Download as PDF, PPTX
![Venugopalan.P.P; EMCME 2009;MIMS.CALICUT.15.03.09
ABCDEF
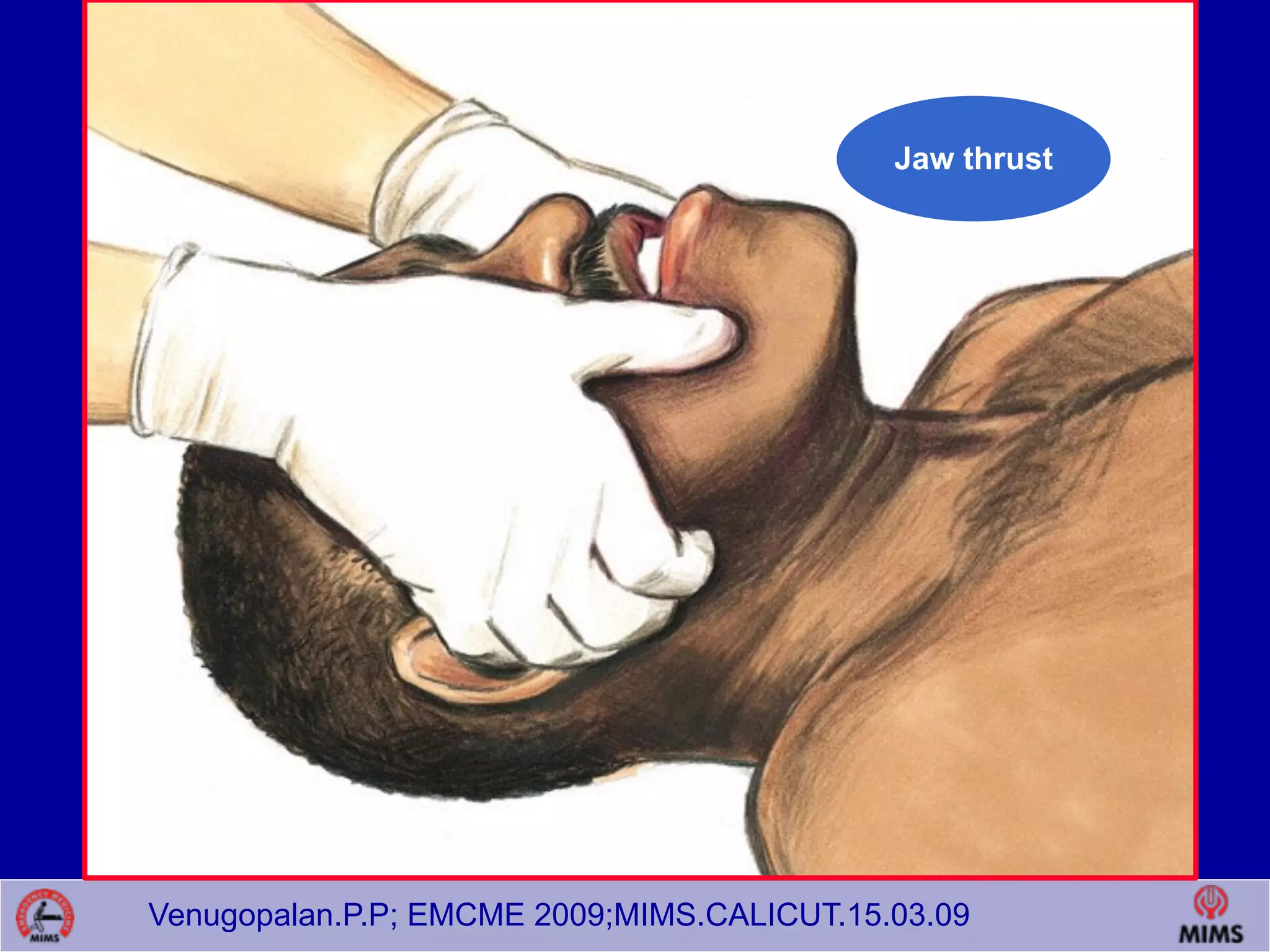
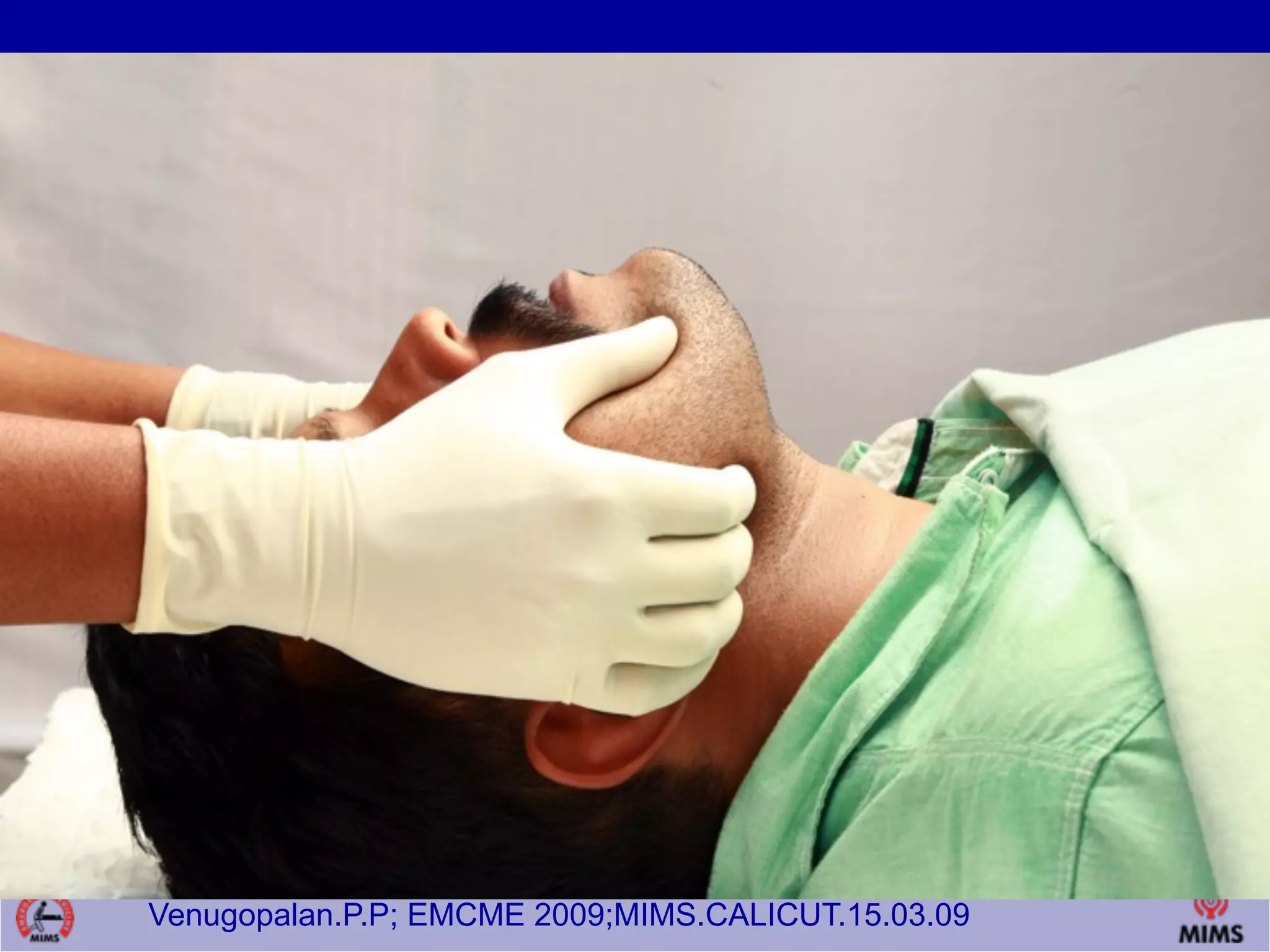
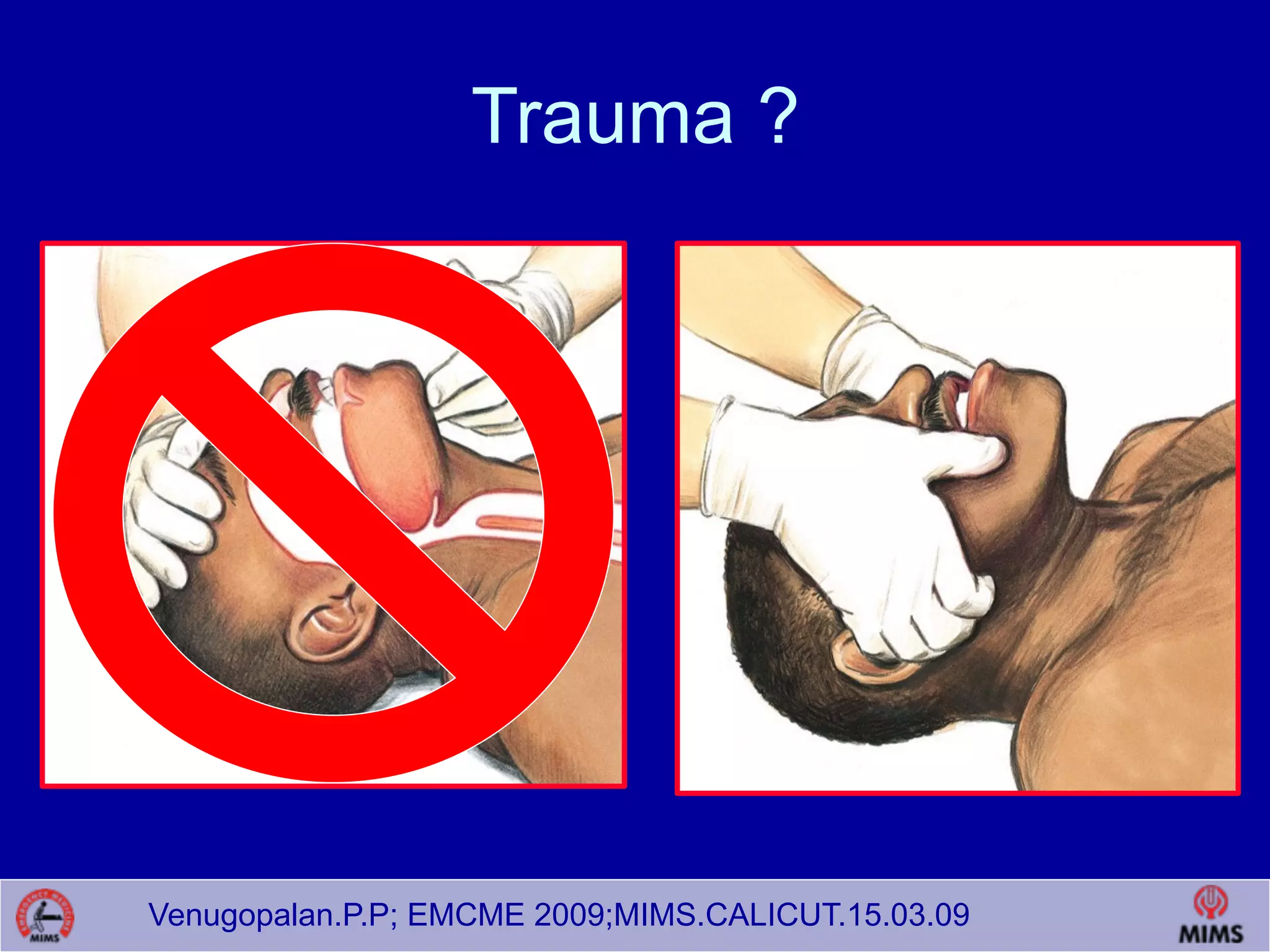
Airway - mouth and neck infections, tumors,
foreign bodies, bleeds
]exam: stridor, phonation, swallowing, secretions, dyspnea
Breathing failure of oxygenation or ventilation
often amenable to medical and non-invasive therapies – think NIV
Circulation supporting tissue oxygen delivery by
unloading the muscles of respiration
sepsis](https://image.slidesharecdn.com/airwayupdate-160620172053/75/Airway-management-in-ED-Basics-and-advanced-8-2048.jpg)






![Venugopalan.P.P; EMCME 2009;MIMS.CALICUT.15.03.09
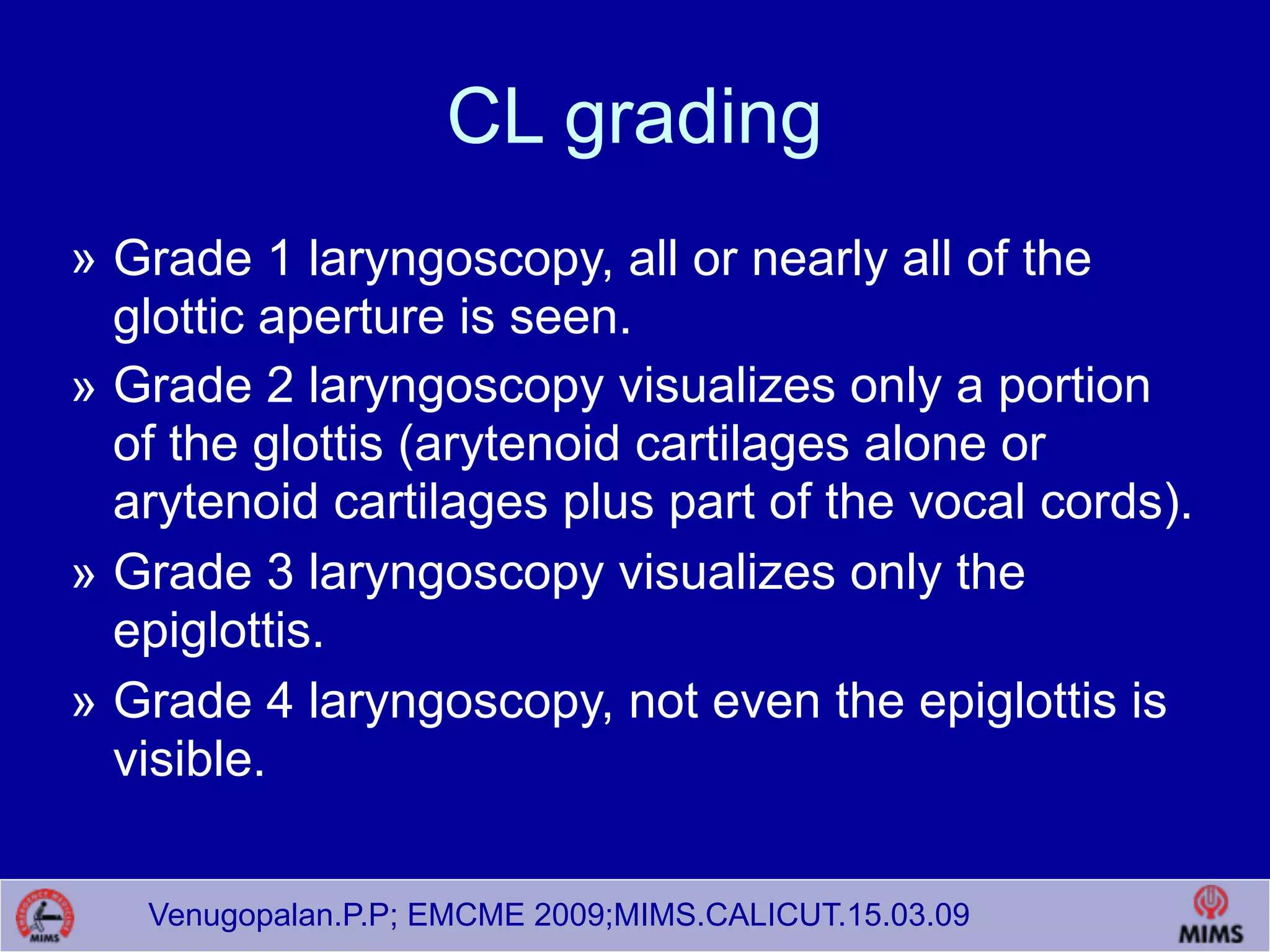
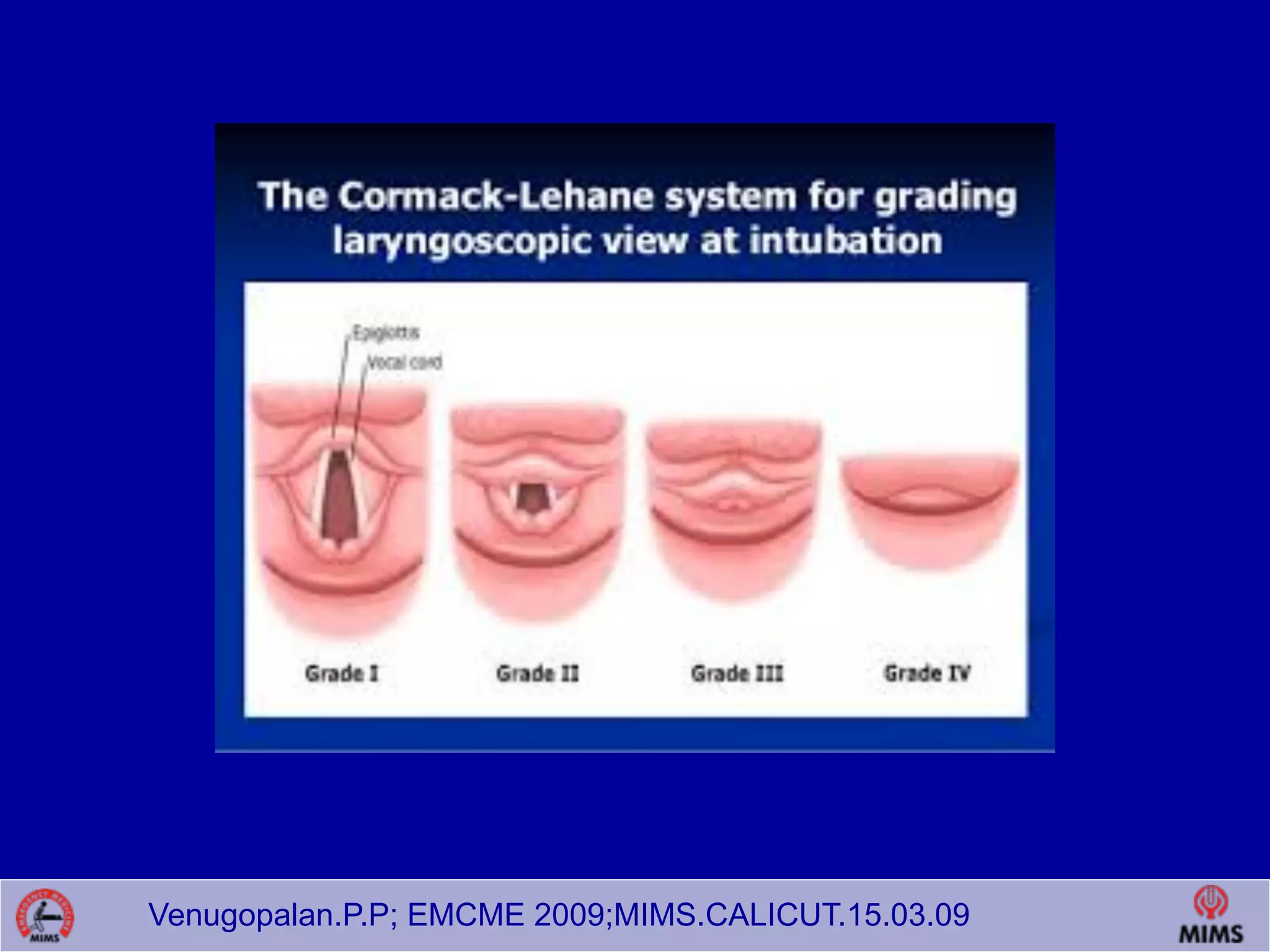
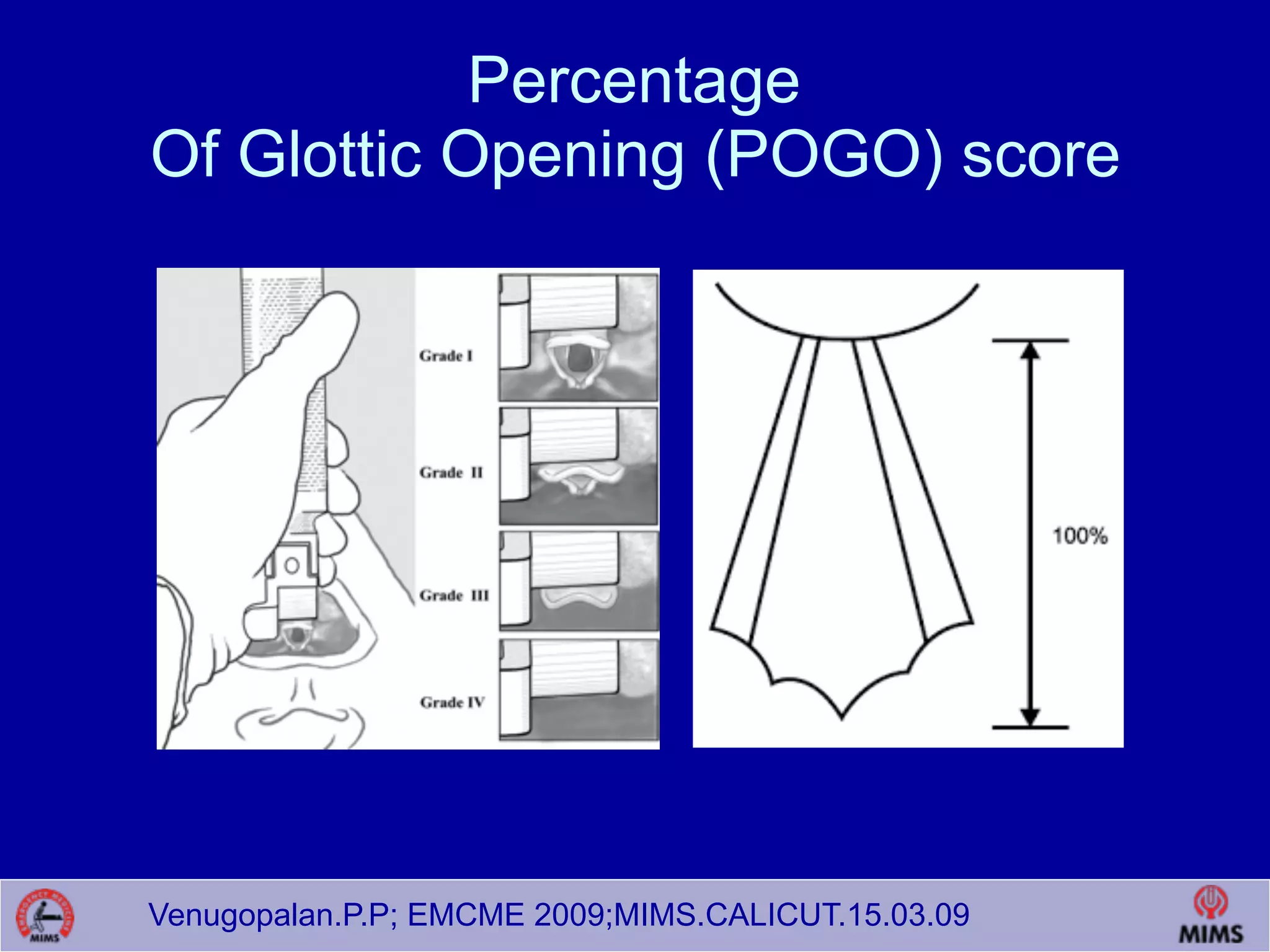
Cormack and Lehane[CL]
» The most widely used system for grading
laryngoscopic view of the glottis is that of
Cormack and Lehane (CL)
» Grades laryngoscopy according to the
extent to which laryngeal and glottic
structures can be seen.](https://image.slidesharecdn.com/airwayupdate-160620172053/75/Airway-management-in-ED-Basics-and-advanced-58-2048.jpg)
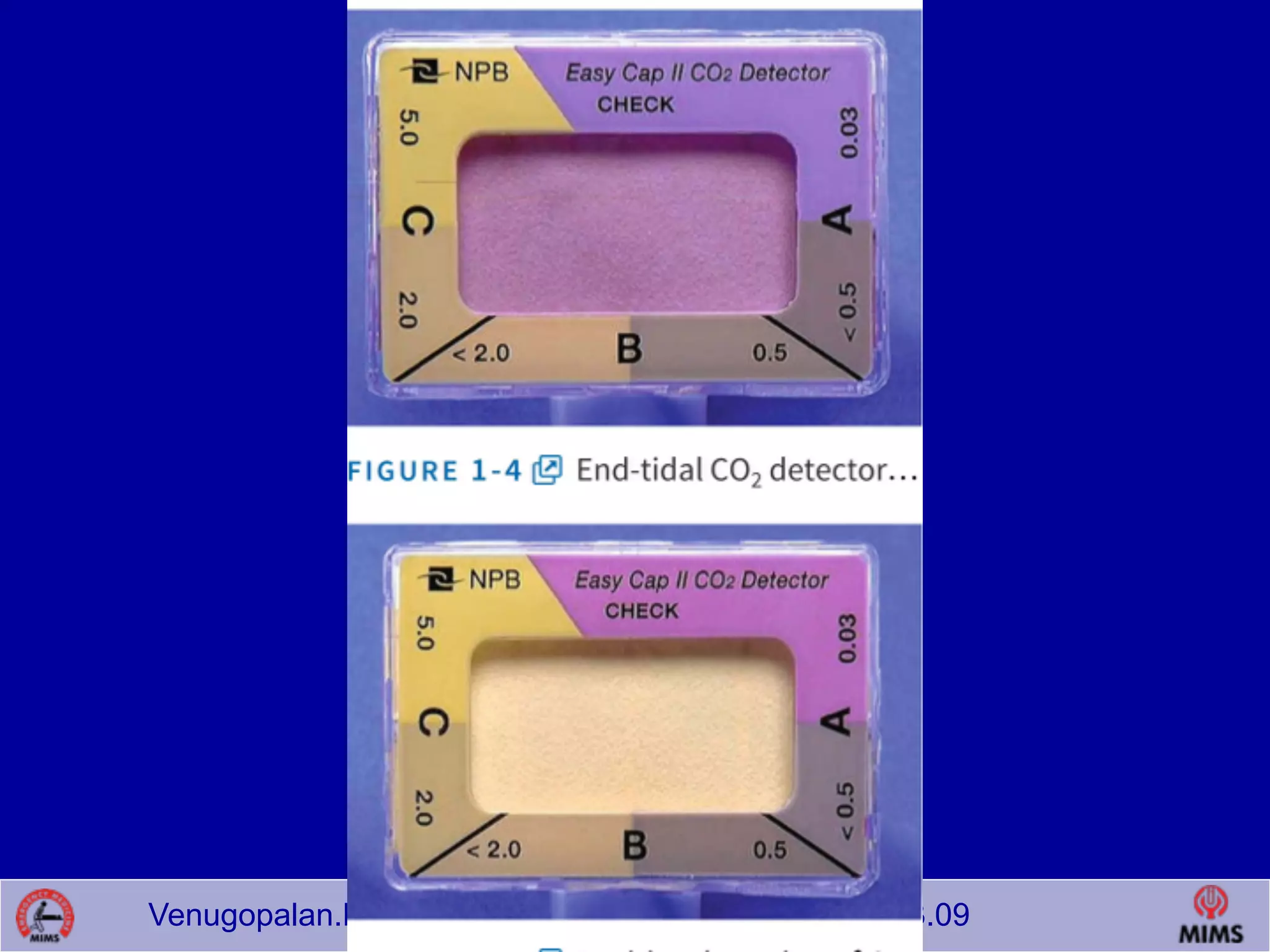
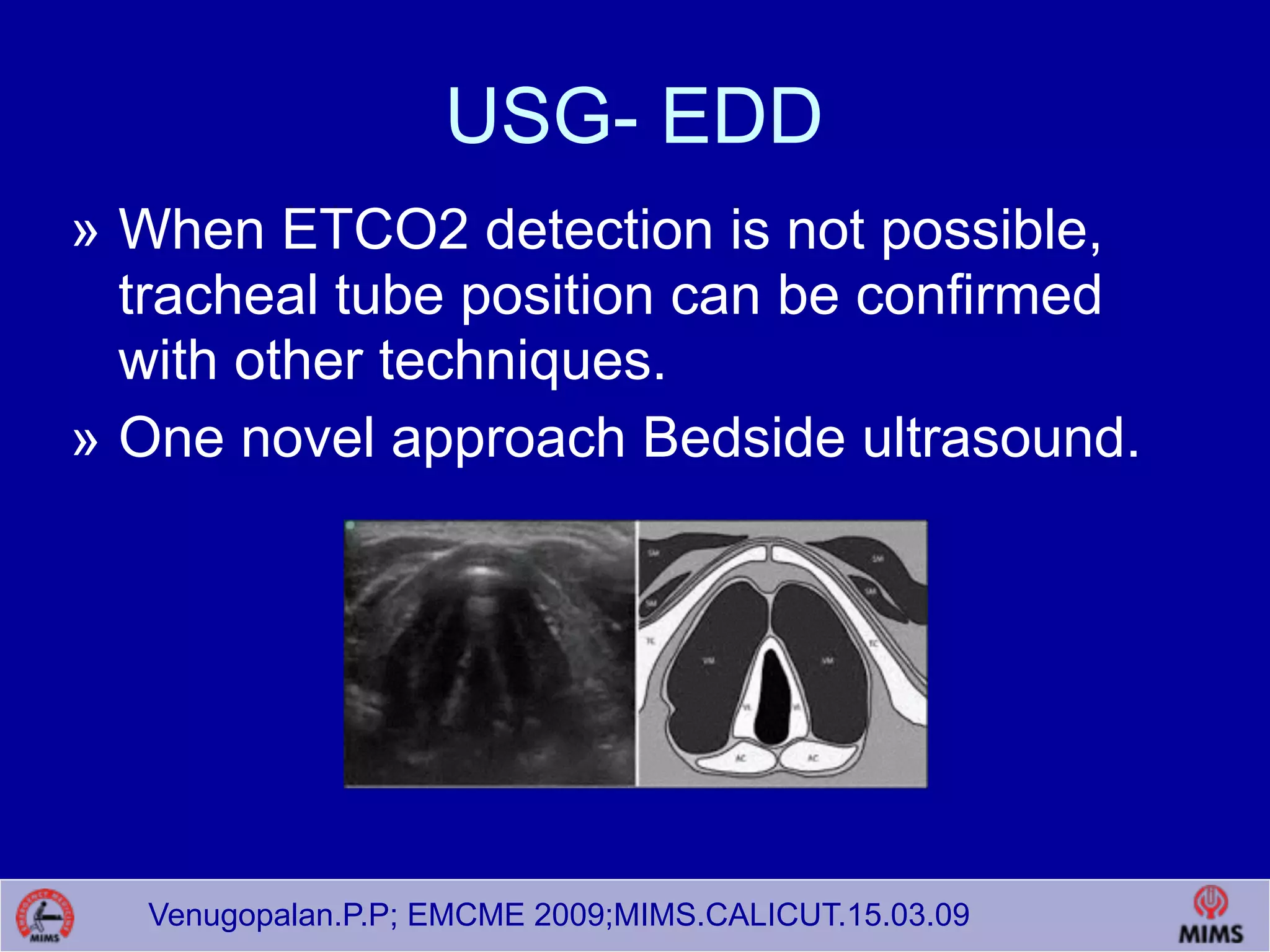

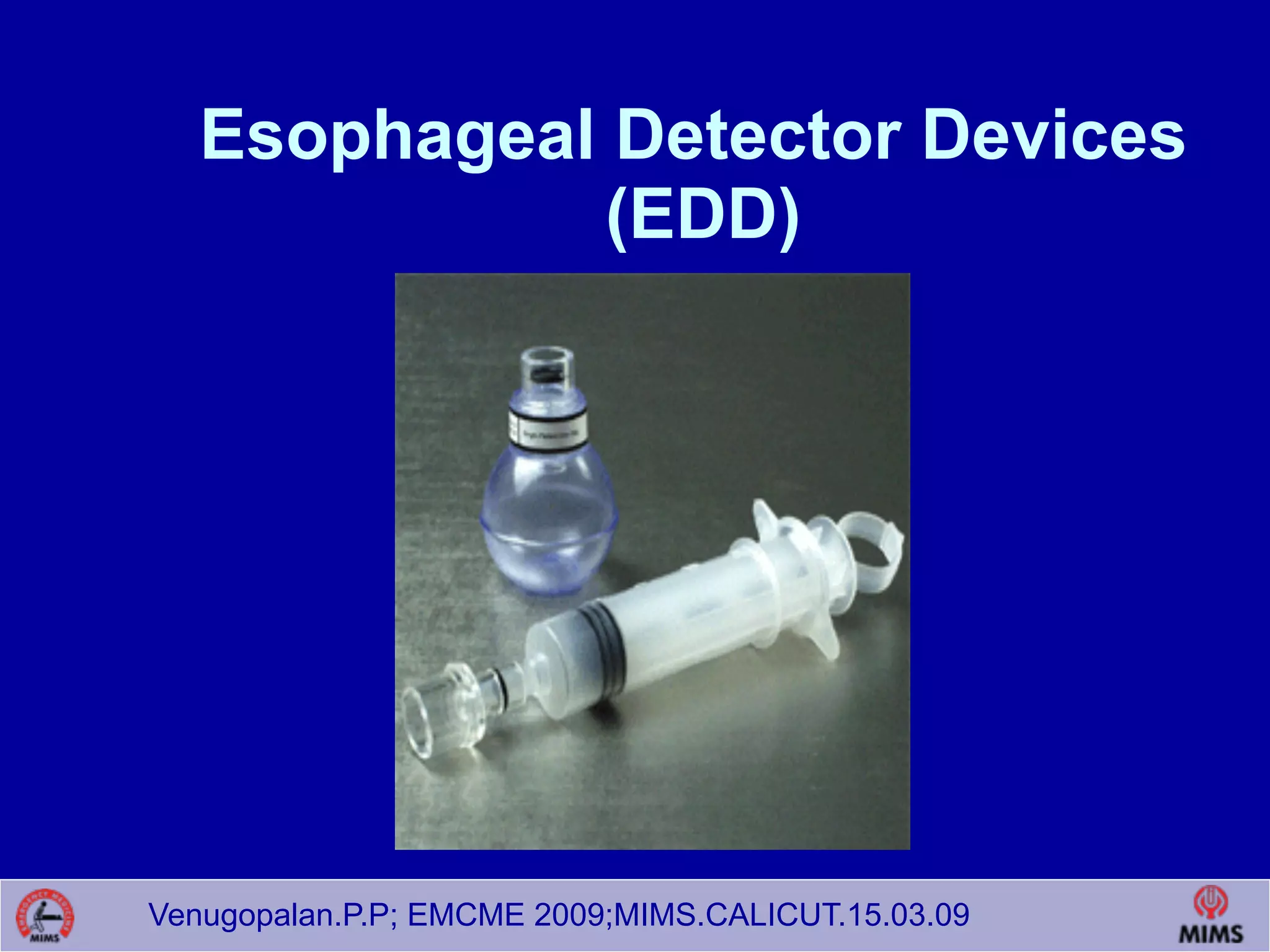











The document discusses airway management techniques in emergency room settings. It covers topics such as indications for intubation, assessing airway patency, use of basic adjuncts like oropharyngeal airways, nasopharyngeal airways and more advanced techniques like rapid sequence intubation. It also discusses techniques to confirm proper endotracheal tube placement like end-tidal CO2 detection, ultrasound and esophageal detector devices. The document aims to provide emergency physicians with updated knowledge on airway management.











































































































