit.
a. Difference between the apical pulse and the peripheral pulse
2. Check the patient’s blood pressure.
a. Pulsus paradoxus occurs when the systolic blood pressure falls more than 10 mm Hg with inspiration.
c. Cardiac conditions in which this finding may be present include AMI, cardiogenic shock, cardiac tamponade, and constrictive pericarditis.
3. Check for a beat-to-beat difference in the strength of a pulse.
a. This is pulsus alternans and may be a sign of severe ventricular failure.
#31 Lecture Outline
F. Blood pressure findings in cardiac patients
1. A normal SBP is less than 120 mm Hg, and a normal diastolic blood pressure (DBP) is less than 80 mm Hg.
2. An SBP of 140 mm Hg or higher or a DBP of 90 mm Hg indicates stage 2 hypertension.
#32 Lecture Outline
3. In emergencies:
a. Elevated blood pressure may be from anxiety or pain.
b. SBP lower than 90 mm Hg may be hypotension or shock.
c. Widened pulse pressure may be seen in conditions such as the later stages of shock.
d. Narrowed pulse pressure may be seen in conditions such as tachycardia and cardiac tamponade.
4. If possible, obtain and compare blood pressure in both arms.
#33 Lecture Outline
G. Assessment of heart sounds
1. S1 heart sounds occur near the beginning of the ventricular contraction when the tricuspid and mitral valves close.
a. The sound of the tricuspid valve’s closing may be louder in cases of hypertension.
b. S1 sounds may be louder in patients with anemia, a fever, or hyperthyroidism, as well as patients with stenosis of their mitral valve.
c. Decreased S1 sounds can indicate:
i. Fibrotic or calcified mitral valve
ii. Obesity
iii. Emphysema
iv. Cardiac tamponade
d. A split sound from any delay in the closing of both valves is considered abnormal.
#34 Lecture Outline
2. S2 heart sounds occur near the end of ventricular contraction when the pulmonary and aortic valves close.
a. Louder in patients with chronic high blood pressure or pulmonary hypertension
b. Decreased in patients with hypotension
c. Split in the case of a right bundle branch, resulting in a delay in the pulmonic valve closing
d. The aortic valve may close more slowly than the pulmonic valve in situations involving left bundle branch blocks.
#35 Lecture Outline
3. S3 is an extra, abnormal heart sound in adults caused by ventricular wall vibrations resulting from a rapid filling period of the ventricle during the beginning of diastole.
a. It is often associated with heart failure.
4. S4 is a rare heart sound heard just before S1 and is caused by turbulent filling of a stiff ventricle in hypertrophy and possible myocardial infarction.
#36 Lecture Outline
5. A murmur is a sound from turbulent blood flow through the valves caused by:
a. Increased blood flow across a normal valve
b. Flow across an irregular or constricted valve
c. Blood flow into an enlarged heart chamber
d. Backward blood flow through a compromised valve
#37 Lecture Outline
H. Reassessment
1. Reassessment should be done on the way to the hospital.
2. Prepare proper documentation of the call and notify the receiving facility of any history findings, physical exam findings, and cardiac monitoring or ECG findings.
#39 Lecture Outline
A. The mechanical pumping action of the heart
1. Can occur only in response to an electrical stimulus
2. This impulse causes the heart to beat because of a series of complex chemical changes within the myocardial cells.
B. Depolarization and repolarization
1. Depolarization is the process of discharging resting cardiac muscle fibers by means of an electrical impulse that stimulates contraction.
a. Myocardial cells are bathed in an electrolyte solution.
b. Chemical pumps inside the cell maintain the concentrations of ions, which creates an electric gradient across the cell membrane.
c. A polarized cell normally has a net internal charge of –90 mV.
#40 Lecture Outline
d. When the myocardial cell receives a stimulus from conduction, the permeability of the cell wall changes to allow Na+ in.
i. Makes the cell more positive
e. Ca+2 also enter, which helps maintain the depolarized state of the cell membrane.
f. This depolarization spreads along the cell until it is completely depolarized, causing a mechanical contraction.
#41 Lecture Outline
2. Repolarization begins with the closing of the sodium and calcium channels to stop the inflow of these ions.
a. Potassium channels open to allow the escape K+ to help restore a negative charge to the inside of the cell.
b. Sodium ions are pumped out and potassium ions are pumped back into the cell, reestablishing the proper electrolyte distribution.
c. After the potassium channels close, the sodium-potassium pump helps move sodium and potassium ions back to their respective locations, which maintains the polarity of the cell membrane.
#42 Lecture Outline
C. Cardiac action potential
1. The action potential of a typical myocardial cell can be divided into five phases: phase 0 to phase 4.
a. Phase 0
i. Begins when the cardiac muscle cell receives an impulse
ii. Na+ moves into the cell through sodium channels, causing the interior of the cell to become electrically positive relative to its exterior.
iii. The transmembrane potential (TMP) changes from −90 mV to about −70 mV.
iv. At threshold, still more Na+ channels open, allowing a rapid influx of Na+ and a rapid rise in membrane voltage to about + 30 mV.
v. At the same time, Ca++ enters more slowly through calcium channels.
vi. The influx of Ca++ causes the sarcoplasmic reticulum to release calcium for muscle contraction.
vii. The cell depolarizes and begins to contract.
viii. On an ECG, the QRS complex represents phase 0.
b. Phase 1
i. Inward sodium channels close and the cell begins to repolarize.
ii. Negatively charged chloride ions enter the cell.
iii. Outward potassium channels open briefly, allowing K+ to leave the cell and resulting in a decrease in the TMP.
c. Phase 2
i. The plateau phase, is the longest phase of the action potential.
ii. Na+ and Ca++ slowly enter the cell, while K+ flows out of the cell.
iii. The presence of Ca++ prolongs depolarization of the membrane, creating a plateau.
iv. Contraction ends when the outward flow of K+ exceeds the inward flow of Na+ and Ca++.
v. Corresponds to the ST segment on the ECG
d. Phase 3
i. Final phase of repolarization
ii. Slow calcium channels gradually close, and Ca++ is transported out of the cell.
iii. Potassium channels open, and the rapid movement of K+ out of the cell causes the TMP to become increasingly negative.
iv. By the end of this phase, the membrane potential has been restored to its resting value.
v. With repolarization complete, the cell can now respond to a new stimulus.
vi. On an ECG, the T wave represents phase 3.
e. Phase 4
i. Called the resting phase, it represents the normal working myocardial cell at its resting membrane potential of −90 mV.
#43 Lecture Outline
D. Refractory periods
1. The periods during which the cell is depolarized or in the process of repolarizing
2. It consists of two phases.
a. The first half represents the absolute refractory period, a period of time (from phase 0 to the middle of phase 3) in which the ventricles have not sufficiently repolarized to enable another depolarization.
b. The second half represents the relative refractory period (middle of phase 3 to the beginning of phase 4), which indicates that some cells have repolarized sufficiently to depolarize again.
#44 Lecture Outline
E. The conduction system
1. Specialized conduction tissue made up of specialized pacemaker cells
a. The pacemaker is the area of conduction tissue in which the electrical activity arises; it sets the pace for cardiac contraction.
2. The dominant pacemaker: the SA node
a. Lies at the junction of the superior vena cava and the right atrium
i. It receives blood from the RCA.
ii. In about 0.08 seconds, electrical impulses generated in the SA spread across the atria and advance through three internodal pathways.
iii. The three pathways include the anterior internodal pathway, middle internodal tract, and thorel tract.
#45 Lecture Outline
b. The AV node is located in the floor of the right atrium behind the tricuspid valve, near the opening of the coronary sinus.
i. When the impulse from the SA node enters the AV node, it is delayed for about 0.12 seconds before it is relayed through the rest of the conduction system.
ii. This delay allows the atria to empty blood into the ventricles.
iii. About 70% to 80% of the blood in the atria fills the ventricles by gravity:
(a) The remaining 20% to 30% comes from atrial contraction.
iv. The AV junction (including the AV node, surrounding tissue, and the bundle of His [also called the AV bundle]) conducts impulses from the AV junction to the right and left bundle branches.
c. Normally, impulses pass through the AV junction into the bundle of His and then move rapidly into the right and left bundle branches on both sides of the interventricular septum.
i. If the atrial rate becomes very rapid, then the AV junction can regulate the number of impulses that reach the ventricle.
ii. They then spread into the Purkinje fibers.
iii. An electric impulse spreads across the ventricles in about 0.08 seconds while the ventricles simultaneously contract.
#46 Lecture Outline
3. Secondary pacemakers
a. Any conduction system component can act as a secondary pacemaker if the SA node becomes damaged or suppressed.
#47 Lecture Outline
4. Accessory conduction pathways
a. Extra heart muscle tissue that connects the atria and ventricles, bypassing the AV node.
i. James fibers
(a) In the atrial internodal pathways
(b) Extend into the ventricles while bypassing the AV node
ii. Mahaim fibers
(a) In the AV node, the bundle of His, and the bundle branches
(b) Extend into the ventricles and provide a common pathway for reentrant dysrhythmias
iii. Bundle of Kent
(a) Typically located between the LA and the LV, although it is sometimes found between the RA and the RV.
(b) It enables the depolarization wave to bypass the AV node and trigger early depolarization of a section of ventricular tissue.
(c) Simultaneously, depolarization travels through the AV node and bundle of His to the bundle branches.
(d) These simultaneous depolarization events create a change on the ECG tracing called a delta wave.
b. Can trigger tachydysrhythmias
#48 Lecture Outline
F. The autonomic nervous system and the heart
1. Effect on the heart by the sympathetic and parasympathetic divisions of the autonomic nervous system
#49 Lecture Outline
a. Sympathetic (accelerator) nerves supply specific areas of the heart’s electrical system, atrial muscle, and ventricular myocardium.
i. Nerves transmit commands by releasing norepinephrine.
ii. Norepinephrine travels to the SA node, AV node, and ventricles.
iii. To prevent a buildup of lactic acid, the heart speeds up, increasing CO.
b. An accelerated heart rate shortens all phases of the cardiac cycle.
i. When the ventricles have less time to relax, less time is available for these chambers to fill adequately with blood.
ii. CO decreases, and signs of myocardial ischemia may appear.
#50 Lecture Outline
c. Parasympathetic (inhibitory) nerve fibers supply the SA node, atrial muscle, and the AV junction of the heart by way of the vagus nerve.
i. The vagus nerve:
(a) Innervates functional areas
(b) Decreases the heart rate
(c) Stimulated in a number of ways, including:
(1) Increased pressure on the carotid sinus
(2) Strained or forced exhalation against a closed glottis (Valsalva maneuver)
(3) Distention of a hollow organ, such as the bladder or stomach
#51 Lecture Outline
d. If the brain senses that the heart should slow its pace:
i. An electrical impulse travels down the vagus nerve to the SA node.
ii. The electrical impulse stimulates the release of acetylcholine (ACh).
iii. ACh signals the SA node to decelerate the heart rate.
iv. Another ACh molecule travels to the AV node ensuring that no additional impulses get through.
#52 Lecture Outline
2. Baroreceptors and chemoreceptors
a. Baroreceptors: Sensors composed of specialized nerve tissue
i. Also known as pressoreceptors
ii. Found in the internal carotid arteries and aortic arch
iii. Detect changes in blood pressure
iv. Generate a reflex response in either the sympathetic or parasympathetic division of the ANS
#53 Lecture Outline
b. Chemoreceptors
i. Chemoreceptors located in the internal carotid arteries, aortic arch, and medulla detect changes in the concentrations in the blood.
(a) Hydrogen ions (pH)
(b) Oxygen
(c) Carbon dioxide
ii. Causes either a sympathetic or parasympathetic response to changes
#54 Lecture Outline
G. Causes of cardiac dysrhythmia
1. Evaluate the dysrhythmia in the context of the patient’s overall clinical condition.
a. Treat the patient, not the monitor!
#55 Lecture Outline
H. The electrocardiogram
1. A graphic record of the changes in voltage that occur in the heart muscle during depolarization and repolarization
2. Three standard limb leads (leads I, II, and II)
3. More detailed information from a 12-lead ECG
4. Lead wires are connected to electrodes to offer an electrical snapshot of a specific part of the heart.
#56 Lecture Outline
5. Electrode placement
a. The electrodes must be placed in a consistent, predetermined place to get a reliable reading.
b. Electrodes in the prehospital setting are usually adhesive with a gel center for better skin contact, although some have a diaphoretic electrode to better stick to a patient who is sweating.
#57 Lecture Outline
c. Basic principles for best skin contact and to minimize artifacts in the signal.
i. Shave the patient’s body hair at the electrode site.
ii. Rub the electrode site briskly with a dry gauze pad.
iii. Attach the electrodes to the ECG cables before placement, and confirm the correct location on the patient.
iv. Turn on the monitor and print a sample rhythm strip to check for interference.
d. To properly perform cardiac monitoring, refer to Skill Drill 18-1.
#58 Lecture Outline
6. The leads
a. Two main groups:
i. Limb leads (leads I, II, and III)
ii. Precordial leads (V1 to V6)
b. The augmented limb leads (aVR, aVL, aVF) contain only one true pole; the other is a combination of information from other leads.
#59 Lecture Outline
c. A standard 12-lead ECG comprises the three standard limb leads, the three augmented limb leads, and the six precordial leads.
d. A lead wire is an electrical cable that attaches an electrode to the ECG monitor.
i. An image of the heart taken from a specified vantage point
ii. Measures the electrical potential difference between two electrodes
e. Frontal plane leads (leads I, II, and III) view the heart from the front of the body.
f. The precordial leads (V1 to V6) are called unipolar chest leads, anterior leads, or V leads.
#60 Lecture Outline
g. Limb leads were initially discovered by Willem Einthoven.
i. Einthoven discovered that the heart emits electrical energy every time it contracts.
(a) Recorded three leads:
(1) Lead I
(2) Lead II
(3) Lead III
#61 Lecture Outline
(b) Leads I, II, and III are bipolar leads.
(1) Contain a positive and negative pole
(2) Measures the difference in electrical potential between electrodes placed on two extremities
#62 Lecture Outline
h. The augmented voltage (aV leads) are also created using the four limb electrodes.
i. Leads aVR, aVL, and aVF are created by combining two of the limb leads and using the other lead as the other pole.
(a) Example: The lead aVR is created between the right arm and the combination of the left arm and leg electrodes.
#63 Lecture Outline
i. If you are performing continuous cardiac monitoring, then place four electrodes on the patient’s torso.
i. White—right upper chest near the shoulder
ii. Black—left upper chest near the shoulder
iii. Red—left lower abdomen
iv. Green—right lower abdomen
#64 Lecture Outline
j. If you are acquiring a 12-lead ECG, then place the four electrodes on the patient’s limbs.
i. White—right wrist
ii. Black—left wrist
iii. Red—left ankle
iv. Green—right ankle
#65 Lecture Outline
k. Precordial leads view the heart in the horizontal plane.
i. The precordial leads V1 to V6 are unipolar.
ii. They are referenced against a calculated point known as Wilson central terminal.
iii. The Wilson central terminal is created by bisecting the limb leads in Einthoven’s triangle.
#66 Lecture Outline
l. The electrode for each unipolar lead is the positive terminal for that lead.
i. Leads V1 and V2 view the septum.
ii. Leads V3 and V4 look at the anterior wall of the left ventricle.
iii. Leads V5 and V6 view the lateral wall of the left ventricle.
iv. It is critical that these leads are placed consistently:
(a) V1—right of the sternum, fourth ICS
(b) V2—left of the sternum, fourth ICS
(c) V3—directly between leads V2 and V4
(d) V4—left midclavicular line, fifth ICS
(e) V5—left anterior axillary line at level of lead V4
(f) V6—left midaxillary line at level of lead V4
#67 Lecture Outline
m. Contiguous leads: leads that view geographically similar areas of the myocardium.
i. Leads II, III, and aVF are contiguous.
ii. Leads V1 and V2, V2 and V3, V3 and V4, V4 and V5 , and V5 and V6 are pairs of contiguous leads.
iii. Leads I and aVL, and aVL and V5 are also contiguous pairs.
n. In cases where a right-sided ECG is needed to evaluate the electrical activity of the right ventricle, the precordial leads are placed on the right anterior thorax.
i. V1R—left of the sternum, fourth ICS
ii. V2R—right of the sternum, fourth ICS
iii. V3R—directly between V2R and V4R
iv. V4R—right midclavicular line, fifth ICS
v. V5R—right anterior axillary line at level of lead V4R
vi. V6R—right midaxillary line at level of lead V4R
vii. Lead V4R is the most sensitive and specific for right ventricular AMI.
#68 Lecture Outline
o. Posterior leads are used to evaluate left ventricle posterior wall electrical activity.
i. Three precordial leads are placed on the left posterior thorax:
(a) V7—between V6 and V8, fifth ICS
(b) V7—midscapular, fifth ICS
(c) V7—just to the left of the spine, fifth ICS
#69 Lecture Outline
p. Use 15- and 18-lead ECGs as follows:
i. The 15-lead ECG uses the standard 12-lead ECG plus leads V4R, V7, and V8.
(a) A standard 12-lead ECG is recorded, followed by a second tracing containing the additional leads.
ii. The 18-lead ECG uses the 12-lead tracing plus leads V4R through V6R and V7 through V9.
#70 Lecture Outline
7. ECG concepts
a. The ECG baseline is generally a flat, straight, horizontal line that reflects a period of electrical silence in the myocardium.
i. Also referred to as the isoelectric line, TP segment, and isomeric line
b. An electrical impulse moving in the direction of a negative electrode produces a deflection below the baseline.
c. An electrical impulse moving toward a positive electrode produces a deflection above the baseline.
#71 Lecture Outline
d. Perpendicular movement of an impulse toward a positive electrode produces either of the following:
i. A perfectly flat line
ii. A waveform with both a positive and a negative component (biphasic waves)
#72 Lecture Outline
8. ECG paper
a. Graph paper moving past a stylus at a constant speed (25 mm/s)
i. One 1-mm box equals 0.04 second (1/25 of a second or 40 milliseconds) while one large box (consisting of five small boxes) equals 0.20 second (200 milliseconds).
ii. The vertical axis represents the amplitude (gain of deflection in millivolts).
iii. The standard amplitude calibration is 10 millimeters per millivolt.
#73 Lecture Outline
iv. A calibration box printed at the beginning of all 12-lead ECGs informs the paramedic about paper speed and amplitude and measures 5-mm wide and 10-mm tall.
#74 Lecture Outline
9. ECG components
a. The electrical conduction events in the heart can be recorded on an ECG as a series of:
i. Waves
ii. Segments
iii. Intervals
iv. Complexes
b. A P wave represents atrial depolarization.
i. Characterized by a smooth, round, upright shape
ii. Normal duration of less than 0.11 seconds (110 ms)
iii. Amplitude less than 2.5 mm tall
#75 Lecture Outline
c. PR interval (PRI) is the distance from the beginning of the P wave to the beginning of the QRS complex.
i. Represents the time required for an impulse to traverse the atria and AV junction, normally 0.12 to 0.20 seconds (120 to 200 ms).
ii. The PR segment represents the amount of time the AV node delays transmission of atrial activity to the ventricles.
#77 Lecture Outline
d. The QRS complex consists of three waveforms and represents ventricular depolarization.
i. Measured from the beginning of the Q wave to the end of the S wave and should follow each P wave consistently.
ii. It is narrow in healthy people, with a duration of less than 0.11 second.
iii. It indicates that conduction has proceeded normally.
iv. If impulse conduction is abnormal, then the complex has a bizarre appearance and a duration of 0.12 second or longer.
v. The first negative deflection is the Q wave, which represents conduction through the interventricular septum.
(a) Should not last more than 0.04 second
(b) Should be less than one-third the height of the QRS complex
(c) Considered abnormal or pathologic if it meets abnormal criteria—could indicate an AMI
vi. The first upward deflection is the R wave.
vii. The S wave is any downward deflection after the R wave.
viii. A second upward deflection is called an R-prime (Rʹ) wave.
ix. The R and S waves represent depolarization of the right and left ventricles.
#78 Lecture Outline
e. The J point is the point on the ECG where the QRS complex ends and the ST segment begins.
i. Represents the end of depolarization and the apparent beginning of repolarization
ii. Often depressed or elevated with an ischemic myocardium
f. The ST segment begins at the J point and ends at the T wave and represents early ventricular repolarization.
i. An elevated ST segment may indicate myocardial injury.
ii. A depressed ST segment may indicate myocardial ischemia.
#79 Lecture Outline
g. The T wave represents ventricular repolarization; should be asymmetric, less than half the overall height of the QRS complex, and oriented in the same direction as the overall QRS complex.
i. Very large (hyperacute) T waves may indicate myocardial ischemia, injury, and infarction.
ii. Tall, pointed (peaked) T waves may be seen with hyperkalemia.
iii. Deeply inverted T waves may be seen with acute CNS events.
#80 Lecture Outline
h. The U wave most likely represents the final stage of ventricular repolarization.
i. A U wave taller than 2 mm is considered abnormal and may be a sign of hypokalemia or cardiomyopathy.
i. The QT interval represents all the electrical activity of one completed ventricular cycle.
i. Begins with the onset of the Q wave and ends with the T wave
ii. Varies with age, sex, and heart rate
iii. Generally measures between 0.40 and 0.44 second
iv. A long QT interval can lead to ventricular dysrhythmias and sudden cardiac arrest.
#81 Lecture Outline
j. The TP segment is generally a flat, straight, horizontal line beginning at the end of the T wave and ending at the start of the P wave.
i. The baseline is the reference part to compare with the J point.
k. The R-R interval represents the interval between two ventricular depolarizations.
i. Can be used to calculate heart rate and determine regularity of the patient’s cardiac rhythm
#82 Lecture Outline
I. Approach to dysrhythmia interpretation
1. Method for interpreting ECG strips and being alert for dysrhythmia:
a. Identify the waves (P-QRS-T).
b. Measure the PRI.
c. Measure the QRS duration.
d. Determine rhythm regularity.
e. Measure the heart rate.
2. Notation of whether P waves are upright and fall within normal parameters
#83 Lecture Outline
3. Rhythm regularity
a. Determining rhythm regularity can be done by simply measuring the distance between R waves.
i. Regular—if the distance between R waves is exactly the same
#84 Lecture Outline
ii. Irregularly irregular—if no two R waves are equidistant
#85 Lecture Outline
iii. Regularly irregular—if the R waves are irregular but appear to follow a pattern
#86 Lecture Outline
4. Determining heart rate
a. The 6-second method—the fastest method for measuring heart rate from the ECG
i. This can be used on regular and irregular rhythms.
ii. Count the number of QRS complexes in a 6-second strip, and then multiply by 10 to obtain the rate per minute.
#87 Lecture Outline
b. The sequence method—reserved for regular rhythms
i. Memorize the following: 300, 150, 100, 75, 60, 50.
ii. Find an R wave on a heavy line and count off the above sequence for each large box you land on until you reach the next R wave.
iii. If the R-R interval spans fewer than three large boxes, the rate is greater than 100 (tachycardia); if it is more than five large boxes, the rate is less than 60 (bradycardia).
#88 Lecture Outline
c. The 1,500 method—the most accurate, typically used for heart rates in excess of 150 beats/min, and can only be used on regular rhythms
i. Count the number of small boxes between any two QRS complexes, and then divide by 1,500.
ii. Yields a rate of approximately 65 beats/min
#89 Lecture Outline
J. Specific cardiac dysrhythmias
1. Cardiac dysrhythmias can be induced by many events.
a. Many can be traced to ischemia, especially the cardiac conduction system.
b. Dysrhythmias are the most common cause of cardiac arrest.
2. Dysrhythmias are classified in numerous ways.
a. Disturbances of automaticity or disturbances of conduction
b. Tachydysrhythmias or bradydysrhythmias
c. Life threatening or non–life threatening
d. By the site from which they arise
#90 Lecture Outline
3. Some rhythms originate in the SA node.
a. Normal sinus rhythm
i. Intrinsic rate of 60 to 100 beats/min and with regular rhythm and minimal variations between R-R intervals
ii. Upright P wave that precedes each QRS complex
(a) PRI: 0.12 to 0.20 seconds (120 to 200 ms)
(b) QRS complex: 0.11 seconds (110 ms) or less
#91 Lecture Outline
b. Sinus bradycardia
i. Rate of less than 60 beats/min.
ii. An upright P wave precedes every QRS complex.
(a) PRI: 0.12 to 0.20 seconds (120 to 200 ms)
(b) QRS complex: 0.11 seconds (110 ms) or less
iii. Very slow heart rates lead to inadequate CO and precipitate heart electrical instability.
iv. Ectopic pacemakers in the AV junction or ventricles may fire and produce escape beats when the sinus rate becomes very slow.
v. An impulse or rhythm originating from a site other than the SA node is referred to as ectopic.
vi. In healthy adults and conditioned athletes, sinus bradycardia may be asymptomatic and may occur during sleep.
vii. May cause:
(a) Altered mental status
(b) Ischemic chest discomfort
(c) Acute heart failure
(d) Seizures
(e) Syncope
(f) Hypotension
viii. Treatment is indicated when these signs and symptoms persist despite adequate airway and breathing.
c. Management of symptomatic bradycardia
i. Goals for emergency care
(a) Maintain adequate oxygenation, ventilation, and perfusion.
(b) Correct the rhythm disturbance and restore a stable perfusing rhythm.
(c) Search for the underlying cause, which may be hypoxia, hypothermia, shock, ACS, AV block, toxin exposure (beta-blockers, calcium channel blockers, organophosphates, digoxin), an electrolyte disorder, increased intracranial pressure, or other factors.
#92 Lecture Outline
ii. Administering emergency medical care
(a) Maintain an open airway, assist breathing as necessary, and administer supplemental oxygen as needed to maintain an Spo2 of 95% to 98%.
(b) Apply a cardiac monitor, BP monitor, and pulse oximeter; and obtain a 12-lead ECG.
(c) Establish an IV infusion of normal saline, obtain a finger-stick blood glucose level, and treat hypoglycemia if present.
(d) Administer atropine IV bolus for symptomatic sinus bradycardia or a conduction block at the level of the AV node and repeat atropine every 3 to 5 minutes until the desired heart rate is achieved or until the dosage limit of 3 mg has been reached.
#93 Lecture Outline
(e) If atropine is ineffective and the patient’s symptoms or hemodynamic instability persist, then consider TCP or the administration of a dopamine or epinephrine infusion.
(f) Transport the patient for definitive care.
#94 Lecture Outline
d. Artificial pacemakers deliver repetitive bursts of electrical impulses to the heart.
i. Transcutaneous pacemakers (TCPs)
(a) Depolarize the myocardium by delivering electrical energy through the skin of the chest.
(b) “Capture” is usually associated with ventricular depolarization.
(1) Characterized by a wide QRS complex on the ECG and should result in a corresponding pulse.
#95 Lecture Outline
ii. Use a TCP in the following situations:
(a) A patient with a bradydysrhythmia that severely reduces CO and does not respond to atropine
(b) A patient who requires interhospital transfer for pacemaker implantation
(c) A symptomatic patient with artificial pacemaker failure
iii. To properly initiate TCP, refer to Skill Drill 18-2.
#96 Lecture Outline
e. Sinus tachycardia
i. The rate is 101 to 180 beats/min, with regular rhythm.
ii. Upright P wave precedes every QRS complex.
(a) PRI: 0.12 to 0.20 second (120 to 200 ms)
(b) QRS complex: 0.11 second (110 ms) or less
iii. May result from:
(a) Pain
(b) Fever
(c) Hypoxia
(d) Hypovolemia
(e) Exercise
(f) Stimulation of the sympathetic nervous system
(g) AMI
(h) Pump failure
(i) Anemia
(j) Certain drugs, caffeine, nicotine, and alcohol
#97 Lecture Outline
iv. Hypoxia, metabolic alkalosis, hypokalemia, and hypocalcemia can lead to electrical instability, prompting the firing of cells that normally do not generate impulses.
v. Prolonged tachycardia increases the work of the heart, causing further ischemia during an AMI.
(a) CO may be significantly reduced if the heart rate exceeds 150 beats/min.
vi. Treatment is related to the underlying cause.
#98 Lecture Outline
f. Sinus dysrhythmia
i. A slight variation in cycling of a sinus rhythm usually exceeding 0.12 second (120 ms) between the longest and shortest cycles associated with respiratory cycle fluctuations
ii. The rate increases during inspiration and decreases during expiration.
iii. An upright P wave precedes every QRS complex.
(a) PRI: 0.12 to 0.20 second (120 to 200 ms)
(b) QRS complex: 0.11 second (110 ms) or less
iv. Often found in children and young adults and tends to diminish with age
#99 Lecture Outline
g. Sinus arrest
i. The SA node fails to initiate an impulse, which eliminates the P wave, QRS complex, and/or T wave for one cardiac cycle, then resumes normal functioning.
ii. The atrial and ventricular rates are usually within normal limits, with regular rhythm, except for the absent complexes.
iii. Upright P waves precede every QRS complex.
(a) PRI (when present): 0.12 to 0.20 second (120 to 200 ms)
(b) QRS complex (when present): 0.11 second (110 ms) or less
#100 Lecture Outline
iv. Possible causes include:
(a) Ischemia of the SA node
(b) Increased vagal tone
(c) Carotid sinus massage
(d) Use of drugs such as digitalis and quinidine
v. Occasional episodes are not significant unless the heart rate drops below 60 beats/min.
vi. Treatment may include a temporary pacemaker in the field or a permanent pacemaker placed in the hospital.
#101 Lecture Outline
h. Sick sinus syndrome
i. A variety of rhythms involving a poorly functioning SA node common in older adults
ii. Patients may exhibit syncope, dizziness, and palpitations or may have no symptoms.
iii. It shows on an ECG as:
(a) Sinus bradycardia
(b) Sinus arrest
(c) SA block
(d) Alternating patterns of extreme bradycardia and tachycardia
#102 Lecture Outline
K. Rhythms originating in the atria
1. Impulses from any area in the atria
2. Upright P waves preceding each QRS complex
a. They are not as well rounded as those generated from the SA node.
#103 Lecture Outline
3. Premature atrial complex (PAC)
a. An ectopic complex within another rhythm
i. An upright P wave precedes each QRS complex, but its shape differs from P waves originating from the SA node.
(a) PRI: 0.12 to 0.20 second (120 to 200 ms) but may vary slightly
(b) QRS complex: 0.11 second (110 ms)
ii. Not always conducted to the ventricles
(a) A nonconducted PAC is the presence of a P wave that occurs early on the ECG and is not followed by a QRS complex.
iii. Very common and can be caused by stress, stimulants (eg, caffeine), or from conditions (eg, heart failure or electrolyte imbalance)
iv. Treatment is focused on correcting the underlying cause.
#104 Lecture Outline
4. Supraventricular tachycardia (SVT)
a. Originates from a site above the ventricles
i. Ventricular rate faster than 100 beats/min at rest
ii. In patients with normal ventricular function, tachycardia with a rate of less than 150 beats/min rarely causes serious signs and symptoms.
iii. The ventricular filling time is greatly lowered when the ventricular rate exceeds 150 beats/min, which greatly reduces CO.
iv. When the ventricular rate reaches 150 to 180 beats/min, the P waves (if present) with SVT tend to be completely obscured by the T wave of the preceding beat.
(a) PRI: cannot be measured until heart rate is lowered
(b) QRS complex: 0.11 second (110 ms) or less
#105 Lecture Outline
b. The most common is called AV nodal reentrant tachycardia.
i. Under conditions like the presence of myocardial ischemia, a premature impulse can trigger a series of rapid beats.
ii. These impulses could get stuck in a repetitive pattern, generating multiple ectopic beats or a very rapid rhythm.
#106 Lecture Outline
c. Cannon “A” waves are created by a dissociation between the atria and ventricles.
i. Larger waves can indicate deteriorating functionality of the right ventricle or increasing right ventricular end-diastolic pressure.
d. Treatment depends on the severity of the patient’s symptoms and may include medication or electrical therapy to slow the heart rate.
#107 Lecture Outline
e. Note the following for management of tachycardia with a pulse.
i. Goals for emergency medical care include:
(a) Identify and treat patients with signs or symptoms of hemodynamic instability or those who are symptomatic because of the dysrhythmia.
(b) Maintain adequate oxygenation, ventilation, and perfusion.
(c) Correct the rhythm disturbance and restore a sinus rhythm.
(d) Search for the underlying causes, such as medications (caffeine, diet pills, thyroid agents, or decongestants), illicit drugs (cocaine, amphetamines), heart failure, or a history of dysrhythmia.
ii. Before starting treatment, make the following judgements:
(a) Determine the severity of the patient’s signs or symptoms.
(b) Determine whether the QRS complex is narrow or wide.
(c) Determine whether the ventricular rhythm is regular or irregular and obtain a 12-lead ECG if time permits.
#108 Lecture Outline
iii. If the patient is stable and exhibiting signs related to tachycardia, therapies such as vagal maneuvers and medications are recommended.
iv. If unstable signs and symptoms are determined to result from tachycardia, use of electrical therapy with synchronized cardioversion is recommended.
#109 Lecture Outline
v. Follow the procedure to provide emergency care for an adult who has tachycardia with a pulse:
(a) Maintain an open airway and an Spo2 between 95% and 98% by assisting in breathing and administering supplemental oxygen.
(b) Apply a cardiac monitor, BP monitor, and pulse oximeter; obtain a 12-lead ECG, but do not delay emergency care.
(c) Establish an IV infusion of normal saline and obtain a finger-stick blood glucose measurement.
#110 Lecture Outline
(d) If the QRS is narrow and regular, the patient is stable, and there are no contraindications, then perform vagal maneuvers.
(e) If the QRS is narrow and regular and the patient is unstable, consider sedation before performing synchronized cardioversion.
(f) Transport the patient for definitive care.
#111 Lecture Outline
vi. Vagal maneuvers are attempted for stable patients with regular narrow-QRS tachycardia before starting medication therapy.
(a) Stimulate baroreceptors, which signal brainstem centers to stimulate the vagus nerve and slow the heart rate
(b) Many types exist.
(1) Carotid sinus massage: Assess for bruits before performing this procedure.
(2) The Valsalva maneuver: The patient bears down as if attempting a bowel movement.
#112 Lecture Outline
vii. Administer adenosine if vagal maneuvers are ineffective and the patient with a narrow-QRS tachycardia remains stable.
(a) Administer at the IV site closest to the patient’s heart.
(b) Follow with a 20-mL flush of normal saline solution.
(c) Be prepared for a short run of asystole.
#113 Lecture Outline
(d) If the first dose of adenosine is unsuccessful, then administer a double dose of adenosine and administer it again in 1 to 2 minutes.
(e) If needed, repeat the dose again in 1 to 2 minutes.
(f) If adenosine does not convert the rhythm, rapidly transport the patient to the medical facility.
#114 Lecture Outline
viii. If at any time the condition of a patient with SVT becomes unstable, you should move to the unstable arm of the tachycardia algorithm.
ix. Synchronized cardioversion is the use of a defibrillator to terminate a hemodynamically unstable tachydysrhythmia.
#115 Lecture Outline
x. Cardioversion is indicated for VT and SVT associated with severely compromised CO.
(a) Sedate the patient first if performing cardioversion on a responsive patient.
(b) Benzodiazepines are commonly administered for sedation.
(c) To properly perform cardioversion, refer to Skill Drill 18-3.
#116 Lecture Outline
5. Preexcitation
a. Refers to early depolarization of ventricular tissue by means of an accessory pathway between the atria and ventricles.
b. The most common preexcitation disorder is Wolff-Parkinson-White syndrome (WPW).
i. Characterized by:
(a) A short PRI (less than 0.12 second [120 milliseconds])
(b) Nonspecific ST-T wave changes
(c) A widened QRS complex
(d) The appearance of a delta wave on ECG
c. Lown-Ganong-Levine syndrome also causes preexcitation of ventricular tissue.
i. Characterized by:
(a) A short PRI
(b) A normal QRS duration
d. Patients with WPW and Lown-Ganong-Levine syndrome are susceptible to tachydysrhythmias.
#117 Lecture Outline
e. Care of a patient with either of these syndromes includes:
i. Seeking the advice of a physician
ii. Basing treatment on the gravity of the patient’s instability, QRS complex width, and the ventricular rhythm regularity
iii. Ensuring medication that slows or blocks conduction through the AV node is not administered
#118 Lecture Outline
6. Atrial fibrillation (AF)
a. The atria no longer contract but instead fibrillate or quiver, with no organized contraction.
b. Cells in the atria depolarize independently, rather than in response to an SA node impulse.
c. Results in a fibrillating or chaotic baseline.
d. Characterized by:
i. No visible P wave on the ECG strip
ii. No PRI to measure
iii. Irregularly irregular appearance
iv. QRS complex: 0.11 second (110 ms) or less
e. Common rhythm among older adult patients
f. Increases the risk of stroke because blood within the fibrillating atria tends to clot
g. Stable but symptomatic patients may be prescribed:
i. Anticoagulant medications (eg, warfarin [Coumadin])
ii. Beta-blockers, calcium channel blockers, or digoxin
h. Unstable patients may need synchronized cardioversion.
#119 Lecture Outline
7. Atrial flutter
a. Atrial impulses fire at a rate too fast for the ventricles to keep up.
b. Atrial complexes are known as flutter waves or F waves, with a distinctive sawtooth shape resembling a picket fence.
c. One or more of the F waves gets blocked by the AV node, resulting in several F waves before each QRS complex.
d. Usually regular with constant (usually 2:1) conduction, or irregular, with the QRS complex measuring 0.11 second (110 ms) or less
#120 Lecture Outline
e. Can degenerate into AF
f. Patients are often prescribed anticoagulant medications because these patients are thought to have the same risk of thromboembolism as patients with AF.
g. A beta-blocker or calcium channel blocker may be administered if the patient is stable but symptomatic.
h. Synchronized cardioversion may be necessary if the patient is unstable.
i. Prehospital treatment is uncommon in stable patients.
#121 Lecture Outline
8. Wandering atrial pacemaker
a. The pacemaker moves from the SA node to various areas within the atria or AV junction.
b. The rate is usually 60 to 100 beats/min, with a slightly irregular rhythm and R-R intervals based on the pacemaker site for that particular complex.
c. A P wave precedes each QRS complex; however, the P wave shapes vary, indicating multiple sites of origin.
d. The definition requires the presence of at least three different shapes of P waves within one ECG strip.
e. Characterized by:
i. PRI: 0.12 to 0.20 second (120 to 200 ms) (varies based on complex origin)
ii. The QRS complex: 0.11 second (110 ms) or less
#122 Lecture Outline
f. It is seen in children, older adults, and athletes.
g. Treatment is indicated in the prehospital setting only if the dysrhythmia is associated with a slow rate and the patient is symptomatic.
i. Treatment would be the same as for symptomatic sinus bradycardia.
#123 Lecture Outline
9. Multifocal atrial tachycardia (MAT)
a. Multiple ectopic sites within the atria depolarize at different but rapid rates.
b. Characterized by a rate of more than 100 beats/min
c. A tachycardic wandering atrial pacemaker, with an irregular rhythm and R-R intervals that vary based on the site of the pacemaker
d. There is a P wave preceding each QRS complex, but the shape varies, indicating multiple sites of origin.
#124 Lecture Outline
e. Characterized by:
i. PRI of 0.12 to 0.20 second (120 to 200 ms) (varies slightly)
ii. QRS measuring 0.11 second (110 ms) or less and P waves may not be visible if the MAT increases to more than 150 beats/min
f. Most often seen in patients with:
i. Significant lung disease
ii. Pulmonary hypertension
iii. Coronary disease
iv. Valvular heart disease
v. Hypomagnesemia
g. Also seen in patients undergoing theophylline therapy
h. Treatment is not usually at the prehospital level, and therapies for SVT are generally ineffective with MAT.
#125 Lecture Outline
L. Rhythms originating at the AV junction
1. The AV junction should take over if the SA node fails to initiate an impulse.
2. Junctional rhythms normally have a rate of 40 to 60 beats/min.
3. An impulse generated in the AV junction travels down into the ventricles and up toward the SA node.
#126 Lecture Outline
4. This leads to three possible circumstances, in which the QRS complex appears normal.
a. If the impulse begins moving upward through the atria before the other part enters the ventricles, an inverted P wave will show, followed immediately by the QRS complex.
b. If the impulse moving through the atria occurs at the exact time it travels through the ventricles, the smaller inverted P wave will be hidden within the QRS complex, giving the appearance of a missing P wave until a normal QRS complex begins.
c. If the impulse starts late through the atria, it will result in an inverted P wave after the QRS complex.
#127 Lecture Outline
5. A premature junctional complex is an early complex that appears within another rhythm.
a. The rate depends on the underlying rhythm and is irregular.
b. The P wave, if present, will be inverted and may either precede or follow the QRS complex.
c. Characterized by:
i. PRI, if present: less than 0.12 second (120 ms)
ii. The QRS complex: measures 0.11 second (110 ms) or less
d. Can be caused by many of the same factors that cause PACs
e. Do not normally require treatment, since most people with the condition are asymptomatic
#128 Lecture Outline
f. Possible symptoms:
i. Perceived skipped beats
ii. Light-headedness
iii. Dizziness
iv. Other signs of decreased CO with frequent PJCs
g. Frequent PJCs may be a predictor of future cardiac dysrhythmias.
#129 Lecture Outline
6. Junctional escape rhythm occurs when the SA node does not function and the AV junction takes over as the pacemaker.
a. Also called a junctional rhythm
i. Rate of 40 to 60 beats/min; usually regular rhythm with little variation between R-R intervals
ii. The P wave inverted and present before the QRS
iii. PRI: less than 0.12 second (120 ms)
iv. QRS complex: 0.11 second (110 ms) or less
b. Often accompanies:
i. SA node disease
ii. Increased vagal tone
iii. Valvular heart disease
iv. Inferior wall MI
v. Other cardiac conditions
c. It can occur after resuscitation from cardiac arrest.
d. Treatment depends on underlying cause but may require a surgically implanted pacemaker.
e. In the field, atropine should be considered, and TCP may be necessary if the patient’s condition is severely compromised.
#130 Lecture Outline
7. Accelerated junctional rhythm is present with a rate exceeding 60 beats/min but less than 100 beats/min.
a. Regular with little variation between R-R intervals, and the P wave, if present, is inverted before or after the QRS complex
b. Characterized by:
i. PRI: less than 0.12 second (120 ms)
ii. The QRS complex: measures 0.11 second (110 ms) or less
c. May be associated with:
i. Digoxin toxicity (most common cause)
ii. Hypoxia
iii. Inferior wall MI
iv. Rheumatic fever
v. Recent cardiac surgery
vi. Electrolyte imbalance
d. The patient usually is asymptomatic.
#131 Lecture Outline
8. Junctional tachycardia is accompanied by a rate that exceeds 100 beats/min.
a. ECG characteristics are the same as an accelerated junctional rhythm, but the rate is faster than 100 beats/min.
b. It is uncommon in adults but is associated with acute coronary syndrome, heart failure, theophylline administration, or digoxin toxicity.
c. Seldom requires treatment in the prehospital setting; if the rate exceeds 150 beats/min, CO could suffer.
d. At a rapid ventricular rate, distinguishing junctional tachycardia from other narrow-QRS tachycardias is often difficult.
e. If the patient is symptomatic, then treat in accordance with the tachycardia algorithm.
#132 Lecture Outline
M. Rhythms originating in the ventricles
1. The ventricles may start originating their own impulses and become the pacemaker if the AV junction does not take over after the SA node does not initiate an impulse.
a. Will have wide QRS complexes (0.12 second [120 ms] or more) and missing P waves
#133 Lecture Outline
2. Premature ventricular complex (PVC)
a. Not a dysrhythmia, but rather an early complex that appears within another rhythm
b. It is characterized by lack of P wave and no PRI.
c. The QRS complex associated with the PVC measures 0.12 second (120 ms) or more
d. The T wave is usually opposite in the direction of the QRS.
e. A full compensatory pause usually follows a PVC; to determine if one is present:
i. Measure an R-R interval of the underlying rhythm.
ii. Next, measure from the R wave of the QRS complex before the PVC to the R wave of the QRS complex after the PVC.
iii. A full compensatory pause has occurred if the R-R interval that includes the PVC measures twice that of the underlying rhythm.
#134 Lecture Outline
f. A PVC may be unifocal or multifocal.
i. Unifocal: originate from the same area or focus within the ventricle and look alike on the ECG
#135 Lecture Outline
ii. Multifocal: varied appearance; more than one focus initiating the ventricular impulses
#136 Lecture Outline
g. A ventricular couplet is two PVCs with no intervening pause.
h. A “run” of VT is the term for three or more PVCs in a row; also referred to as salvos or bursts.
#137 Lecture Outline
i. Ventricular bigeminy is the pattern that occurs when the complexes become so frequent that they begin to alternate with normal complexes, generating a normal–PVC–normal–PVC pattern.
j. Ventricular trigeminy is the pattern of every third beat being a PVC (normal–normal–PVC).
#138 Lecture Outline
k. Most often originate from ischemia in the ventricular tissue
l. Generally considered more serious than premature atrial or junctional complexes.
m. A principal hazard of PVCs is that the R wave of the PVC may occur during the T wave of the preceding complex.
i. This so-called R-on-T phenomenon can lead to ventricular fibrillation.
n. Occasional PVCs are common and usually don’t require treatment in otherwise healthy patients.
o. PVCs that occur in patients with heart disease require close monitoring and search for underlying cause.
#139 Lecture Outline
3. Idioventricular rhythm (IVR)
a. Occurs when the SA and AV nodes fail and the ventricles must pace the heart
b. Usually regular, with little variation between R-R intervals
c. No P wave, so no PRI
d. Rate of 20 to 40 beats/min; usually regular, with little variation between R-R intervals
e. QRS complex: more than 0.12 second (120 ms)
f. Agonal rhythm: pattern created when the ventricular rate slows to less than 20 beats/min
g. May or may not result in a palpable pulse
h. Treatment: improving the CO by increasing the rate and, if possible, treating the underlying cause
i. If pulse, then treat the rhythm in accordance with the bradycardia algorithm
ii. If no pulse, then the patient is in cardiac arrest
#140 Lecture Outline
4. Accelerated IVR
a. This rhythm occurs when an idioventricular rhythm exceeds 40 beats/min but remains less than 100 beats/min.
b. The rhythm is regular, with little variation between R-R intervals.
c. P waves are absent, so there is no PR interval.
d. The QRS complex is 0.12 second (120 ms) or more.
e. May be observed in patients with AMI, after reperfusion therapy, or during resuscitation efforts.
f. It rarely requires intervention because the rate is well tolerated.
#141 Lecture Outline
5. Ventricular tachycardia (VT)
a. Three or more sequential ventricular beats at a rate exceeding 100 beats/min
b. The rhythm is regular, with only a slight variation between R-R intervals.
c. P waves are absent, so the PRI does not exist.
d. The QRS complex is 0.12 second (120 ms) or more; this is considered a wide-QRS tachycardia.
e. QRS complexes usually have uniform tops and bottoms (monomorphic).
#142 Lecture Outline
f. Occasionally, the QRS complex will vary in height and width in an alternating pattern (polymorphic VT).
i. The most common is torsades de pointes.
ii. A prolonged QT interval may be congenital or acquired.
g. If the patient is stable, emergency care should focus on treatment with antidysrhythmic medications.
h. If the patient is unstable and the cardiac monitor shows monomorphic VT, electrical therapy using synchronized cardioversion may be necessary.
i. If the patient is unstable and the monitor shows polymorphic VT, defibrillation should be performed.
j. If the cardiac monitor shows VT but there is no pulse, then the patient is in cardiac arrest.
#143 Lecture Outline
6. Ventricular fibrillation (VF)
a. Rhythm in which the entire heart is fibrillating without a discernable pattern
b. Occurs when many different cells become depolarized independently rather than from an SA node impulse
#144 Lecture Outline
c. No P waves, PR interval, or QRS complexes
i. When fibrillatory waves are greater than 3 mm in amplitude, the dysrhythmia is called coarse VF.
ii. When the fibrillatory waves are less than 3 mm in amplitude, the dysrhythmia is called fine VF.
#145 Lecture Outline
d. Defibrillation
i. Effective for:
(a) VF
(b) Pulseless VT
ii. Delivers a current that is powerful enough to depolarize all of the heart’s component muscle cells
(a) Automated external defibrillator (AED)
(b) Manual defibrillator
#146 Lecture Outline
(c) Regardless of the type, high-quality CPR must be ongoing while the defibrillator is readied for use.
(d) Adhesive pads are placed on the chest wall to maximize the flow of current through the heart.
(e) AEDs and manual defibrillators deliver energy in waveforms.
(1) Monophasic waveforms deliver energy through the heart from one defibrillation pad to the other in a single direction.
(2) With biphasic waveforms, energy travels through the heart from one defibrillation pad to the other and then reverses direction, flowing back through the heart from one pad to the other.
#147 Lecture Outline
iii. Safety measures for performing manual defibrillation:
(a) Ensure no one is touching the patient.
(b) Do not defibrillate a patient who is lying in pooled water.
(c) Do not defibrillate someone who is touching metal that others are touching.
(d) To prevent burns, avoid placing a defibrillation pad over a medication patch or any metal objects such as jewelry.
(e) If the patient has an implanted pacemaker or internal defibrillator, place the defibrillation pad below the device/battery, or place the pads in anterior and posterior positions.
#148 Lecture Outline
iv. The defibrillator should be inspected at the beginning of each shift to check for the following gear:
(a) Defibrillation pads
(b) Cables and connectors
(c) Power supply
(d) Monitor
(e) ECG recorder
(f) Any ancillary supplies (extra pads and spare batteries)
v. To properly perform manual defibrillation, refer to Skill Drill 18-4.
#149 Lecture Outline
vi. An AED in manual mode allows for the use of all electrical therapy functions, as well as multiple-lead cardiac monitoring and 12-lead ECG acquisition.
vii. If an AED is not in use, but the patient goes into cardiac arrest, select manual mode on the defibrillator unit.
(a) It is essential to minimize the interruption of chest compressions.
viii. A fully automated AED can assess the patient’s rhythm and, if VF or VT is present, charge the pads and defibrillate, with no intervention by the rescuer.
(a) A semiautomated AED uses visual and verbal prompts to indicate when a shock is advised.
ix. To properly perform defibrillation with an AED, refer to Skill Drill 18-5.
x. Assess for a pulse, recognizing that one of the following outcomes is likely:
(a) The pulse is regained.
(b) The pulse is not regained, and the AED indicates that no shock is advised.
(c) The pulse is not regained, and the AED indicated that a shock is advised.
#150 Lecture Outline
xi. Wearable cardioverter-defibrillators
(a) Designed for patients at risk of sudden cardiac death, but who are not immediate candidates for therapy with an implantable cardioverter-defibrillator
(b) Example: LifeVest houses nonadhesive sensing electrodes and separate defibrillation electrodes; continuously reads and records the patient’s ECG; and up to five biphasic energy shocks can be delivered for a single event.
#151 Lecture Outline
7. Asystole (“flat line”)
a. The only true arrhythmia; the entire heart is no longer contracting and shows no evidence of organized activity.
b. Complete absence of ventricular electrical activity; P waves may be occasionally seen, but with no QRS complexes or T waves (called P-wave asystole, ventricular asystole, or ventricular standstill).
c. A flat line on an ECG monitor may or may not indicate asystole.
d. Asystole is considered a nonshockable cardiac arrest rhythm.
#152 Lecture Outline
8. Pulseless electrical activity (PEA)
a. An organized cardiac rhythm not accompanied by a detectable pulse
i. The mechanical ventricular activity is too weak to produce a palpable pulse, as in cases of:
(a) Cardiogenic or hypovolemic shock
(b) Cardiac tamponade
(c) Massive pulmonary embolism
(d) Electrolyte imbalance disturbances (including hyperkalemia in renal failure)
(e) Drug overdose
b. The key to treatment is identifying the cause.
c. PEA is a nonshockable cardiac arrest rhythm.
#153 Lecture Outline
N. Management of adult cardiac arrest
1. Most patients with cardiac arrest have evidence of prior heart disease.
a. Can also occur from electrocution, drowning, trauma, drug overdose, asthma, or anaphylaxis
b. Possibly no warning before the event
2. Cardiac arrest management requires an orderly, systematic approach that is rehearsed repeatedly in a team setting.
#154 Lecture Outline
3. Bring the following devices and equipment when you initially approach the scene:
a. Defibrillator
b. Portable oxygen cylinder
c. Airway management equipment, including an intubation kit
d. IV equipment
e. Drug box
#155 Lecture Outline
4. The goals of emergency medical care of a patient in cardiac arrest include the return of spontaneous circulation (ROSC) and the preservation of neurologic function.
a. Begin emergency medical care immediately upon discovering pulselessness.
#156 Lecture Outline
5. Withholding CPR is considered appropriate when:
a. Attempts to perform CPR would place rescuers at risk.
b. There are obvious clinical signs of irreversible death.
c. A valid advance directive, a physician order for life-sustaining treatment form indicating that resuscitation is not desired, or a valid do not attempt resuscitation order is presented to rescuers.
#157 Lecture Outline
6. Proceed with CPR as follows:
a. If bystanders have delivered uninterrupted chest compressions before arriving, or if the arrest is witnessed by EMS personnel
i. Proceed with rhythm analysis
b. If compressions have not been provided, or if the arrest was not witnessed by EMS personnel
i. Begin chest compressions while a second rescuer sets up the AED or defibrillator, and proceed with rhythm analysis.
#158 Lecture Outline
7. Components of high-quality adult CPR include the following:
a. Chest compressions at a rate of 100/min to 120/min
b. Compressions of the chest to a depth of at least 2 inches (5 cm) and less than 2.4 inches (6 cm)
c. Full chest recoil after each compression
d. Minimal interruption of compressions and a chest compression fraction of at least 60%
e. Adequate ventilation
f. Rotate the person delivering chest compressions every 2 minutes to minimize fatigue
#159 Lecture Outline
8. Four possible cardiac arrest rhythms:
a. Pulseless VT
b. Pulseless VF
c. Asystole
d. PEA
#160 Lecture Outline
9. Key points to remember:
a. If defibrillation is indicated, then the provider giving chest compressions should continue while a second rescuer charges the defibrillator.
i. Then pause CPR, clear the patient, and deliver the shock.
ii. Resume chest compressions immediately, without pausing for a rhythm or pulse check.
#161 Lecture Outline
b. After 2 minutes or five cycles of CPR, pause resuscitation efforts and check the rhythm on the monitor.
i. If a rhythm other than VF or VT appears, then identify the new rhythm and check for a pulse.
ii. If there is no pulse, then move down the algorithm to the asystole-PEA pathway and immediately resume CPR.
iii. If there is a pulse, then move to the appropriate algorithm for the new rhythm.
#162 Lecture Outline
c. Minimize rescuer fatigue by switching the CPR compressor and ventilator at the end of each 2-minute session of CPR.
d. To maximize the number of compressions delivered per minute, interruptions should not exceed 10 seconds.
#163 Lecture Outline
e. Using normal saline, attempt to establish vascular access.
i. If you are unable to establish IV access, then establish intraosseous (IO) access using an adult IO system.
ii. Vascular access should be achieved without interrupting chest compressions.
iii. As soon as IV or IO access has been established, administer epinephrine.
(a) Epinephrine 1 mg (1 mg/mL [1:10,000]) is administered IV or IO and is repeated every 3 to 5 minutes until a pulse returns.
iv. Whenever giving IV or IO medication during CPR, follow it immediately with a 20-mL flush of normal saline to facilitate delivery of the medication to the central circulation.
#164 Lecture Outline
f. Several options are available for airway management.
i. A nonrebreathing mask may be used for three to four cycles of uninterrupted chest compressions, after which bag-mask ventilation or an advanced airway is considered.
ii. A bag-mask device may be used throughout the resuscitation effort.
iii. For adults in cardiac arrest without an advanced airway, use a 30:2 compression to ventilation ratio.
#165 Lecture Outline
iv. Ventilate with just enough volume to produce visible chest rise, and deliver each breath over about 1 second.
v. If the decision is made to insert an advanced airway, then verify placement by multiple methods, including waveform capnography, and secure the tube.
vi. Deliver 1 breath every 6 seconds (10 breaths/min) without interrupting chest compressions.
#166 Lecture Outline
g. VF or pulseless VT that persists or recurs after one or more shocks is called refractory VF/VT.
i. An antidysrhythmic, such as amiodarone, may be considered.
ii. Lidocaine may be considered as an alternative to amiodarone for VF/VT.
#167 Lecture Outline
h. During the arrest, consider the Hs and Ts to identify possible reversible causes of the arrest and factors that may complicate the resuscitation effort.
i. If at any point there is an ROSC, then assess the patient’s vital signs, support the airway and breathing, as required, and give medications as indicated to manage cardiac dysrhythmias, and maintain the blood pressure.
#168 Lecture Outline
10. Transportation of patients depends on the EMS system and is dictated by local protocol.
a. A patient has the best chance of survival when resuscitated at the scene, unless the location is unsafe.
b. It is not safe to defibrillate a patient in a moving ambulance.
#169 Lecture Outline
11. Special circumstances in cardiac arrest
a. Cardiac arrests that require the paramedic to adjust treatments and procedures include those associated with:
i. Morbid obesity
ii. Anaphylaxis
iii. Opioids
iv. Acute asthma
v. Electrolyte disturbances
vi. Drowning
#170 Lecture Outline
12. Post–cardiac arrest care
a. Goals of optimizing cardiopulmonary function and vital organ perfusion
b. Begin by optimizing oxygenation and ventilation.
i. Achieve and maintain an Spo2 of 92% to 98%.
ii. Avoid hyperventilation.
iii. Obtain a 12-lead ECG as soon as possible to determine whether acute ST-segment elevation is present.
iv. Assess and maintain an SBP of at least 90 mm Hg and a mean arterial pressure of at least 65 mm Hg.
c. Marked hypotension must be corrected rapidly.
i. Administer a fluid bolus of 1 to 2 liters (L) normal saline or lactated Ringer solution.
ii. If the patient has marked hypotension and the transport time to the medical facility will be prolonged, then consider administering a vasopressor infusion.
iii. If the rhythm is bradycardic or tachycardic, then follow the bradycardia or tachycardia algorithm.
d. Perform a neurologic assessment and determine whether the patient can follow commands.
e. Closely monitor the post–cardiac patient.
#171 Lecture Outline
13. When to stop CPR
a. Decisions regarding ongoing resuscitative efforts are guided by the local protocol or direct communication with medical control.
b. When the patient does not respond to prehospital cardiac arrest treatment, it is acceptable to cease efforts because:
i. ALS providers are capable of performing an initial resuscitation equivalent to an in-hospital resuscitation attempt; there are no additional benefits to ED resuscitation.
ii. CPR performed during patient packaging and transport is much less effective than CPR administered at the scene.
iii. EMS providers risk physical injury while attempting to perform CPR in a moving ambulance while unrestrained.
iv. Continuing resuscitation in futile cases places other motorists and pedestrians at risk, increases the amount of time during which the EMS crew is unavailable for other calls, impedes ED care of other patients, and incurs unnecessary charges from the medical facility.
#172 Lecture Outline
c. The AHA has published criteria for BLS and ALS termination of resuscitation for adult out-of-hospital cardiac arrests.
d. In some jurisdictions, state legislation will be required to permit pronouncement of death at the scene by a paramedic.
e. Gaining permission to stop CPR in the field will involve delicate issues:
i. Expectations of the patient’s family
ii. Disposition of the body
iii. Pressure from bystanders
iv. Paramedics unaccustomed to telling family a patient is dead
#173 Lecture Outline
O. Atrioventricular (AV) blocks
1. The SA node initiates impulses, which proceed through the atria and ventricles, resulting in heart contractions.
a. Occasionally, impulses are delayed more than usual or are completely blocked, causing AV blocks.
#174 Lecture Outline
b. First-degree AV block
i. Occurs when each impulse is delayed slightly longer than normal, resulting in a constant PRI that exceeds 0.20 second (200 ms)
ii. Considered the least serious type of block, but is often the first indication of damage in the AV node
iii. Usually regular with minimal variations between R-R intervals
(a) Regularity depends on the underlying rhythm.
iv. An upright P wave precedes each QRS complex; varying size and shape
(a) PRI: 0.20 second (200 ms) or greater; constant in duration
(b) QRS complex: 0.11 second (110 ms) or less
v. Rarely treated in a prehospital setting unless associated with symptomatic bradycardia
#175 Lecture Outline
c. Second-degree AV block type I
i. This is also called Mobitz type I second-degree block or Wenckebach.
ii. Occurs when an interruption in impulse conduction occurs within the AV node, bundle of His, or His-Purkinje system.
(a) This prevents the impulse from proceeding to the ventricles and generating a QRS complex.
iii. The interval between P waves is regular, and an upright P wave precedes most QRS complexes.
iv. The ventricular rhythm is irregular, with a prolonged R-R interval between the last QRS complex before the blocked P wave and the QRS complex after the first unblocked P wave.
v. PRI starts out within normal limits of 0.12 to 0.20 second (120 to 200 ms) but grows longer with each P wave.
(a) Results in a P wave followed by another P wave instead of a QRS complex
(1) The P wave is then followed by a QRS complex with a normal PRI.
(2) The pattern repeats in the same rhythm.
(b) QRS complex: 0.11 second (110 ms) or less
vi. The keys to recognizing second-degree AV block type I:
(a) Observing there are more P waves than QRS complexes
(b) Noting the P waves occur at regular intervals
(c) Recognizing the PRIs associated with the conducted P waves get longer until a P wave appears that is not followed by a QRS complex
(d) Noting the irregular ventricular rhythm
#176 Lecture Outline
vii. Causes include:
(a) Ischemic heart disease
(b) Acute inferior wall or right ventricular MI
(c) Increased vagal tone
(d) Digoxin toxicity
(e) Certain electrolyte imbalances
(f) Administration of certain medicines
viii. The patient is usually symptomatic; if the patient develops bradycardia, treat in accordance to the bradycardia algorithm.
(a) When this rhythm occurs in conjunction with AMI, continuously monitor the patient for increasing AV block.
#177 Lecture Outline
d. Second-degree AV block type II
i. This is also called Mobitz type II second-degree block or type II AV block.
ii. More serious than second-degree AV block type I.
iii. Impaired conduction occurs within the bundle of His or, more commonly, the bundle branches.
iv. An intermittent block characterized by regularly occurring P waves and the abrupt appearance of at least one P wave that is not followed by a QRS complex
v. Ventricular rhythm is irregular because of the dropped QRS complexes.
(a) PRI always constant
(b) QRS complex:
(1) 0.11 second (110 ms) or less if the block occurs above or within the bundle of His
(2) Greater than 0.11 second (100 ms) if the block occurs below the bundle of His
#178 Lecture Outline
vi. Causes include:
(a) Ischemic heart disease
(b) Acute anterior wall MI
(c) Infectious heart diseases
(d) A cardiac surgery
vii. Symptoms include:
(a) Dizziness
(b) Fatigue
(c) Dyspnea on exertion
(d) Syncope
viii. Emergency care may require the use of TCP.
ix. Can progress to third-degree AV block without warning
x. Second-degree AV blocks can occur in patterns; it is difficult to determine if it is type I or type II.
(a) When two P waves appear for each QRS, it is a 2:1 AV block.
(b) When three P waves appear for each QRS, it is a 3:1 AV block.
xi. Usually, the QRS duration is a clue.
(a) Within normal limits in type I blocks
(b) Usually longer than normal in type II blocks
#179 Lecture Outline
e. Third-degree AV block
i. Also called complete heart block or complete AV block
ii. It occurs when all impulses reaching the AV junction are prevented from reaching the ventricles and generating a QRS complex.
(a) A secondary pacemaker assumes responsibility for impulse conduction.
iii. Look for nonconducted P waves and the absence of any relationship between the P waves and the QRS complexes.
iv. It usually has a regular rhythm, with consistent P-P and R-R intervals.
v. The P wave is upright with a nonexistent PRI.
vi. The ventricular rate, which depends on the activity of a secondary pacemaker is:
(a) 40 to 60 beats/min if the pacemaker originates in the AV junction
(b) 20 to 40 beats/min if it originates in the ventricles
vii. QRS complexes wider than 0.12 second (120 ms) are common.
viii. It can be produced by AMI, ischemic heart disease, hyperkalemia, or too high a dose of certain rate-control medications.
ix. Patients can be asymptomatic or symptoms may include:
(a) Fatigue
(b) Dyspnea
(c) Syncope
x. It is treated in the field only if it is associated with bradycardia.
#180 Lecture Outline
P. Artificial pacemaker rhythms
1. An artificial pacemaker consists of:
a. A pulse generator
b. Wire electrodes attached to one or more chambers of the heart
2. The pulse generator of a permanent pacemaker contains programmable hardware.
3. It is implanted in the subcutaneous tissue of the chest, below the right or left clavicle.
#181 Lecture Outline
4. Cause a unique vertical spike on the ECG tracing
a. Single-chamber pacemaker
b. Dual-chamber pacemaker (AV sequential)
c. Biventricular pacemaker
#182 Lecture Outline
5. There are two rate types.
a. Fixed rate pacemaker: seldom used today; generates a pacing impulse at a preprogrammed rate
b. Demand pacemaker: equipped with a sensor that generates a paced impulse when the patient’s heart rate has dropped below a predetermined rate (usually 60 beats/min)
#183 Lecture Outline
6. Sometimes an implanted pacemaker malfunctions.
a. Types of pacemaker failure include the following:
i. Failure to capture: Pacemaker spikes may be visible, but they will not be followed by a QRS complex.
(a) Dislodged wire connecting the patient’s heart to the pacemaker
(b) Battery depletion
(c) Ventricular perforation
ii. Failure to pace: Indicated on the ECG by the absence of pacemaker spikes at expected times
(a) Pulse generator failure
(b) Broken lead wire or dislodged lead
(c) Disconnected wire or cable
(d) Battery depletion
iii. Failure to sense: Indicated on the ECG by the appearance of pacemaker spikes within the P wave, QRS complex, or T wave; malfunction in which the pacemaker competes with the patient’s own intrinsic rhythm
(a) Pulse generator failure
(b) Broken lead wire or dislodged lead
(c) Excessively high sensitivity setting
(d) Battery depletion
iv. Oversensing: Indicated on the ECG by the occurrence of pacemaker spikes at a rate slower than the pacemaker’s preset rate, or by the absence of paced beats even though the pacemaker’s preset rate is faster than the patient’s rate; the pacemaker fails to generate an impulse because it has sensed extraneous signals and misinterpreted them as QRS complexes
v. Runaway pacemaker: A very tachycardic pacemaker rhythm that must be slowed to preserve the patient’s cardiac function; reset by placing a strong magnet over the pacemaker to recalibrate
b. If any of these malfunctions occurs, the patient’s heartbeat will depend on a natural pacemaker (usually the ventricles), causing greatly reduced CO.
c. TCP may be required to support CO until the pacemaker can be replaced.
#185 Lecture Outline
A. The purposes of a 12-lead ECG
1. Used to enable viewing of the heart from several angles to localize the site of cardiac injury or to identify dysrhythmias and other cardiac abnormalities
#186 Lecture Outline
2. Indications:
a. Before and after electrical therapy (defibrillation, cardioversion, pacing)
b. Chest pain or discomfort
c. Electrical injury
d. Known or suspected electrolyte imbalance
e. Known or suspected medication overdose
f. RVF and/or LVF
g. Post-syncope
h. Stroke
i. Syncope or near-syncope
j. Hemodynamic instability of unknown etiology
3. Devices capable of recording 12-lead ECGs contain interpretation software.
a. Rely on your own interpretation, not the automated findings.
b. Most devices are also capable of transmitting ECGs to the medical facility.
#187 Lecture Outline
B. Acquisition modes
1. Monitor mode or diagnostic mode
a. For rhythm interpretation, ECGs are recorded in monitor mode.
i. Uses electronic filters to remove artifact and other unwanted information
ii. Can skew shape and location of the ST segment and T wave
iii. Captures the range of 1 to 30, 40, 100, or 150 hertz (Hz)
#188 Lecture Outline
b. Diagnostic mode filters out very little electrical information, so there is more artifact on the tracing.
i. Captures electrical information within the range of 0.05 to 150 Hz
ii. Used to record a 12-lead ECG by default and cannot be changed
iii. Possible to record 3-lead ECGs in diagnostic mode
iv. Frequency range near the bottom of the ECG tracing
#189 Lecture Outline
C. Lead placement
1. The best way to learn how to record 12-lead ECG is to practice with the equipment.
2. When positioning the electrodes, make sure the patient does not get chilled as shivering will cause artifact.
3. To properly acquire a 12-lead ECG, refer to Skill Drill 18-6.
#190 Lecture Outline
D. Approach to the 12-lead ECG interpretation
1. A seven-step method to 12-lead ECG interpretation follows:
a. Review the snapshot.
b. Interpret the dysrhythmia.
c. Determine the axis.
d. Identify conduction system disturbances.
e. Evaluate chamber size.
f. Review for zones of ischemia, injury, and infarction.
g. Identify noncardiac causes.
#191 Lecture Outline
2. Review the snapshot.
a. Look at the tracing to see if anything stands out.
b. Check that all the leads are printed, if artifact is present, and if the rate is at either extreme.
#192 Lecture Outline
3. Interpret the dysrhythmia.
a. Five-step process to identify the underlying rhythm:
i. Identify the waves (P-QRS-T).
ii. Measure the PRI.
iii. Measure the QRS duration.
iv. Determine rhythm regularity.
v. Measure the heart rate.
#193 Lecture Outline
4. Determine the axis.
a. Vector: a quantity, such as force, that has magnitude and direction
b. QRS axis: a single vector that represents the mean of all vectors created by the ventricles during depolarization
#194 Lecture Outline
i. Viewed from lead I, the QRS wave will be:
(a) A positive deflection if heading toward the left arm
(b) A negative deflection if heading toward the right arm
#195 Lecture Outline
ii. Viewed from lead aVF, the QRS wave will be:
(a) A positive deflection if heading toward the patient’s feet
(b) A negative deflection if heading toward the patient’s head
c. Axis deviation
i. Refers to movement of the QRS axis to the right or left of its normal position.
ii. May provide important clues about the heart’s electrical activity, but it is not specific for any particular diagnosis.
iii. The fastest method to determine the QRS axis involves using the QRS complexes in leads I and aVF to create a simple quadrant system.
(a) The intersection represents the impulse origin, with the four quadrants where the impulse can travel.
#196 Lecture Outline
(1) Positive QRS in leads I and aVF: normal QRS axis
(2) Positive QRS in lead I and negative in lead aVF: left axis deviation
(3) Negative QRS in lead I and positive in lead aVF: right axis deviation
(4) Negative QRS in leads I and aVF: extreme right axis deviation
(b) If a ventricle is enlarged, it contributes more electrical energy, and the resulting electrical vector points in the direction of the hypertrophy.
(c) If an area of the ventricle is infarcted, it has no electrical energy, and the vector will point away from it.
#197 Lecture Outline
5. Identify conduction system disturbances.
a. Bundle branch blocks
i. A QRS complex with a bizarre appearance and a duration of longer than 0.12 second (120 ms) signifies some abnormality in conduction through the ventricles.
ii. A type of intraventricular conduction defect involving impaired conduction from the bundle of His to one or more of the bundle branches
iii. Right and left bundle branch blocks are the most common findings on the 12-lead ECG.
iv. Right bundle branch blocks (RBBBs): terminal R wave in lead V1
(a) QRS complex duration of 0.12 second (120 ms)
(b) Typically, the QRS complex appears as an rSR' complex (R-prime wave).
(c) Terminal S waves are also seen in leads I, aVL, and V6.
#198 Lecture Outline
v. Left bundle branch blocks (LBBBs): terminal S wave in lead V1
(a) QRS complex duration of 0.12 second (120ms)
(b) Terminal R waves are seen in leads I, aVL, and V6.
vi. RBBB or LBBB aberration describes the shape of the QRS complex in aberrantly conducted beats.
#199 Lecture Outline
b. Fascicular blocks
i. Also known as hemiblocks: occur when the anterior and posterior fascicles become diseased or ischemic and they cannot conduct electrical impulses
ii. Anterior fascicular block: rS complexes in leads II, III, aVF, and qR complexes in leads I and aVL
iii. Posterior fascicular block: qR complexes in leads II, III, and aVF, and rS complexes in lead I
#200 Lecture Outline
iv. Bifascicular block: a combination of two or more blocked fascicles or conduction pathways
(a) Combinations vary and produce different effects in different patients.
(1) RBBB and anterior hemiblock
(2) RBBB and posterior hemiblock
(3) Anterior hemiblock and posterior hemiblock (LBBB)
v. Trifascicular block: when all three components are blocked or impaired, with one component still occasionally providing AV conduction
vi. Concordant precordial pattern: when the QRS complexes in the precordial leads are all in the same direction
(a) Has several possible explanations, including improper lead placement, anterior wall MI, or VT
#202 Lecture Outline
a. Right atrial abnormality was formerly called right atrial enlargement or right atrial hypertrophy.
i. Right atrium will dilate if returning venous pressure is elevated or pulmonary pressures are high.
ii. Often associated with chronic pulmonary disorders
(a) Characterized by a P wave with an amplitude higher than 2.5 mm in lead II and/or higher than 1.5 mm in lead V1
(b) The duration of the P wave is usually normal.
#203 Lecture Outline
b. A left atrial abnormality is characterized by:
i. A P wave of normal height but prolonged duration of longer than 0.12 second (12 ms) in lead II
ii. A P wave with a notched appearance
iii. A biphasic P wave in lead V1 predominantly negative
c. Left atrial abnormality may be seen in patients with:
i. Valvular heart disease, such as mitral or aortic valve stenosis
ii. Hypertensive heart disease
iii. Cardiomyopathy
iv. CAD
v. An athletic heart
#204 Lecture Outline
d. Right ventricular hypertrophy
i. The enlargement of the right ventricle
ii. Usually caused by pulmonary hypertension
iii. An R wave that exceeds the height of the S wave in V1
#205 Lecture Outline
e. Left ventricular hypertrophy
i. The enlargement of the left ventricle, commonly due to systemic hypertension, but also from some cardiac abnormalities
ii. The left ventricular wall thickens due to an increase in workload.
iii. The left ventricle loses elasticity and fails to pump blood effectively, leading to heart failure.
iv. ECG criteria is typically based on QRS voltages.
(a) Deepest S wave in lead V1, plus
(b) Tallest R wave in V5/V6 taller than 35 mm, and/or
(c) R wave in lead aVL taller than 11 mm
v. Diagnosis is made by echocardiogram, not ECG.
#206 Lecture Outline
7. Review for zones of ischemia, injury, or infarction.
a. An infarction occurs when the ischemic process is not interrupted, resulting in tissue death.
i. Early recognition is key to limiting loss of heart tissue (ie, time is muscle).
b. When a coronary artery is blocked, there are characteristic changes that appear on the ECG:
i. ST-segment depression: ischemia
ii. ST-segment elevation: myocardial injury
iii. Pathologic Q waves: infarction
#207 Lecture Outline
iv. ST-segment depression greater than 0.5 mm in 2 or more contiguous leads in a patient with chest pain or discomfort: unstable angina or NSTEMI
#208 Lecture Outline
v. Suspect STEMI if:
(a) For leads V2 and V3, the ST-segment elevation is 2 mm or more in men older than 40 years or 1.5 mm or more in women, or
(b) It is elevated 1 mm or more at the J point in the other leads
vi. Nondiagnostic ECG: absence of ST-segment changes
(a) This does not rule out acute myocardial ischemia, injury, or infarction.
(b) Serial blood work and additional testing are required for diagnosis.
c. Early acquisition of a 12-lead ECG in a patient who may have an ACS is essential.
i. Obtain the first 12-lead ECG within 10 minutes of patient contact.
#209 Lecture Outline
d. Treatment decisions are made on the basis of:
i. The patient’s presentation and history
ii. The 12-lead ECG findings
iii. Any laboratory test results (ie, cardiac biomarkers)
#210 Lecture Outline
e. Correlate the patient’s cardiovascular anatomy with the heart surface viewed by each ECG lead.
i. Lead groups enable you to localize ECG areas that show changes consistent with ischemia, injury, or infarction.
f. Reciprocal changes represent a location in the chest wall opposite the infarction.
i. Mirror image J-point, ST-segment, and T-wave changes are seen on the ECG during an ACS.
ii. The presence of reciprocal changes is evidence of AMI, but absence is not diagnostic.
#211 Lecture Outline
g. Other cardiovascular conditions include two conditions that may produce ST-segment elevation, mimicking AMI.
i. Benign early repolarization
(a) Almost always a coincidental finding on ECG
(b) Characterized by ST-segment elevation, a J or fishhook appearance at the J point, and concave ST-segment morphology
(c) Often exclusive to the left precordial leads (V4 to V6) and/or inferior leads
(d) No reciprocal changes
#212 Lecture Outline
ii. Pericarditis
(a) Patients present with:
(1) Positional chest pain (often alleviated by sitting forward)
(2) Shortness of breath
(3) History of recent infection or fever
(b) Characterized by ST-segment elevation (not exceeding 5 mm) that is present in multiple leads and a depressed or down-sloping PR segment
(c) The PR segment is elevated or up-sloping in lead aVR.
(d) The ST segment is concave and reciprocal ST-segment depression is never seen.
#213 Lecture Outline
8. Identify noncardiac causes of ECG abnormalities.
#214 Lecture Outline
a. Pulmonary embolism
i. Can be identified by the presence of:
(a) An S1Q3T3 pattern
(1) Deep S wave in lead I
(2) Deep, narrow Q wave in lead III
(3) T-wave inversion in lead III
(b) New RBBB
(c) ST-segment depression in leads V1 to V3
ii. Thorough physical exam and to other pertinent information crucial
#215 Lecture Outline
b. Hypothermia
i. Patients may develop J waves (Osborne), which are often large and upright, occurring on the terminal wave of the QRS complex.
ii. The J wave may be accompanied by ST-segment depression and T-wave inversion.
iii. The more serious the condition, the larger the J wave.
iv. Reveals a bradycardic rhythm and baseline containing artifact from shivering and poor electrode adhesion
#216 Lecture Outline
c. Electrolyte imbalances
i. Hyperkalemia:
(a) Tall, peaked, asymmetric T waves develop.
(b) P waves can become flattened and disappear.
(c) In severe cases, QRS complex widens.
ii. Hypokalemia:
(a) Flat or seemingly absent T waves and U waves
#217 Lecture Outline
iii. Hypercalcemia may produce a shortened QT interval.
iv. Hypocalcemia may slightly lengthen the QT interval.
(a) Both lengthening and shortening are entirely due to length change in the ST segment.
(b) The T wave is unaffected by calcium concentration changes.
#218 Lecture Outline
d. Cardiomyopathy
i. A disease of the heart muscle
ii. The main types of cardiomyopathy: dilated, hypertrophic, and restrictive
iii. Dilated cardiomyopathy weakens the heart muscle, diminishing its ability to pump enough blood to the rest of the body and causing the heart to enlarge and stretch.
iv. Hypertrophic cardiomyopathy is a genetic condition in which the myocardial walls become very thick, impairing ventricular filling.
(a) Patients will experience (often associated with physical exercise):
(1) Shortness of breath
(2) Chest pain
(3) Syncope
(b) Often diagnosed in the patient’s 30s and 40s
(c) In most cases, the disease is inherited; in other cases, the cause is unclear or unknown.
(d) Characterized by deep, narrow Q waves in the inferior and high lateral leads and very tall R waves in the left precordial leads.
#219 Lecture Outline
v. With restrictive cardiomyopathy, the ventricular walls stiffen due to abnormal substances deposited between heart muscle cells throughout the heart or because the inner surface of the heart is lined with scar tissue.
(a) The rigidity of the ventricular walls hinders ventricular filling; the heart eventually loses its ability to pump adequately.
#220 Lecture Outline
e. Brugada syndrome
i. Genetic disorder involving sodium channels in the heart
ii. Characterized by:
(a) Incomplete RBBB
(b) ST-segment elevation that aggressively returns to baseline
(c) Changes in leads V1 to V2 (and possibly in V3)
iii. Often undiagnosed until adulthood
iv. Symptoms may include syncope, seizures, difficulty breathing, or SCA.
v. Although there is no cure, treatment options may include the use of medications, catheter ablation, or an implanted cardioverter-defibrillator.
#221 Lecture Outline
f. Long QT syndrome (LQTS)
i. Characterized by a QT interval exceeding approximately 0.44 second (440 ms)
ii. Patients are at increased risk of ventricular dysrhythmias, including torsades de pointes and VF.
iii. It is a result of:
(a) Genetic mutation of several genes
(b) Administration of certain drugs such as amiodarone
(c) Certain conditions such as hypocalcemia, AMI, and pericarditis
iv. Common symptoms include unexplained syncope, palpitations, or seizures.
#222 Lecture Outline
g. Intracranial hemorrhage
i. May cause deeply inverted, symmetric T waves in the precordial leads and a prolonged QT interval
ii. The patient will almost always have neurologic symptoms or be unresponsive.
#223 VI. Pathophysiology, Assessment, and Management of Specific Cardiovascular Conditions
#224 Lecture Outline
A. Epidemiology of CVD
1. Cardiovascular disease (CVD) is the leading cause of death in the United States.
2. Examples include angina pectoris, AMI, heart failure, hypertension, stroke, and diseases of the arteries.
#225 Lecture Outline
B. Acute coronary syndromes (ACSs)
1. Characterized by an abrupt reduction in blood flow through one or more coronary arteries.
2. If blood vessels become blocked:
a. Tissues are deprived of oxygen (ischemia).
b. When the ischemic process is not interrupted, tissue death occurs (infarction).
3. Etiology
a. The usual cause of an ACS is the rupture of an atherosclerotic plaque.
#226 Lecture Outline
b. Atherosclerosis affects the inner lining of blood vessels.
i. Leads to narrowing and blood flow reduction through those vessels
c. The atherosclerotic process is as follows:
i. Small amounts of fatty material are deposited along the arteries’ inner wall.
ii. Fat gradually enlarges and becomes a mass of fatty tissue (atheroma).
iii. The atheroma eventually calcifies and hardens into a lesion.
iv. The lesion infiltrates the arterial wall and diminishes its elasticity, while decreasing the amount of blood flow through the lumen.
d. This area is an ideal site for the formation of a thrombus, which can obstruct the artery altogether.
e. Calcium may precipitate into the arterial walls, causing arteriosclerosis, reducing arterial elasticity.
f. Obstructive CAD exists when an individual has stenosis of 50% or more of a coronary vessel.
#227 Lecture Outline
4. Types of risk factors
a. Nonmodifiable risk factors cannot be changed.
b. Modifiable risk factors can be controlled, modified, or treated.
5. Risk factors for CHD
a. Health conditions:
i. Diabetes
ii. High levels of blood cholesterol and other lipids
iii. High BP
iv. Obesity
b. Lifestyle habits:
i. Physical inactivity
ii. Excessive alcohol consumption
iii. Tobacco smoking
c. Nonmodifiable risk factors:
i. Genetics and family history
ii. Increasing age
iii. Sex
iv. Race
d. Contribution risk factors:
i. Geography and socioeconomic circumstances
ii. Stress
iii. Some cancer therapies
#228 Lecture Outline
6. Angina pectoris
a. Principal symptom of CAD
i. Pain that occurs when the oxygen supply to the myocardium is not enough to meet the demand.
(a) A switch to anaerobic metabolism leads to buildup of carbon dioxide and lactic acid.
(b) During exercise or other physiologic stress, the patient may not have enough blood flowing to the myocardium to satisfy the increased demand for oxygen.
(c) If angina occurs at rest, the patient has more severe CAD.
#229 Lecture Outline
ii. It is important to distinguish between stable and unstable angina.
(a) Stable angina: follows a recurrent pattern
(1) Pain occurs after a predictable amount of exertion, with a predictable location, intensity, and duration.
(2) Patients often take some form of NTG.
(3) ST-segment depression or inverted T waves show on ECG.
(4) ECG changes resolve when the heart’s oxygen demand is met.
(b) Unstable angina: more serious and indicates a higher level of coronary artery obstruction
(1) Characterized by changes in frequency, severity, and duration of pain and other symptoms
(2) More frequent and severe attacks, which may begin during sleep or at rest
(3) Warning signs of an impending MI
#230 Lecture Outline
(c) Variant angina: caused by coronary artery vasospasm and results in chest pain at rest
(1) Brought on by emotional stress, exertion, or cold weather
(2) Can occur in patients with normal coronary arteries as well as in patients with CAD
(3) ST-segment elevation common on the ECG
(4) Resolution of symptoms on their own or with NTG
#231 Lecture Outline
(d) Microvascular angina (MVA): caused by constriction or spasm within the smallest coronary artery walls
(1) Often underrecognized and untreated because coronary angiography fails to show obstructive CAD or spasm of the epicardial coronary arteries
(2) More common in women and people with diabetes or hypertension
(3) Chest discomfort may be more intense and prolonged.
(4) May be accompanied by complaints of fatigue, shortness of breath, and sleep disturbances
(5) ST-segment depression during exercise
#232 Lecture Outline
7. Acute myocardial infarction (AMI)
a. Part of the cardiac muscle is deprived of coronary blood flow long enough that portions of the muscle die.
b. The location and size of the infarct depend on which artery is blocked and where along its course the blockage occurs.
i. Most infarcts involve the left ventricle.
ii. When the anterior, lateral, or septal wall of the left ventricle are infarcted, it is usually from occlusion of the left coronary artery or one of its branches.
iii. RCA occlusion usually causes inferior wall infarcts.
c. Subendocardial myocardial infarction is when the ischemic process affects the inner layer of muscle only.
d. Transmural myocardial infarction is when the infarct extends through the entire wall of the ventricle.
#233 Lecture Outline
e. Infarcted tissue is surrounded by a ring of ischemic tissue that is relatively deprived of oxygen but still viable.
i. The tissue is electrically unstable and may be the source of cardiac dysrhythmias.
f. Patients with STEMI have ECG evidence of ST-segment elevation.
g. NSTEMI produces no sign of myocardial injury on the patient’s ECG.
h. Distinguishing patients with unstable angina from those with AMI may be impossible during initial presentation.
i. Signs, symptoms, and ECG finding associated with these two conditions may be identical.
#234 Lecture Outline
8. Assessment
a. Goals:
i. Identify whether STEMI is present and, if so, notify the medical facility.
ii. Determine the time of symptom onset.
iii. Monitor cardiac rhythm and vital signs; be prepared to provide CPR and defibrillation, if needed.
iv. Administer appropriate medications.
v. Transport to an appropriate facility.
#235 Lecture Outline
b. Symptoms
i. The most common symptom is chest discomfort.
(a) Although some patients will have a history of stable angina, ACS will be the initial presentation of CAD in others.
(b) Pain is felt just beneath the sternum and may be described as:
(1) Heavy
(2) Squeezing
(3) Crushing
(4) Tight
(c) The pain radiates to the arms and into the fingers and may radiate to the neck, jaw, upper back, or epigastrium.
(d) The pain is dull and unaffected by deep inspiration, movement, or position and may or may not be relieved by nitrates or rest.
(e) The patient often unconsciously clenches a fist when describing the pain (Levine sign).
(f) The pain is sometimes mistaken for indigestion.
#236 Lecture Outline
ii. Not every ACS patient has chest discomfort.
(a) Silent MI
(b) Others may present solely with dyspnea or with arm, shoulder, back, jaw, neck, epigastric, or ear discomfort (anginal equivalents).
#237 Lecture Outline
iii. Atypical or unusual symptoms are more common in women, older adults, and patients with diabetes.
(a) Women
(1) Chest discomfort that presents as aching, tightness, pressure, burning
(2) Discomfort that may come and go, often in the back, shoulder, or neck
(3) Shortness of breath
(4) Weakness
(5) Nausea and vomiting
#238 Lecture Outline
(b) Older adults
(1) Compromised mental status
(2) Generalized weakness
(3) Syncope
(4) Shortness of breath
(5) Abdominal or epigastric discomfort
(c) Patients with diabetes
(1) Generalized weakness
(2) Syncope
(3) Light-headedness
(4) Diminished mental status
#239 Lecture Outline
iv. When obtaining a history, ask the usual SAMPLE and OPQRST questions, but also determine if the patient has taken any pain medication and if it helped.
(a) If the patient took NTG and got no relief, establish why the pain was unrelieved.
(1) The patient may be having an ACS.
(2) The NTG may have gone stale.
(b) Ask if the patient whether the last few doses of NTG have had the usual effects.
(1) Slight burning on the tongue
(2) Feeling flushed
(3) Transient throbbing headache
v. Use a pain rating scale when assessing the severity of the patient’s discomfort.
vi. As soon as a cardiac condition is established, start treatment.
vii. Other symptoms include:
(a) Diaphoresis, often profuse
(b) Dyspnea as a warning sign of impending LVF
(c) Anorexia, nausea, vomiting, belching
(d) Profound weakness
(e) Dizziness caused by diminished CO
(f) Palpitations
(g) A feeling of impending doom, panic, and dread
#240 Lecture Outline
c. Signs
i. Patients may have relatively normal physical exam finding, with the diagnosis depending mostly on history and 12-lead ECG findings.
ii. Take note of:
(a) Patient’s general appearance
(b) Patient’s level of responsiveness
(c) Skin
(d) Vital signs
(e) Signs of LVF
(f) Signs of RVF
#241 Lecture Outline
9. Management of ACSs
a. Among patients with an ACS, those with STEMI are most likely to benefit from reperfusion therapy.
i. Start treatment at once on arrival at the scene for any patient with chest discomfort because the benefits are time sensitive.
(a) Even before you complete the history or secondary assessment
b. Refer to the ACS algorithm in Figure 18-103 of the text.
#242 Lecture Outline
c. Place the patient at physical and emotional rest.
i. The stress response triggers the release of catecholamines, which can make the damaged heart race.
ii. The massive discharge places the peripheral circulation in a state of severe vasoconstriction.
iii. The heart has to work harder against increased afterload.
iv. The heart’s need for oxygen increases.
v. This cycle can lead quickly to dysrhythmias and death.
#243 Lecture Outline
vi. To begin treatment, place the patient in a semi-Fowler position.
(a) Do not allow the patient to walk to the stretcher.
(b) From the first point of paramedic arrival, the patient must not do anything.
d. Obtain vital signs and perform cardiac monitoring.
i. Obtain the vital signs.
(a) Measure the blood pressure at least every 5 minutes.
(b) Measure pulse rate.
#244 Lecture Outline
ii. Perform cardiac monitoring.
(a) Listen for rhythm irregularities.
(b) Keep your cardiac drugs close at hand.
(c) Treat pulseless rhythms, tachycardia, and symptomatic bradycardia in accordance with the algorithm for each respective dysrhythmia.
(d) Initiate CPR, defibrillation, or cardioversion, if indicated.
#245 Lecture Outline
e. Administer aspirin and oxygen.
i. In most EMS systems, dispatchers may advise patients to chew baby aspirin (160 to 325 mg) unless there is an allergy.
(a) Do so, if not done before your arrival.
ii. If the patient is dyspneic, hypoxemic, or has obvious signs of heart failure, administer oxygen to maintain an Spo2 level of 90%.
#246 Lecture Outline
f. Obtain a 12-lead ECG.
i. Obtain a 12-lead ECG within 10 minutes of patient contact, while another crew member establishes vascular access.
(a) Perform before administering any medication (except possibly aspirin and oxygen).
(b) Repeat the 12-lead ECG with each set of vital signs, when symptoms change, and as often as necessary.
#247 Lecture Outline
ii. In patients whose symptoms suggest ischemia or infarction, the 12-lead ECG allows for rapid stratification into one of three categories:
(a) STEMI
(b) NSTEMI
(c) Normal (nondiagnostic)
#248 Lecture Outline
iii. STEMI treatment requires reperfusion therapy either by:
(a) Percutaneous coronary intervention (PCI)
(b) Administration of a fibrinolytic medication
iv. You should know which medical facilities in your area are equipped to administer fibrinolytic therapy and/or PCI.
v. Fibrinolytic therapy involved administering a medication that converts the body’s clot-dissolving enzyme from its inactive form (plasminogen) to its active form (plasmin).
(a) Medication can lead to uncontrolled bleeding.
#249 Lecture Outline
vi. The ideal STEMI system should include:
(a) Trained EMS dispatchers
(b) Well-established EMS triage and destination protocols
(c) 12-lead ECG acquisition and interpretation capability
(d) ED protocols
(e) Staff experienced in ACLS
#250 Lecture Outline
(f) Ability to communicate with the receiving institution
(g) Medical direction with training and experience in managing STEMI
(h) Interfacility transfer protocols
(i) Post–acute care capabilities
(j) Quality assurance/continuous quality improvement
#251 Lecture Outline
vii. Not all EMS systems are able to support a STEMI system.
(a) When a STEMI system of care exists, and transport times will be more than 30 minutes, administer fibrinolytics in the prehospital setting.
(b) When both prehospital fibrinolysis and direct transport to a PCI center are available, transport may be preferred.
viii. The following concepts referring to the elapsed time before the patient receives reperfusion therapy must be minimized:
(a) EMS-to-balloon time
(b) Door-to-balloon time
(c) Door-to-needle time
ix. Transport and destination decisions should be based on local resources and systems of care.
#252 Lecture Outline
g. Provide pain relief.
i. Administer NTG sublingually as a 0.4-mg tablet or metered-dose spray.
ii. Administer NTG if you are sure there are no contraindications to its use.
(a) Ensure that the patient does not have an initial SPB less than 90 mm Hg.
(b) Do not administer if the patient has used a phosphodiesterase inhibitor within the past 48 hours.
(1) Sildenafil (Viagra, Revatio) or tadalafil (Cialis, Adcirca)
(c) Avoid use in patients receiving IV epoprostenol (Flolan) or treporstenil (Remodulin) to treat hypertension
(d) Avoid administering NTG if right ventricular infarction is suspected.
(1) Hypotension can result when preload is reduced.
(2) Apply right-sided chest leads to assess right ventricular involvement.
iii. If the patient’s discomfort persists and his or her vital signs remain stable, consider administering morphine sulfate.
(a) Preferred analgesic for patients with unstable angina/STEMI
(b) Adverse effects in patients with unstable angina/STEMI
iv. Fentanyl (Sublimaze) is favored over morphine in some EMS systems because of its rapid onset, relatively short duration, and fewer side effects.
v. Follow local protocols.
#253 Lecture Outline
h. Transport the patient.
i. Once the patient is stable, transport in a semi-Fowler position.
(a) Ensure the patient is as relaxed and comfortable as possible.
(b) Additional treatment may be advisable, especially for long transports.
#254 Lecture Outline
ii. Some patients refuse care despite having signs and symptoms consistent with an ACS.
(a) A person with chest discomfort who refuses care is an example of a high-risk refusal.
(b) Calmly try to persuade the person to accept the care you wish to provide, including transport.
(c) If you suspect an MI, tell the patient.
(1) Use nonmedical language: heart attack instead of MI
(2) Explain the risks (including death) and benefits of not accepting care.
(3) Contact medical direction if necessary.
(4) If unable to convince the patient, document refusal.
#255 Lecture Outline
10. Patient and family education
a. Teach your patients and their families how to recognize the signs and symptoms of a heart attack.
b. Instruct them to call 9-1-1 within 5 minutes of symptom onset.
c. Explain to them that:
i. Not all heart attacks are accompanied by sudden chest pain and a loss of responsiveness.
ii. Symptoms may begin gradually or they may come and go.
d. Advise patients who have had a previous heart attack that the signs and symptoms of a second or subsequent cardiac event may differ from those of the first.
#256 Lecture Outline
C. Heart failure
1. Occurs when the heart cannot pump fast enough or powerfully enough to empty its chambers
a. Blood backs up into the systemic circuit, pulmonary circuit, or both.
b. Heart failure is a syndrome, not a disease, characterized by volume overload and inadequate tissue perfusion.
#257 Lecture Outline
2. Common features:
a. Fatigue
b. Dyspnea
c. Edema
d. Exercise intolerance
#258 Lecture Outline
3. Causes
a. Disorders that impair the ventricles’ ability to fill with or eject blood, such as:
i. CAD (most common cause)
ii. Long-standing high BP
iii. Diabetes
iv. Dysrhythmias
v. Cardiomyopathy
vi. Valvular heart disease
vii. Genetic conditions
#259 Lecture Outline
Factors that contribute to heart failure
a. Thyroid disorders
b. Alcohol or illegal substance abuse
c. Cancer treatments that damage the myocardium
d. Infectious agents that cause inflammation
#260 Lecture Outline
5. Identified based on:
a. Symptom onset (acute verses chronic)
b. Ventricle initially involved (left verses right)
i. REF is often a result of LVF.
#261 Lecture Outline
6. Review of the physiology of the normal heart
a. CO is equal to stroke volume multiplied by the heart rate.
b. Three factors affect stroke volume.
i. Preload
ii. Afterload
iii. Cardiac contractility
c. Any condition that impairs preload, afterload, cardiac contractility, or heart rate can cause heart failure.
#262 Lecture Outline
7. Left ventricular failure
a. Blood backs up behind it, causing a chain reaction.
i. The right side continues to pump normally.
ii. The left side cannot keep up, and pressure increases.
iii. Pressure within the pulmonary vessels increases.
iv. Fluid is forced out of the pulmonary capillaries into the alveoli (pulmonary edema).
v. The buildup of fluid widens the gap between the alveoli/capillary membrane, impairing the diffusion of oxygen and carbon dioxide.
#263 Lecture Outline
b. Two types
i. Systolic failure: Left ventricle is weak and has trouble pumping out all the blood in the chamber to the body
ii. Diastolic failure: Left ventricle contracts normally but has become stiff, impeding its ability to relax and fill with blood between contractions
c. Possible causes
i. Poorly controlled hypertension
ii. Tachydysrhythmias
iii. Permanent damage to the myocardium due to CAD
iv. Increased demands on the heart associated with excessive volume or pressure
#264 Lecture Outline
8. Right ventricular failure
a. To eject the blood within its walls, the right ventricle must overcome high pressure and congestion within the pulmonary vessels.
i. When it cannot keep up with the increased workload, the right ventricle fails.
#265 Lecture Outline
ii. Blood backs up behind the right ventricle, raising pressure in the right atrium.
(a) Blood backs up into the superior and inferior venae cavae.
(b) The veins become congested with blood.
(c) Organs become congested with blood.
(d) Rising pressure within the veins forces serous fluid through capillary walls and into body’s tissues, producing edema.
(e) Peripheral edema is most apparent in the feet and ankles.
(f) Serous fluid may also build up in:
(1) The abdomen (ascites)
(2) Pleural cavity (pleural effusion)
(3) Pericardial cavity (pericardial effusion)
(g) As RVF progresses, generalized edema of the entire body may occur (anasarca).
#266 Lecture Outline
b. Cor pulmonale
i. RVF may occur by itself (without LVF) in conditions such as:
(a) RVI
(b) Pulmonary embolism
(c) Pulmonary hypertension
ii. Pulmonary hypertension is a disorder in which the pressure in the pulmonary arteries is higher than normal.
(a) The right ventricle must work hard to overcome increased resistance to eject blood.
(b) The right ventricle enlarges and eventually fails.
iii. RVF caused by pulmonary disease is called cor pulmonale.
(a) Usually the result of COPD
#267 Lecture Outline
9. Compensatory mechanisms
a. Compensatory mechanisms attempt to improve CO by manipulating the following:
i. Preload
ii. Afterload
iii. Cardiac contractility
iv. Heart rate
b. Ultimately, compensatory mechanisms may worsen heart failure.
i. The sympathetic nervous system
(a) Boosts the heart rate
(b) Increases the force of contraction
(c) Constricts blood vessels
#268 Lecture Outline
ii. The accelerated heart rate and stronger force of contraction
(a) Increase the heart’s oxygen demand
(b) Reduce the amount of time the ventricles have to fill
(c) Decrease time for coronary artery perfusion
#269 Lecture Outline
iii. Stimulation of the renin-angiotensin-aldosterone system by decreased blood flow to the kidneys
(a) Angiotensin I forms angiotensin II, promoting more vasoconstriction.
(b) The heart has to work even harder to pump against high pressure.
(c) Aldosterone II encourages sodium and water retention and increased blood volume (increased preload).
#270 Lecture Outline
c. Compensatory mechanisms increase CO for a time, but eventually heart failure advances.
i. Sodium and water retention enlarges the heart’s chambers.
ii. Ventricle walls thicken, weakening the force of contraction.
iii. The force of contraction decreases.
iv. The heart is unable to handle the increased volume of fluid, and CO decreases.
#271 Lecture Outline
10. Assessment
a. The patient may report:
i. A sudden onset of shortness of breath
ii. A shortness of breath that has worsened over a period of hours or days (persists even at rest)
b. The likelihood of a cardiac origin is greater if the patient has a history of:
i. Previous heart attack
ii. High blood pressure
iii. Valvular disease
iv. Cardiovascular condition(s)
c. The patient may report having had trouble sleeping.
i. The patient may have episodes of PND.
d. The patients often report feeling tired or weak.
e. The patient may report having had trouble concentrating.
i. May be the result of hypoxia
f. Other symptoms include:
i. Nausea and a loss of appetite
ii. Feelings of faintness, palpitations, or an irregular or rapid pulse
(a) Ask the patient about prescribed medications, specifically beta-blockers or calcium channel blockers.
iii. Restlessness, anxiety, or unexplained confusion (might be result from hypoxia)
g. The sympathetic nervous system’s response to hypoxia and the body’s compensatory mechanism to maintain CO cause these symptoms:
i. Rapid respiratory rate and heart rate
ii. Pale and cool skin
iii. Diminished peripheral pulses
iv. Increased work of breathing
h. As hypoxia worsens, the patient may become cyanotic or may cough frequently.
i. Coughing may produce pink, frothy sputum.
ii. Buildup of fluid in the lungs causes crackles (rales) and/or wheezing.
i. If RVF accompanies LVF, then jugular venous distention (JVD) will be visible as the venous system becomes congested.
i. Patients who can walk will have swelling of the ankles, feet, calves, or legs.
ii. Patients confined to bed may have swelling of the sacral area.
(a) If edema is present, note (and document) if it is pitting or nonpitting and localized in the ankles, to the mid-calf, or to the knees.
iii. Ascites may also occur.
j. As the pump continues to fail, the heart rate begins to slow, blood pressure falls, and CO decreases substantially.
k. Cardiogenic shock occurs when heart failure is accompanied by hypotension.
#272 Lecture Outline
l. Signs and symptoms present with heart failure may be present with other conditions.
#273 Lecture Outline
11. Management
a. Offer the patient reassurance.
b. Place the patient in a position of comfort.
i. Place them in a sitting position with the feet dangling.
(a) Encourages venous pooling in the legs, which reduces venous return to the heart
(b) Decreases the work of breathing
c. Apply a pulse oximeter.
d. Provide supplemental oxygen as needed to maintain the patient’s Spo2 between 95% and 98%.
i. Use noninvasive positive-pressure ventilation (NIPPV) to manage pulmonary edema associated with heart failure.
ii. Do not use noninvasive positive-pressure ventilation if the patient has:
(a) Compromised airway
(b) Altered mental status
(c) Risk of aspiration
(d) Pneumothorax
(e) SBP of less than 90 mm Hg
iii. It may be necessary to use an advanced airway.
e. Monitor the patient’s respiratory status using waveform capnography.
#274 Lecture Outline
f. Limit the patient’s physical activity.
g. Place the patient on a cardiac monitor and obtain a 12-lead ECG.
h. Establish IV access.
i. Use a heparin lock or saline lock to distribute the correct amount of IV fluid.
ii. If an IV bag and tubing is used, infuse the fluid at a “to keep open” rate (30 mL/h).
iii. Document the amount of fluid in the bag throughout patient care.
i. Pharmacologic therapy for heart failure may vary slightly by EMS system, so check your local protocol.
i. Sublingual NTG may be given to reduce both preload and afterload, thereby supporting CO.
ii. Furosemide is not currently recommended for use in treating heart failure and acute pulmonary edema.
j. Avoid using lights and siren during transport to prevent an increase in a stable patient’s anxiety, heart rate, and BP.
#275 Lecture Outline
k. Surgically implanted ventricular assist devices (VADs) may be used in patients who have heart failure.
i. Acts as an artificial ventricle
ii. Does not depend on the contractility or electrical conduction of the patient’s heart
iii. Can be placed in the left ventricle (LVAD), the right ventricle (RVAD), or both (biventricular assist device)
iv. LVF is more common than RVF, so the LVAD is the most common type of VAD.
v. A VAD may be used in the following situations.
(a) To allow the heart to rest until the patient’s heart can resume its pumping function
(b) As a bridge to heart transplantation
(c) As lifetime therapy (also called destination therapy)
#276 Lecture Outline
vi. There are several types of VADs, and they typically consist of:
(a) A blood pump
(b) Tubing (an inflow cannula and an outflow cannula)
(c) An external power source that connects to a controller
(d) Alarms
vii. VADs are categorized according to:
(a) Type of blood flow (eg, continuous, pulsatile)
(b) The length of time the device can be used for circulatory support (eg, short, intermediate- or long-term)
(c) The source of driving power (eg, pneumatic or electric)
(d) Device location (eg, internal or external)
viii. The patient’s weak or absent pulse may make obtaining a blood pressure using a manual cuff and stethoscope and obtaining a pulse oximetry reading difficult.
#277 Lecture Outline
ix. Types of VADs include:
(a) Transcutaneous VADs: Both the pump and power source are located externally.
(b) Implantable VADs: The pump is located inside the body, and the power source is located externally.
(c) LVADs: Blood is withdrawn from the left atrium or the apex of the left ventricle through a tube into the LVAD and is then returned to the ascending aorta via a second tube.
(d) RVADs: Blood is withdrawn from the right atrium into the RVAD and is returned to the pulmonary artery.
x. Complications with VADs include:
(a) Device malfunction or failure
(b) Thromboembolism
(c) Bleeding
(d) Heart failure
(e) Infection
(f) Dysrhythmias
(g) Cardiac tamponade
(h) Aortic insufficiency
(i) Sepsis
#278 Lecture Outline
xi. To assess for possible VAD pump malfunction:
(a) Assess for alarms.
(b) Auscultate for a “hum” from the pump.
(c) Assess for signs of hypoperfusion.
xii. Use available resources to troubleshoot potential VAD malfunctions and determine the appropriate corrective actions.
(a) Contact the patient’s VAD-trained companion, if available.
(b) Check all the system controller connections, change the VAD batteries, and/or change the system controller.
(c) Have the patient stop all activity and assess patient tolerance.
xiii. Contact the VAD coordinator if the patient with a VAD experiences a cardiac arrest.
(a) If the patient requires defibrillation or cardioversion, be careful not to place the pads directly over the pump.
(b) Bring all VAD-related equipment when transporting the patient to a non-VAD center.
#279 Lecture Outline
D. Cardiac tamponade
1. Pathophysiology
a. Occurs when the buildup of pericardial fluid compresses the heart, impairing contraction and restricting ventricular filling
b. May develop:
i. Gradually if caused by an infection or tumor
ii. Rapidly when caused by heart surgery, pacemaker or central venous catheter insertion, or cardiac trauma such as a stab wound or gunshot wound
#280 Lecture Outline
2. Assessment
a. The patient is usually too ill to give his or her medical history.
i. Symptoms
(a) Anxiety and restlessness
(b) Shortness of breath
(c) Chest tightness
(d) Dizziness
b. Suspect cardiac tamponade in any patient with a penetrating wound of the chest or upper abdomen.
i. If it is not from trauma, the patient may have a history of a medical illness such as pericarditis or end-stage renal disease.
(a) Differentiate between a tamponade and tension pneumothorax; in cardiac tamponade, the lungs are not affected, so:
(1) Breath sounds will be equal
(2) Trachea will be midline
c. Cardiac tamponade produces a classic trio of signs known as Beck triad:
i. JVD
ii. Hypotension
iii. Muffled heart sounds
(a) Signs are present in fewer than half of all patients.
d. Other signs of cardiac tamponade:
i. Cold, mottled, or cyanotic skin; pallor
ii. Tachycardia
iii. Weak or absent peripheral pulses
iv. Narrowing pulse pressure (early sign)
v. Pulsus paradoxus (late sign; may be absent if the patient has severe hypotension)
vi. Signs and symptoms mimicking heart failure
e. ECG is of limited value.
i. May show electrical alternans
3. Management
a. If trauma is the source of the patient’s signs and symptoms:
i. Address any life-threatening hemorrhage.
ii. Ensure adequate oxygenation and ventilation.
iii. Apply a pulse oximeter and provide supplemental oxygen as needed to maintain the patient’s Spo2 between 95% and 98%.
iv. Apply the cardiac monitor.
v. Avoid performing additional procedures that might delay transport.
b. Establish IV access en route to definitive care.
i. Give IV fluids as a temporizing measure, but do not delay transport to initiate this intervention.
c. Pericardiocentesis is the ultimate treatment to withdraw fluid.
i. A needle is inserted into the pericardial space to aspirate excess fluid.
ii. Withdrawal of as little as 50 mL may give significant improvement.
iii. Transport to a facility that can do this procedure.
#281 Lecture Outline
E. Cardiogenic shock
1. Severe impairment of heart muscle function
a. Decreases CO and results in inadequate tissue perfusion
b. Most common cause is LVF secondary to AMI
#282 Lecture Outline
b. Pathophysiology
a. May occur as a complication of shock of any cause
b. May also occur if myocardial contractility has diminished because of prolonged cardiac surgery, ventricular aneurysm, cardiac arrest, or ventricular wall rupture
i. Transient cardiogenic shock can occur after resuscitation.
#283 Lecture Outline
c. Risk factors:
i. Older age
ii. Anterior MI
iii. Diabetes
iv. Hypertension
v. Multivessel CAD
vi. Previous MI
vii. Peripheral vascular or cerebrovascular disease
#285 Lecture Outline
a. Warm and dry
i. Signs of heart failure
ii. No pulmonary congestion
iii. Tachycardia
b. Warm and wet
i. Vasodilation
ii. Pulmonary congestion
iii. Tachycardia and fever
#286 Lecture Outline
c. Cool and dry
i. Peripheral vasoconstriction
ii. No pulmonary congestion
iii. Tachycardia
iv. Narrowed pulse pressure
v. Acute mental status change
vi. Dizziness
#287 Lecture Outline
d. Cold and wet (most common presentation)
i. Cold skin
ii. Pulmonary crackles on auscultation
iii. Ashen or cyanotic with mottled extremities
iv. Altered mental status
v. Dyspnea, orthopnea, JVD
vi. Peripheral edema
vii. Third and fourth heart sounds may be heard
viii. Decrease in SBP
#288 Lecture Outline
e. If family members are present, ask whether the patient has a history of heart disease.
i. Ask if the patient has been taking their medications as prescribed.
#289 Lecture Outline
4. Management
a. Prehospital management
i. Ensure adequate oxygenation and ventilation
ii. Establish vascular access
iii. Continuously monitor ECG
iv. Transport for definitive care
#290 Lecture Outline
b. In the hospital setting, treatment focuses on strengthening contractility without significantly increasing the heart rate, altering preload and afterload, and controlling any dysrhythmias contributing to shock.
c. Place a hypotensive patient in a supine position.
i. If pulmonary congestion is present, place the patient in a sitting position with the feet dangling.
ii. Limit the patient’s physical activity.
#291 Lecture Outline
d. Obtain the patient’s vital signs.
i. Apply a pulse oximeter and administer supplemental oxygen as indicated.
ii. Place the patient on a cardiac monitor and obtain a 12-lead ECG within 10 minutes of patient contact.
e. Consult medical direction before administering IV fluids or medications.
#292 Lecture Outline
i. Vasoactive IV medications to treat cardiogenic shock include:
(a) Dopamine
(b) Norepinephrine
(c) Epinephrine
ii. If instructed to give a vasoactive medication, check the following:
(a) The IV site often
(b) The patient’s response
f. Except for correcting a life-threatening dysrhythmia, there are no other measures to take in the field to stabilize a patient in cardiogenic shock.
i. Complete a fibrinolytic checklist en route.
#293 Lecture Outline
g. If the patient refuses care, repeatedly urge the patient to accept assistance.
i. Consider contacting medical direction for advice.
ii. Document the patient’s refusal.
#294 Lecture Outline
F. Hypertensive emergencies
1. Definitions
a. Hypertension is an SBP exceeding 140 mm Hg or a diastolic pressure exceeding 90 mm Hg.
i. Modifiable risk factor for:
(a) Stroke
(b) AMI
(c) Heart failure
(d) Dementia
(e) Peripheral vascular disease
(f) Aortic dissection
(g) AF
(h) End-stage renal disease
ii. Called the “silent killer” because it usually produces no signs or symptoms
iii. Damages the heart, brain, eyes, blood vessels, and kidneys
b. A hypertensive emergency is defined as an acute elevation of blood pressure to 180/120 mm HG or higher with evidence of end-organ damage.
i. A common cause is failure to take blood pressure medications or other treatments as prescribed.
ii. Usually occurs in patients with a history of hypertension
iii. Causes include:
(a) Acute aortic dissection
(b) Acute CNS events
(c) Acute kidney failure
(d) Drug-induced hypertension from recreational drug use
(e) Pheochromocytoma
(f) Toxemia of pregnancy
c. Hypertensive urgency exists when there is an acute elevation of BP to 180/120 mm Hg or higher without signs or symptoms of end-organ damage.
#295 Lecture Outline
2. Pathophysiology
a. Most cases result from advanced atherosclerosis or arteriosclerosis.
b. Many conditions, such as anxiety or pain, and briefly elevate a person’s BP
i. A single reading does not constitute hypertension.
(a) Suggest the patient have their blood pressure rechecked a couple times in the following weeks.
#296 Lecture Outline
c. Persistent elevation of diastolic pressure is indicative of hypertensive disease, which can:
i. Significantly shorten a life span
ii. Predispose the person to other medical conditions, including:
(a) Renal damage
(b) Stroke
(c) Heart failure
d. Hypertensive emergencies require rapid lowering of blood pressure to prevent or limit organ damage.
i. May cause acute renal failure, AMI, stroke, or death within a few hours if left untreated
#297 Lecture Outline
3. Assessment
a. Hypertensive emergencies often develop rapidly.
b. Neurologic signs and symptoms:
i. Headache
ii. Blurred vision or sudden blindness
iii. Aphasia
iv. Numbness or weakness
v. Mental status changes ranging from confusion to unresponsiveness
vi. Widespread neuromuscular irritability
c. Cardiovascular signs and symptoms:
i. Chest pain or tightness
ii. Shortness of breath
iii. Palpitations
iv. Dysrhythmias
v. Signs of heart failure
vi. Sudden severe chest or upper back pain that may indicate aortic dissection
d. Additional signs and symptoms:
i. Decrease or absence of urine output
ii. Nausea/vomiting
iii. Ringing in the ears (tinnitus)
iv. Nosebleed
v. Muscle cramps
#298 Lecture Outline
e. Peripheral pulses may feel strong or bounding.
i. Check and document the patient’s BP in both arms in case aortic dissection has occurred.
ii. Seizures, signs of heart failure, or signs consistent with AMI
iii. Ischemic changes may be seen on the 12-lead ECG.
f. Ask the patient about what medications they take:
i. Prescribed and over-the-counter medications
ii. Recreational drug use
#299 Lecture Outline
4. Management
a. Provide supportive care.
i. Administer oxygen.
ii. Establish an IV line.
iii. Apply the cardiac monitor and pulse oximeter.
(a) Maintain the Spo2 between 95% and 98%.
iv. Do not delay transport.
v. Provide care according to local protocol for patients with heart failure or chest discomfort.
vi. Offer reassurance to the patient and family.
#300 Lecture Outline
vii. If a long transport time is unavoidable, paramedics may need to initiate drug therapy in the field.
(a) Labetalol (Normodyne, Trandate): Alpha- and beta-blocking properties decrease overall peripheral vascular resistance and prevent reflex tachycardia
(1) Contraindicated in patients with asthma and COPD
viii. Keep the patient supine.
ix. Measure the blood pressure at least every 2 to 3 minutes.
x. Stop the infusion when the blood pressure has fallen to the target level.
b. A patient with a hypertensive emergency requires transport to the closest appropriate facility.
#301 Lecture Outline
c. If the patient refuses care, repeatedly urge the patient to accept assistance.
i. Consider contacting medical direction for advice.
ii. Document the patient’s refusal.
#302 Lecture Outline
G. Infectious diseases of the heart
1. Endocarditis
a. Infection of the inner lining of the heart characterized by endocardium inflammation
b. Occurs when bacteria in the bloodstream colonize a heart valve or other damaged tissue in the heart and begin to multiply
#303 Lecture Outline
c. Highest risks in patients with:
i. Mitral or aortic valve disease
ii. Prosthetic heart valves
iii. Congenital heart disease
d. Right-sided endocarditis
i. Affects the tricuspid and pulmonary valves
ii. IV drug users
iii. Patients with infected central venous catheters, dialysis shunts, or transvenous pacing wires
#304 Lecture Outline
e. Assessment
i. Symptoms
(a) Fever
(b) Chills
(c) Headache
(d) Loss of appetite
(e) Weight loss
(f) Muscle and joint aches and pains
(g) Night sweats
(h) Shortness of breath
(i) Cough
(j) Heart failure
(k) Janeway lesions
(l) Osler nodes
ii. ECG changes may be seen, including a prolonged PRI, third-degree AV block, or LBBB.
#305 Lecture Outline
f. Management
i. Care is supportive.
ii. Allow the patient to assume a position of comfort.
iii. Establish an IV line.
iv. Apply the cardiac monitor.
v. Apply a pulse oximeter and administer oxygen, if indicated.
vi. If the patient has heart failure, follow local protocol and medical direction.
#306 Lecture Outline
g. Treatment
i. Antibiotics
ii. Surgery in severe cases
h. If the patient refuses care, repeatedly urge the patient to accept assistance.
i. Consider contacting medical direction for advice.
ii. Document the patient’s refusal.
#307 Lecture Outline
2. Pericarditis
a. An inflammation of the pericardium
i. Caused by either a viral (most common), bacterial, or, occasionally, fungal infection
(a) In many cases, no cause can be identified (idiopathic pericarditis).
b. Assessment
i. Ask the patient about recent flulike signs and symptoms.
(a) Patients may relate a history of a recent upper respiratory infection.
ii. Chest discomfort is the most common symptom of pericarditis.
iii. Sharp, stabbing chest pain that is made worse by deep inspiration, coughing, or lying flat
iv. Pain decreases when sitting up and forward.
v. Listening to heart sounds may reveal a pericardial friction rub.
(a) This sign is not always present.
vi. Signs include:
(a) Fever
(b) Tachycardia
(c) Tachypnea
(d) Pale skin
(e) JVD
(f) Normal breath sounds unless another condition exists
(g) ST-segment elevation in multiple ECG leads
#308 Lecture Outline
c. Management
i. Prehospital care is supportive.
(a) Allow the patient to assume a position of comfort.
(b) Establish an IV line.
(c) Apply a cardiac monitor.
(d) Apply a pulse monitor and administer oxygen.
(e) Obtain a 12-lead ECG.
(f) Transport without lights or siren.
d. Treatment
i. Pericarditis is treated with nonsteroidal anti-inflammatory drugs.
(a) Viral pericarditis: usually resolves on its own
(b) Bacterial pericarditis: treated with antibiotics
(c) Fungal pericarditis: treated with antifungal medications
e. If the patient refuses care, repeatedly urge the patient to accept assistance.
i. Consider contacting medical direction for advice.
ii. Document the patient’s refusal.
#309 Lecture Outline
3. Myocarditis
a. Inflammation of the myocardium
b. Usually benign and self-limiting
c. If untreated, will impair heart’s ability to pump and may result in:
i. RVF
ii. LVF
iii. Dysrhythmia
iv. Death
v. Dilated cardiomyopathy
d. Can be caused by:
i. Bacteria
ii. Viruses
iii. Parasites
iv. Heart transplant rejection
v. Rheumatic fever
vi. Exposure to chemical poisons (alcoholism; radiation therapy)
vii. Unknown factors
e. Assessment
i. Most cases are associated with flulike symptoms for which the patient does not seek care.
ii. Symptoms include:
(a) Fatigue
(b) Decreased appetite
(c) Mild shortness of breath
(d) Joint and muscle aches and pains
(e) Fever
(f) Palpitations
(g) Chest discomfort, often a sharp, stabbing pain in the center of the chest
(h) Tachycardia
(i) Tachypnea
(j) Atrial or ventricular dysrhythmia
(k) RBBB or LBBB
(l) Crackles, ascites, peripheral edema if heart failure is present
iii. The ECG may show low-voltage QRS complexes, pathologic Q waves, and/or non-specific ST-segment and T-wave abnormalities.
iv. Differential diagnoses to consider for myocarditis include the following:
(a) ACS
(b) Aortic dissection
(c) Esophageal perforation, rupture, or tear
(d) Heart failure
(e) Kawasaki disease
(f) Pneumonia
(g) Pulmonary disease
f. Management
i. Prehospital care is supportive.
(a) Allow the patient to assume a position of comfort.
(b) Establish an IV line.
(c) Apply a cardiac monitor.
(d) Apply a pulse monitor and administer oxygen.
(e) Obtain a 12-lead ECG.
(f) Treat heart failure and dysrhythmia according to local protocol or instructions from medical direction.
#310 Lecture Outline
4. Rheumatic fever
a. Inflammatory disease caused by streptococcal bacteria
b. Causes aortic or mitral valve stenosis, leading to heart complications
c. Supportive prehospital care
#311 Lecture Outline
5. Scarlet fever
a. Scarlet fever is caused by the Streptococcus pyogenes bacterium.
b. Signs and symptoms include:
i. Sore throat
ii. Fever
iii. Rash
iv. “Strawberry tongue”
c. Patients younger than 1 year are at greatest risk.
d. Treated with antibiotics, and prehospital care is supportive
#312 Lecture Outline
H. Vascular disorders
1. Aortic aneurysm
a. An aneurysm is the dilation or outpouching of a blood vessel or the wall of a chamber of the heart.
b. If the vessel wall tears, then its layers can separate in a process called dissection.
i. May begin with a tear in the inner lining of the aorta (the intima) near the weakened portion of the vessel
ii. Blood flows through the tear and between the layers of the vessel wall, exposing the middle layer to blood under high pressure.
iii. Blood fills the space between the layers of the vessel, causing them to separate (dissect).
#313 Lecture Outline
iv. With each ventricular systole, blood is forced into the torn arterial wall, creating a false channel between the intimal and medial layers of the wall.
v. If the dissection goes back to the aortic valve, it may not be able to close.
(a) Blood will regurgitate into the left ventricle during systole.
(b) Coronary blood flow will often be compromised.
#314 Lecture Outline
vi. If the dissection involves the takeoff point of the innominate, left common carotid, or left subclavian artery, blood flow through the affected arteries will be diminished.
vii. Most begin in the ascending aorta within 2 inches (5 cm) of the aortic valve or in the descending thoracic aorta at the site of the ligamentum arteriosum.
c. Risk factors:
i. Tobacco smoking
ii. High blood cholesterol
iii. Hypertension
iv. CHD
d. Aneurysms of the ascending thoracic aorta are usually caused by cystic medial degeneration, a connective tissue disease in which normal elastic tissue is replaced with cystlike connective tissue.
i. A mild form is often present in the aortas of older adults; it may be a natural consequence of aging.
ii. In younger people, it is accompanied by Marfan syndrome, vascular Ehlers-Danlos syndrome, and Loeys-Dietz syndrome.
iii. Connective tissue disease
iv. Congenital issues
(a) Infective endocarditis
(b) Untreated infection
(c) Trauma
#315 Lecture Outline
e. Assessment
i. Signs and symptoms depend on the location.
(a) The pressure of a large amount of blood on surrounding organs may produce symptoms.
ii. The patient’s description of the pain provides clues to the location of the dissection.
(a) Almost all patients report the abrupt onset of constant, unbearable pain.
#316 Lecture Outline
(b) Ascending aorta dissection is usually associated with pain that is either:
(1) Substernal
(2) Located in the neck, throat, jaw, or face
(c) Descending aortic dissection usually produces:
(1) Flank pain
(2) Pain between the shoulder blades
(3) Pain in the back, abdomen, or lower extremities
iii. It may be difficult to distinguish the chest pain of a dissecting aneurysm from that of an AMI, but a number of distinctive features may help differentiate it.
#317 Lecture Outline
iv. Symptoms include:
(a) Anxiousness; feeling of impending doom
(b) Pain, weakness, or numbness and tingling in the extremities
(c) Signs of myocardial ischemia
(d) Heart failure
(e) Altered mental status
(f) Stroke
(g) Paraplegia
(h) Cardiac arrest
(i) Sudden death
(j) Syncope
#318 Lecture Outline
v. Ascending aorta dissections occur in younger patients previously in good health.
(a) One or more of the vessels of the aortic arch is compromised.
(b) Pressure differences greater than 20 mm Hg between the arms may indicate the presence of an aortic aneurysm.
(c) Suspect dissection if this finding is accompanied by acute neurologic changes.
(d) May show signs and symptoms of stroke
(e) ECG changes characteristic of myocardial ischemia may occur when the dissection extends proximal to the coronary artery ostia.
#319 Lecture Outline
vi. Descending aorta dissections are more common in older patients, especially in those with a history of hypertension.
(a) Pain is less severe than ascending aorta dissections.
(b) Distal pulses may be hard to feel.
(c) Rupture of a thoracic aneurysm may occur.
(1) Signs of hemothorax may be present if the dissection ruptures into the pleural cavity.
(2) Signs of cardiac tamponade may be present if the dissection ruptures into the pericardial cavity.
(d) Rupture of an abdominal aortic aneurysm may occur.
(1) Will ordinarily be associated with sudden back pain
(2) Accompanied by abdominal pain and tenderness
(3) The patient might be hypotensive and have a pulsating abdominal mass between the xiphoid process, and an umbilicus may be present.
(4) Sensitive to palpation and may be quite tender
(5) Abdominal distention usually occurs.
(6) Massive GI hemorrhage may be present.
#320 Lecture Outline
f. Management
i. The goal of prehospital management is to provide adequate pain relief and rapid transport.
(a) Contact medical direction immediately.
(b) Avoid procedures that may delay transport to definitive care.
(c) Establish an IV line.
(d) Apply the cardiac monitor.
(e) Apply a pulse oximeter and administer oxygen, if indicated.
(f) Give IV fluids and medications per local protocol or medical direction.
(g) Administer opioids if the patient’s blood pressure can tolerate it.
ii. Reassess the patient at least every 5 minutes en route to the facility.
(a) The patient requires aggressive therapy in the intensive care unit and possibly surgery.
#322 Lecture Outline
a. Occlusion: sudden disruption of arterial blood flow that occurs because of:
i. Thrombus
(a) When the blockage affects an extremity, blood flow to the muscle is limited.
(b) During exercise, muscle contraction may stop blood flow.
(c) The process occurs gradually, allowing collateral circulation to develop.
(d) If extensive collateral circulation develops, the patient may notice no change or only mild increase in symptoms.
#323 Lecture Outline
ii. Embolus (most common)
(a) Conditions that favor origination in the heart include AF, clot formation in the left ventricle after AMI, a rheumatic or prosthetic heart valve, and left ventricular aneurysm.
(b) Arterial emboli can travel to a variety of sites in the body, but most lodge in the femoral artery.
(c) Most emboli occur in patients with significant underlying heart disease.
iii. Tumor
#324 Lecture Outline
iv. Direct trauma to an artery, which can be caused by:
(a) An extremity injury
(b) Diagnostic procedure such as cardiac catheterization
(c) Dissecting aneurysm
(d) Vasospasm (usually attributable to IV drug use)
(e) Blockage of a vascular graft
v. Unknown factors
#325 Lecture Outline
b. Acute limb ischemia results when an arterial occlusion suddenly reduces blood flow to an arm or leg.
c. Note the following concerning peripheral arterial disease (PAD):
i. 10% of patients experience intermittent claudication, including pain, cramping, muscle tightness, fatigue, or weakness of the legs when walking or during exercise.
ii. Symptoms occur as a result of increased oxygen demand during activity.
iii. The arteries that supply the muscles of the calves, hips, or buttocks are narrowed or blocked by atherosclerotic plaques that limit blood flow to the tissues.
iv. Symptoms disappear after a brief rest, and the patient can resume activity until the pain recurs.
v. 40% of patients do not complain of leg pain and present with atypical symptoms such as leg tiredness or fatigue.
vi. The remaining 50% are asymptomatic despite an abnormal pulse examination or have leg symptoms different from classic claudication.
#326 Lecture Outline
d. Assessment includes:
i. Gathering an accurate history
(a) If symptoms occurred suddenly, an embolus is the probable cause.
(b) If symptoms occurred gradually, thrombus is the probable cause.
(c) Find out if the patient has ever had a similar episode.
#327 Lecture Outline
ii. Keeping in mind the five Ps of acute arterial occlusion:
(a) Pain: usually begins distal to the site of obstruction and gradually increases in severity
(1) May be a decrease in pain as sensory loss progresses
(b) Pulselessness
(c) Pallor
(d) Paresthesia: sign of life-threatening ischemia
(e) Paralysis: sign of life-threatening ischemia
#328 Lecture Outline
iii. Finding out whether the patient has risk factors for developing a blood clot:
(a) Recent extremity injury
(b) IV drug use
(c) Heart surgery or AMI
(d) Clotting disorder
(e) Pulmonary embolism
(f) AF
(g) Contraceptive use
(h) Hormone replacement therapy
(i) Rheumatic heart disease
iv. Reviewing the skin color of the affected limb
(a) The skin of the affected limb usually appears pale or mottled distal to or over the affected area.
(b) The foot will turn pale when it is raised and very red after 1 minute of placing it at a level lower than the heart.
(c) The skin of the affected limb may feel cool and may be either moist or dry.
(d) Feel the brachial, radial, femoral, posterior tibial, and dorsalis pedis arteries in pairs.
(e) Peripheral pulses may be absent or diminished in the affected limb.
v. Assessing movement and sensation in all extremities
vi. Checking heart rate and rhythm
vii. Checking the patient’s blood pressure in both arms
viii. Listening for a bruit over the affected vessel or vessels
ix. Watching for signs of chronic limb ischemia, which may be present if the patient has had symptoms of peripheral arterial disease for some time
#329 Lecture Outline
e. Management
i. Allow the patient to assume a position of comfort.
ii. If limb ischemia affects a lower extremity, sit the patient up, and place the patient’s feet lower than the chest.
iii. Establish an IV line.
iv. Apply the cardiac monitor.
v. Apply a pulse oximeter and administer oxygen, if indicated.
#330 Lecture Outline
vi. Give medications as instructed by medical direction, including pain medications.
vii. Keep the patient compartment of the ambulance warm to avoid cold-induced vasoconstriction of the skin.
viii. Transport rapidly to the closest appropriate facility.
ix. Reassess the patient’s condition frequently en route.
#331 Lecture Outline
x. Monitor the five Ps.
xi. If the patient refuses care, repeatedly urge him or her to accept your assistance, including transport.
(a) Consider contacting medical direction for advice.
(b) Document patient’s refusal.
#332 Lecture Outline
3. Acute deep vein thrombosis (DVT)
a. Thrombophlebitis: the development of a blood clot in an inflamed or damaged vein
i. Superficial thrombophlebitis: occurs when a clot develops in a vein near the surface of the skin
ii. DVT: present if a clot develops in the deep veins of the extremities
(a) Associated with an increased risk of pulmonary embolism
#333 Lecture Outline
iii. Three important factors in developing a thrombus:
(a) Venous stasis, or sluggish blood flow
(1) Patients who are pregnant, immobile for long periods, and those with obesity or heart failure
(b) Damage to the inner lining of the vessel
(1) Caused by trauma, inflammation, venipuncture, or the action of agents given during IV therapy
(c) Blood clotting disorders
(1) Caused by dehydration, certain types of cancer, and use of oral contraceptives, hormone replacement therapy, or infertility treatment
#334 Lecture Outline
b. Assessment
i. The patient with DVT may seek medical care because of swelling, pain, or tenderness in a limb.
(a) Find out if the patient has risk factors for DVT.
#335 Lecture Outline
ii. Carefully assess the patient’s upper and lower extremities.
(a) Compare the extremities in pairs.
iii. Look for signs of inflammation of the skin over the affected vein.
iv. Look for pain and tenderness of the calf muscle on dorsiflexion of the foot (Homan sign).
v. Be careful not to rub or massage the affected limb.
(a) Could dislodge a clot (thromboembolism)
#336 Lecture Outline
vi. The differential diagnoses for DVT include:
(a) Arthritis
(b) Cellulitis
(c) Muscle or soft-tissue injury
(d) Superficial thrombophlebitis
#337 Lecture Outline
c. Management
i. Prehospital care is mainly supportive.
ii. Allow the patient to assume a position of comfort.
iii. Establish an IV line and apply the cardiac monitor.
iv. Apply a pulse oximeter and administer oxygen, if indicated.
v. Monitor the patient closely for development of a pulmonary embolism.
#338 Lecture Outline
vi. Transport without lights or siren.
vii. If the patient refuses care, repeatedly urge him or her to accept your assistance, including transport.
(a) Consider contacting medical direction for advice.
(b) Document patient’s refusal.
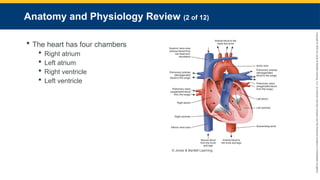
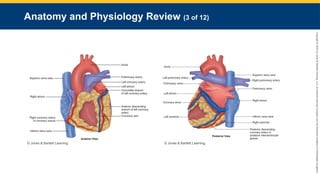





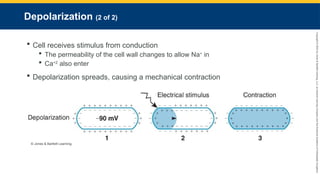
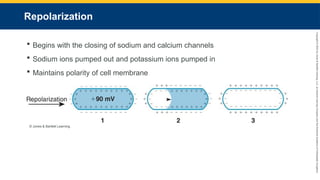
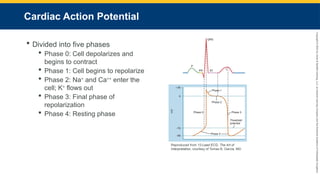
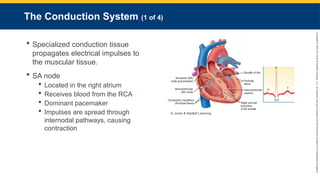
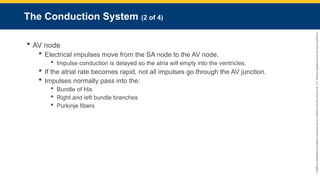
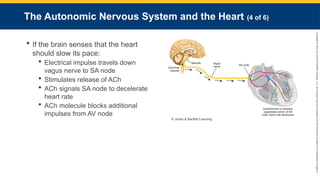
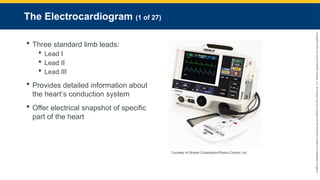
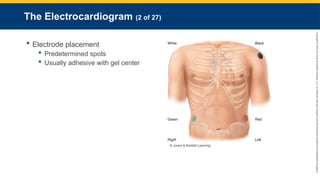

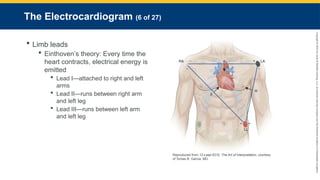
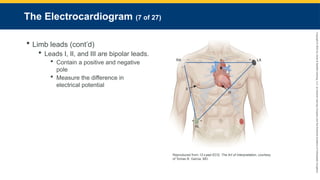

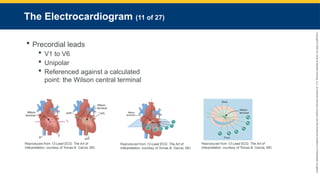
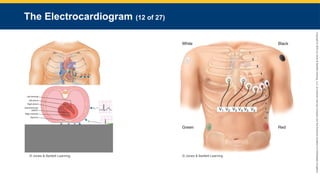
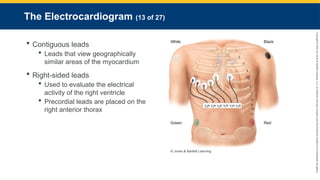
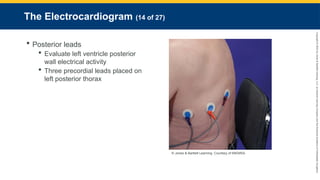

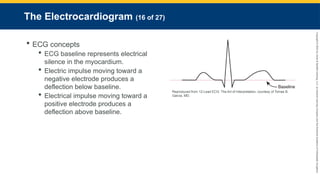
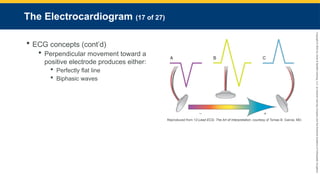

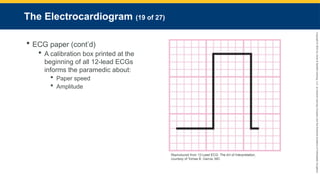
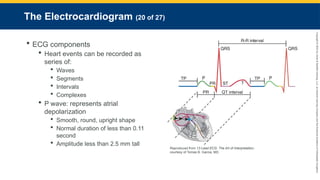
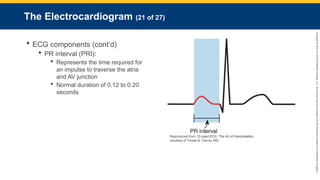
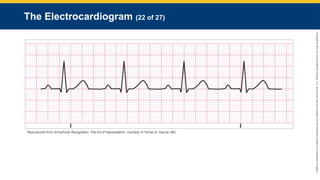
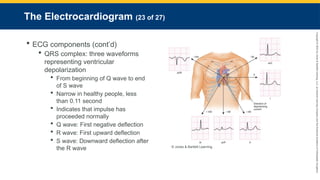

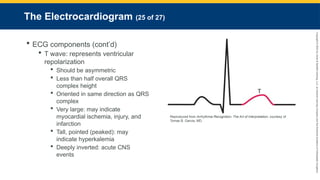
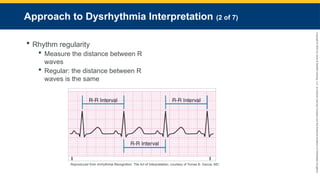
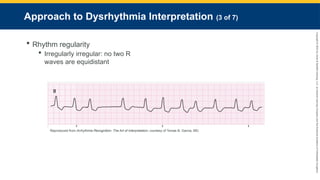
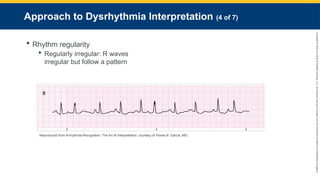
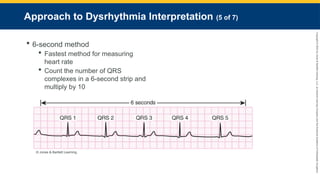
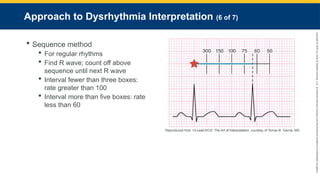
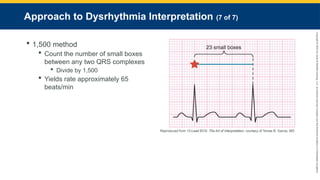
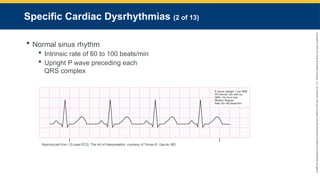
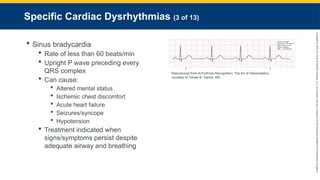
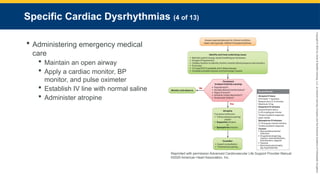
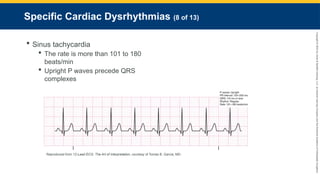
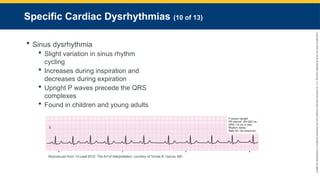
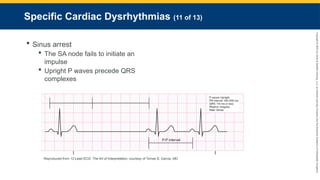
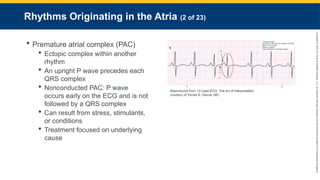
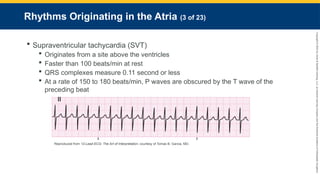
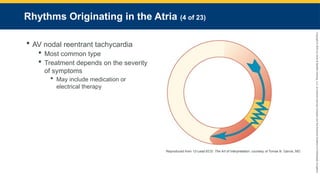


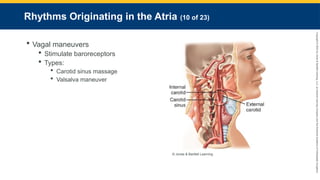
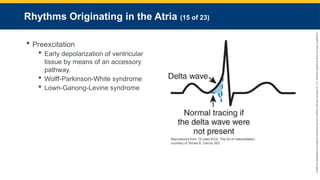
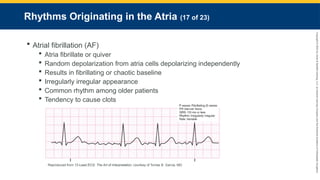
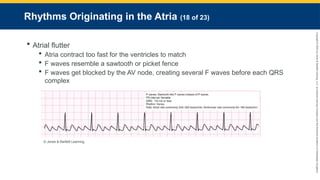
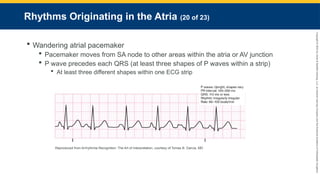
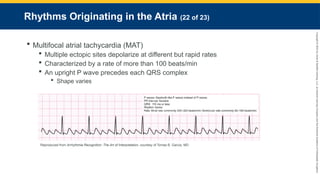
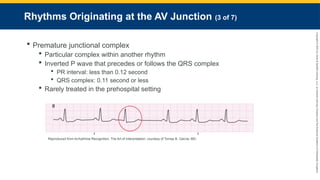
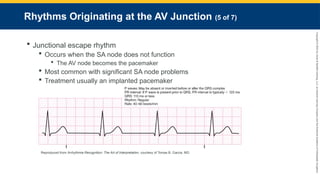
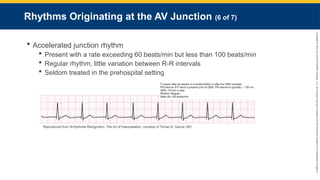
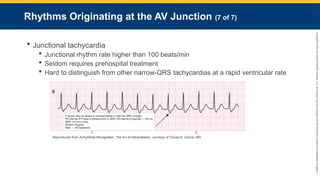

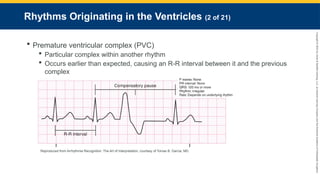
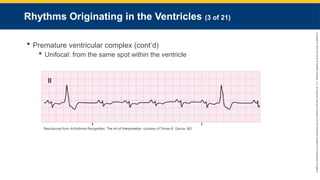
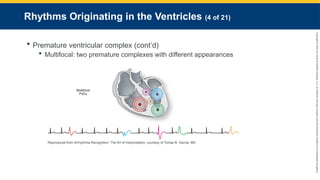
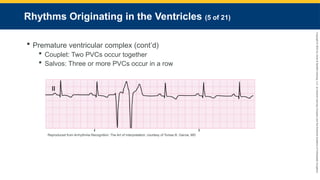
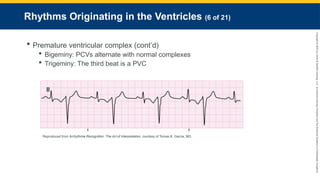
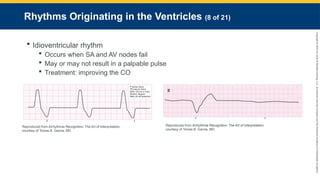
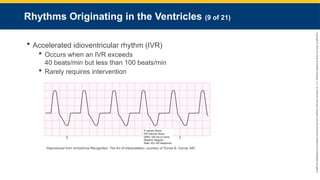
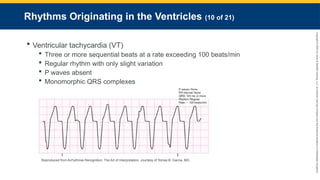
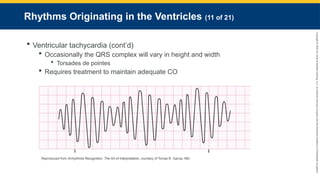
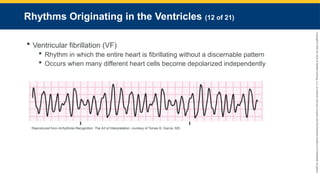
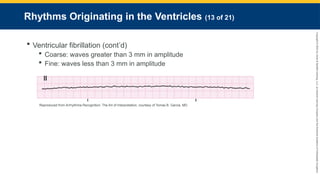

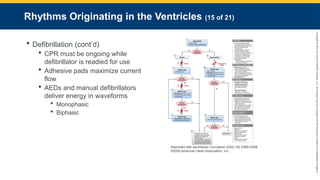

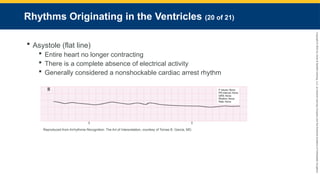






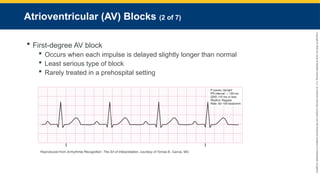

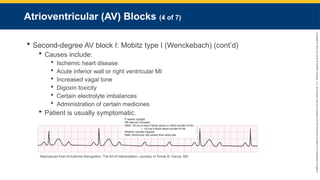
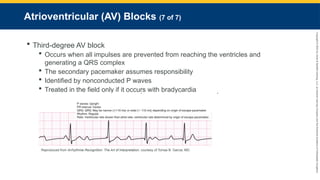
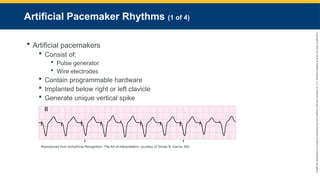
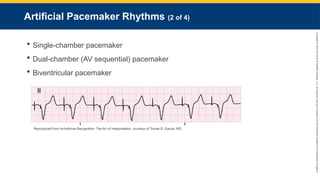
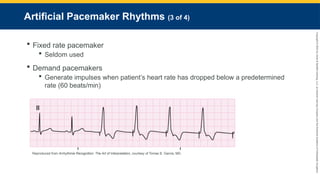


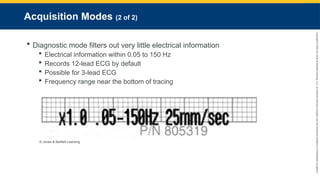

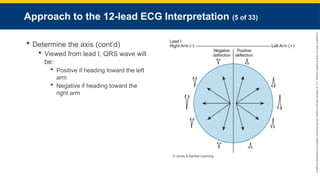
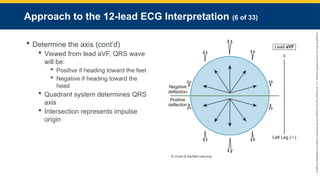
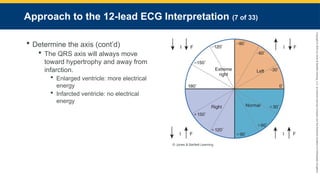

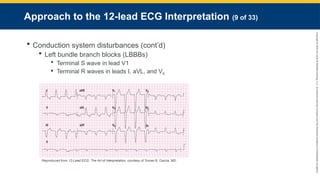
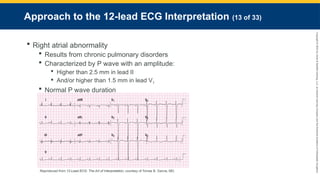
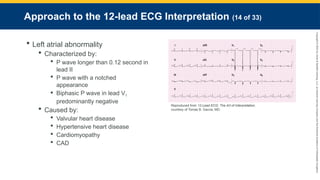
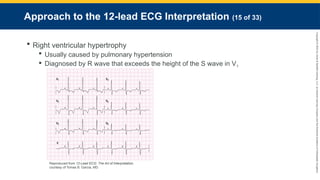
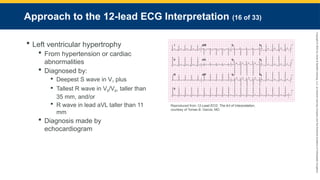

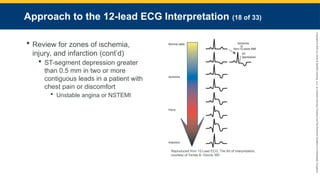
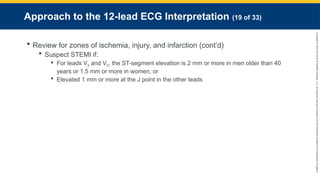

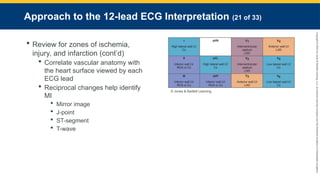
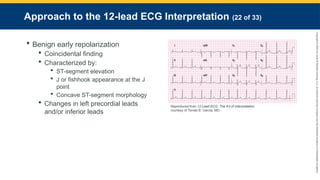
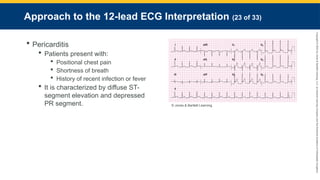
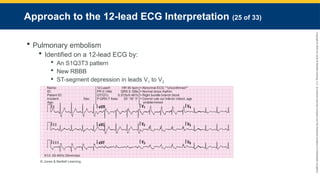
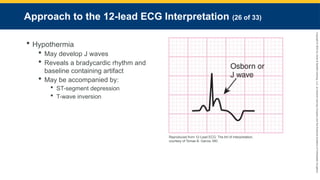
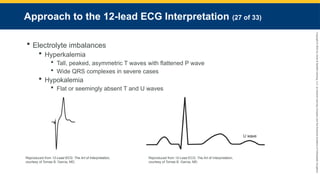

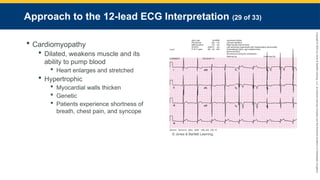
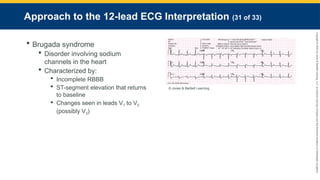
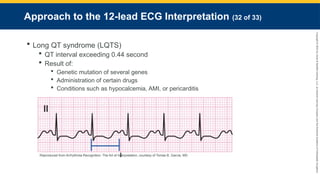
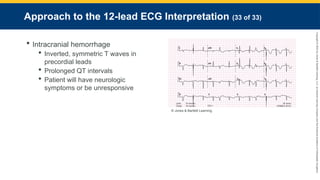





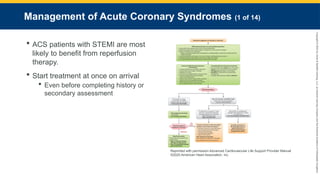

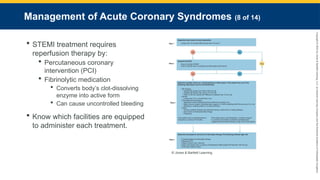


















































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)




![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)












