Downloaded 1,013 times
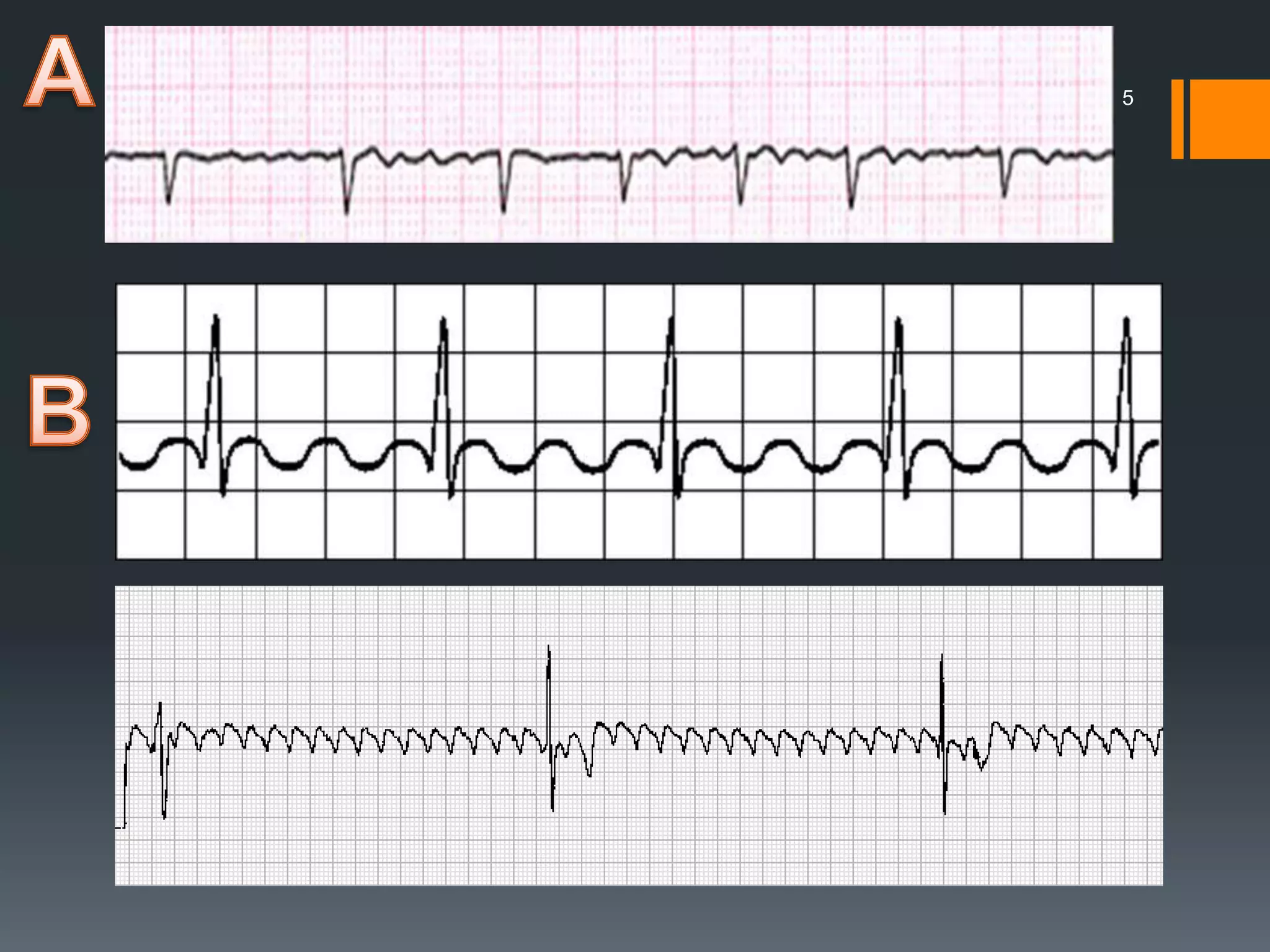
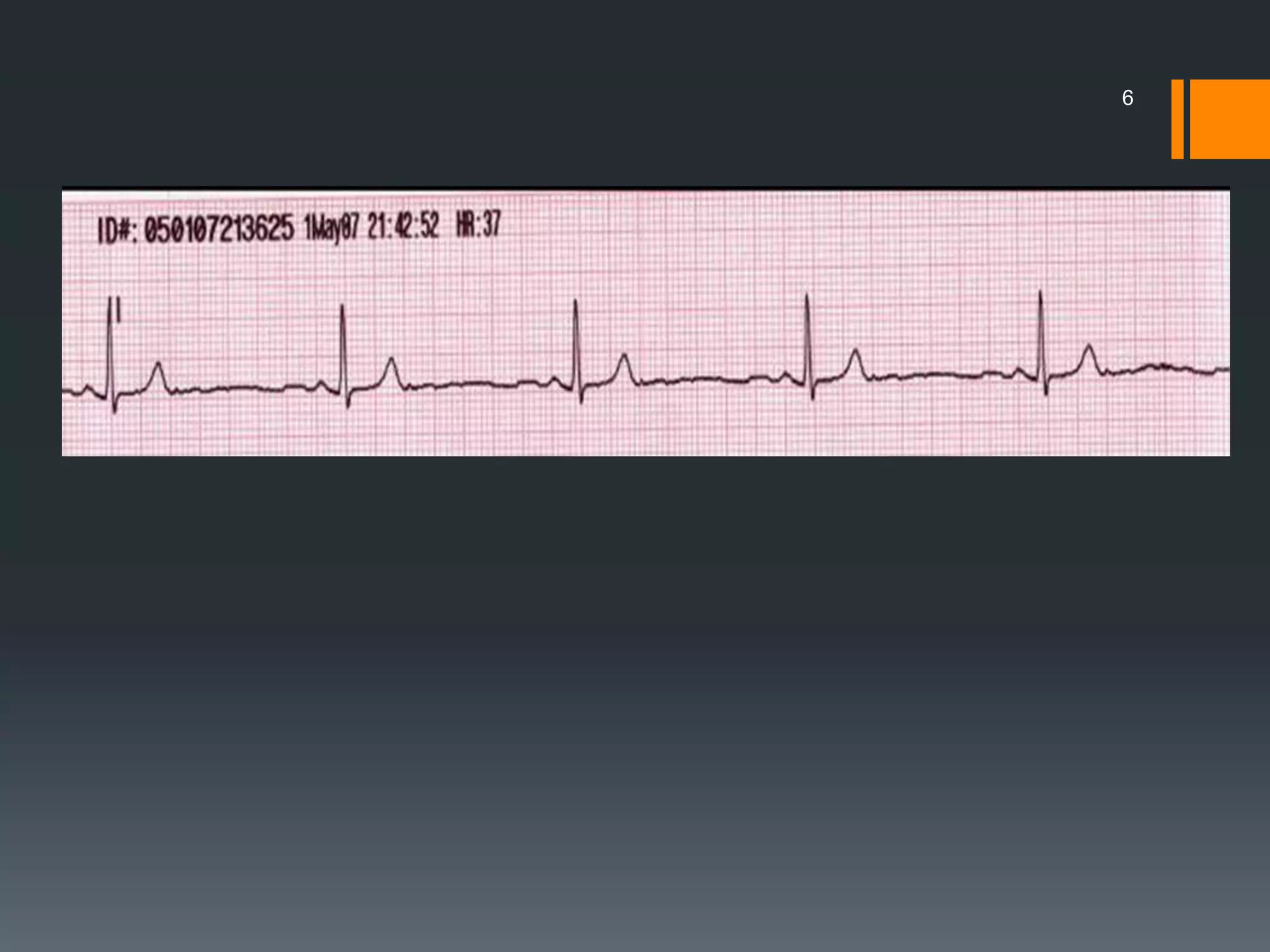
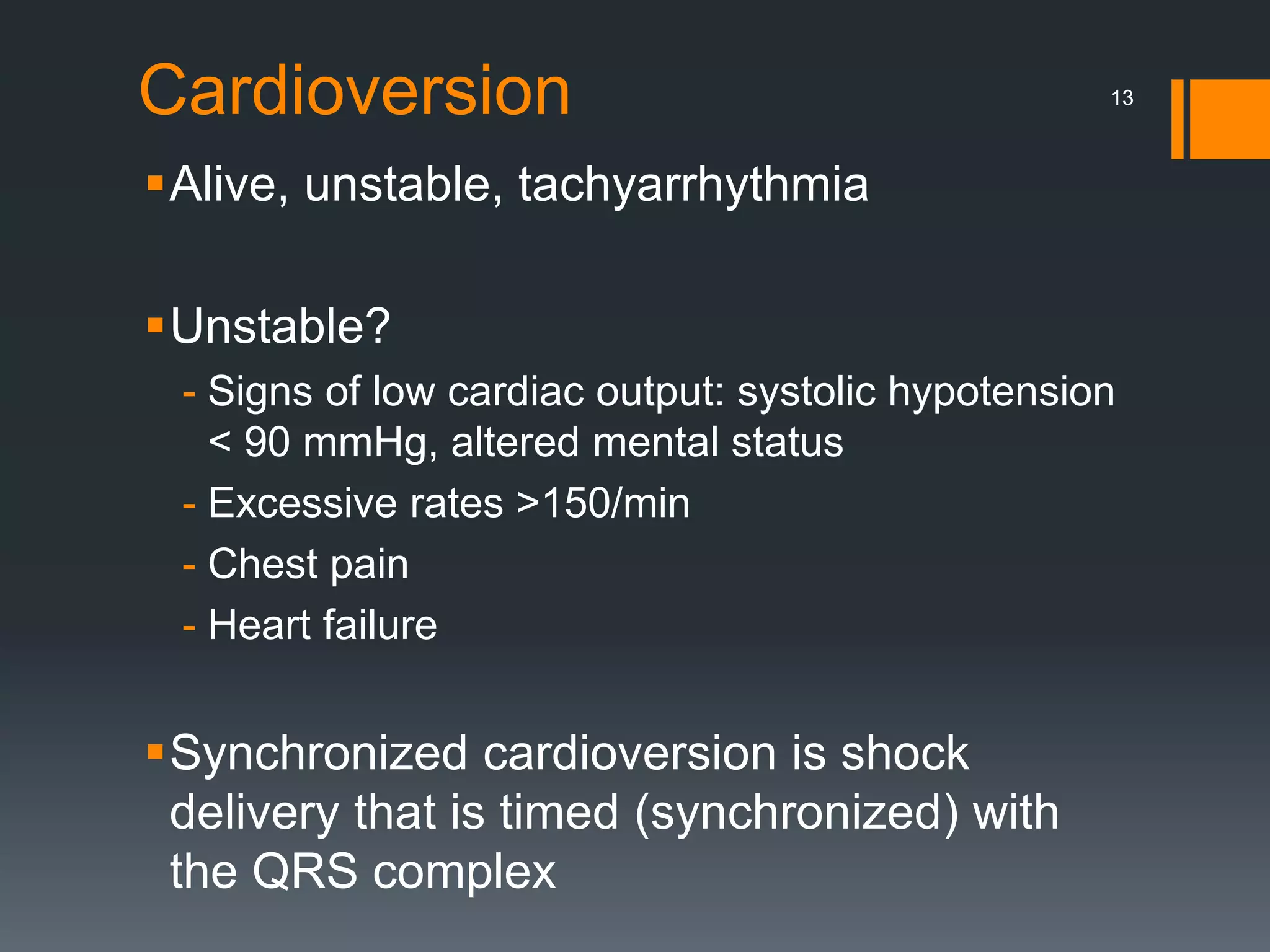

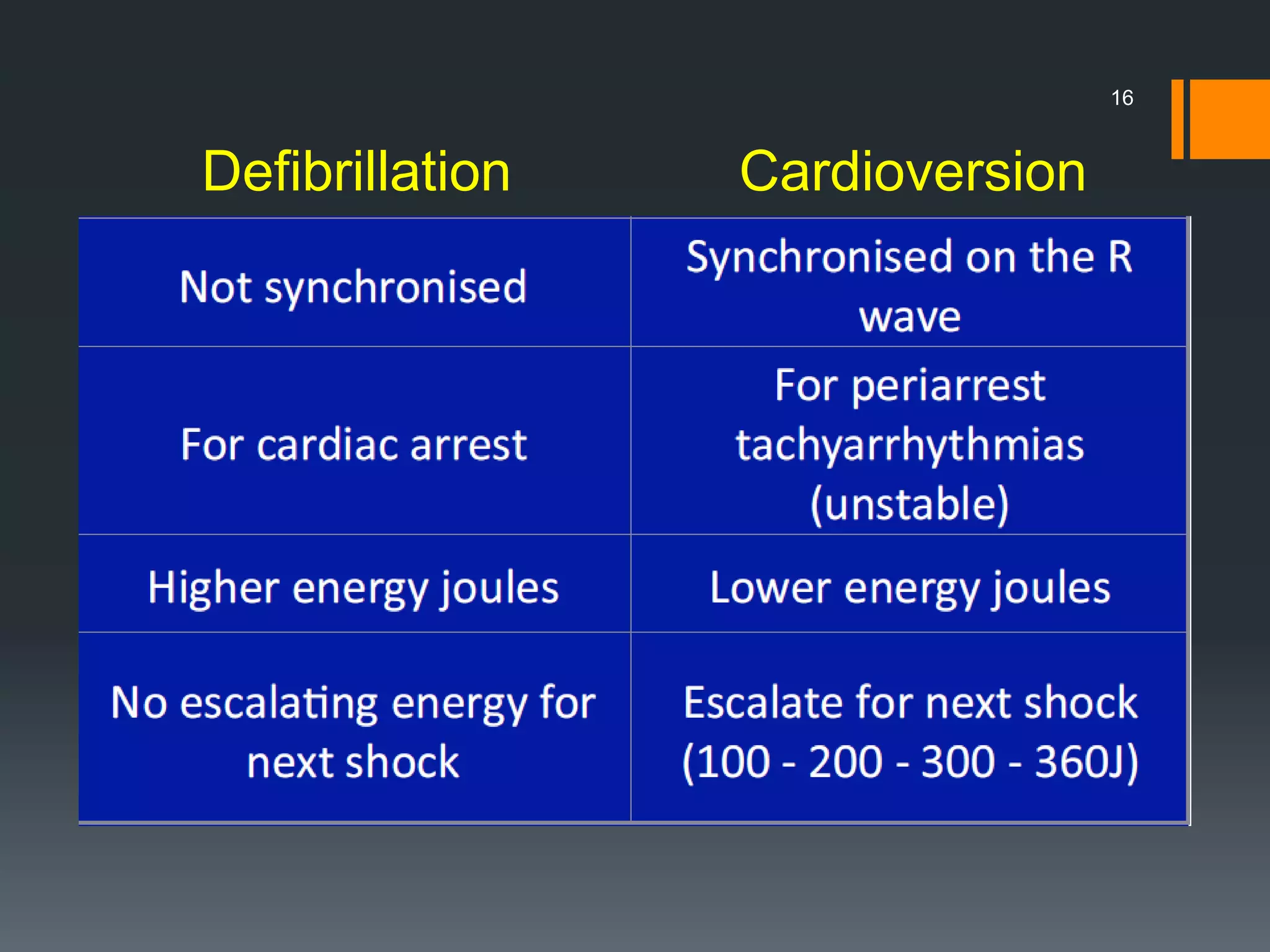
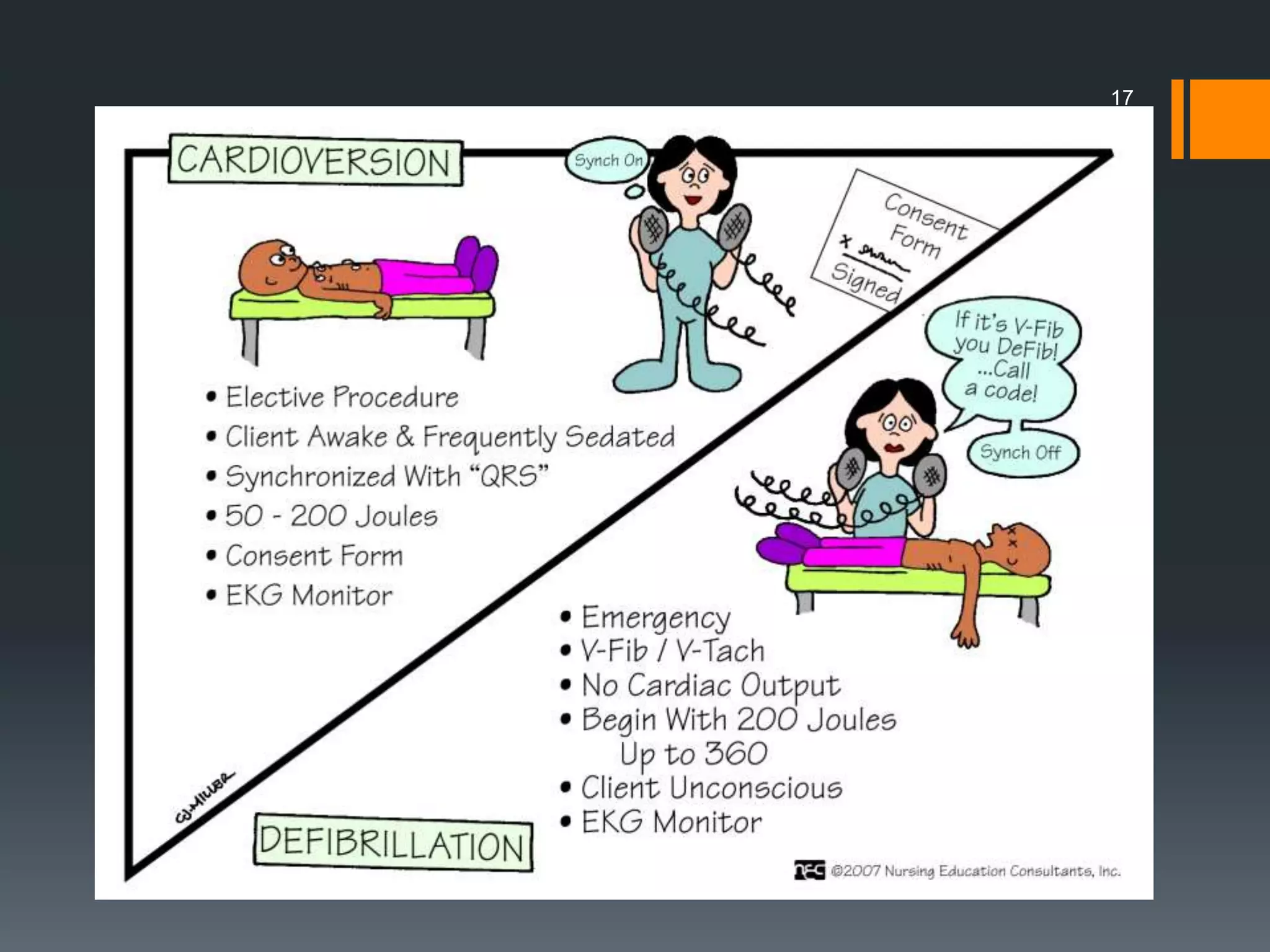
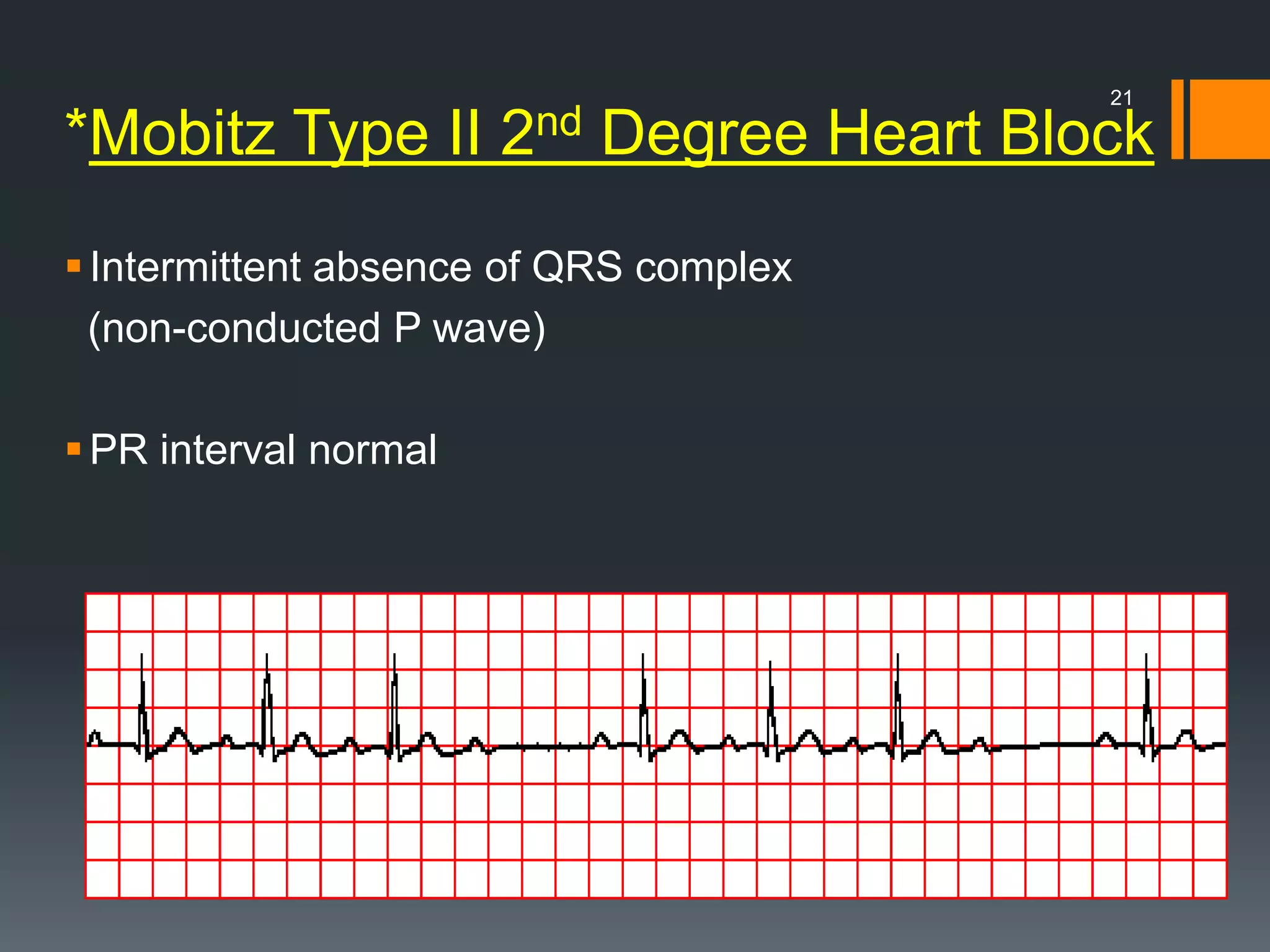
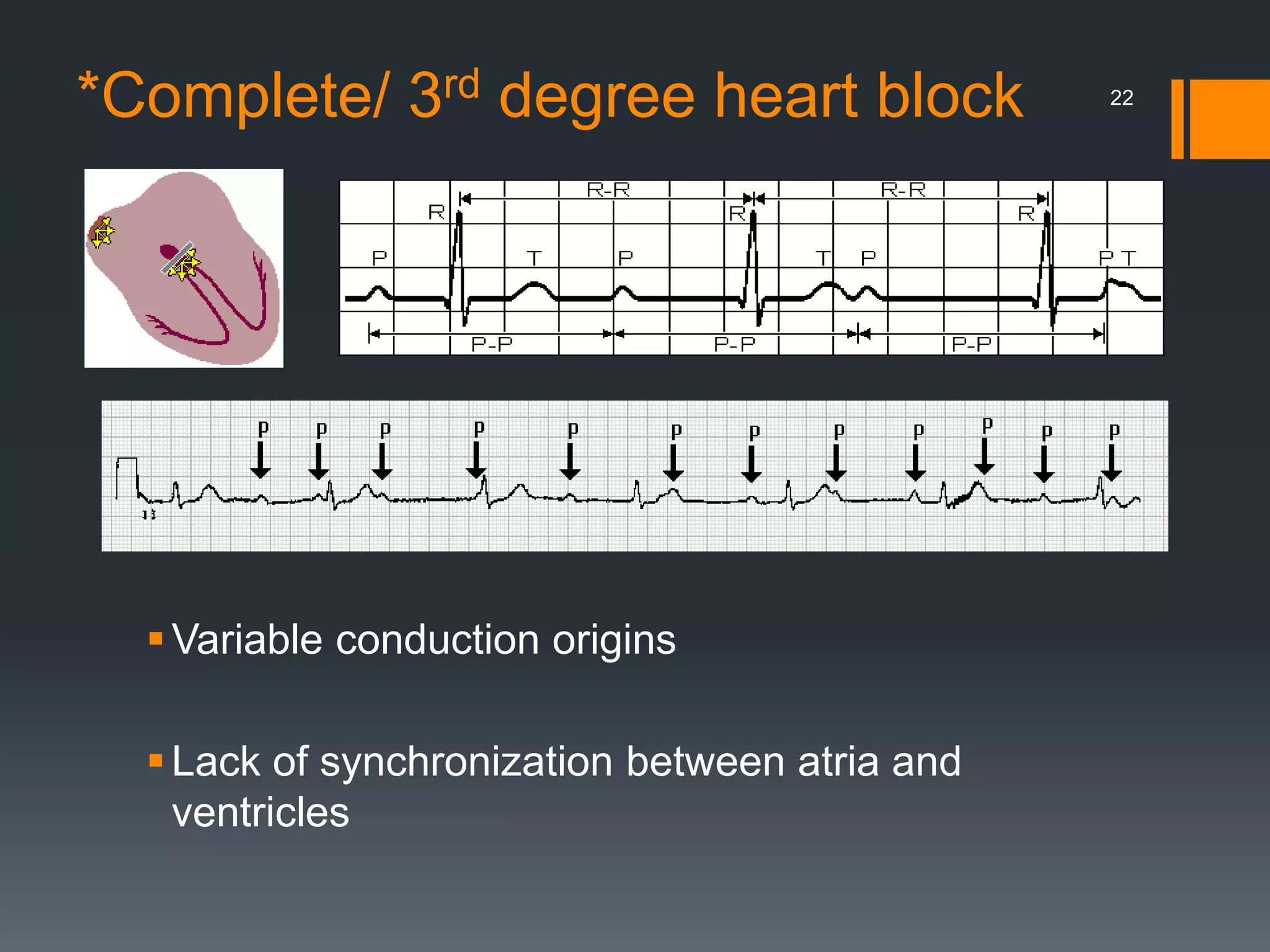
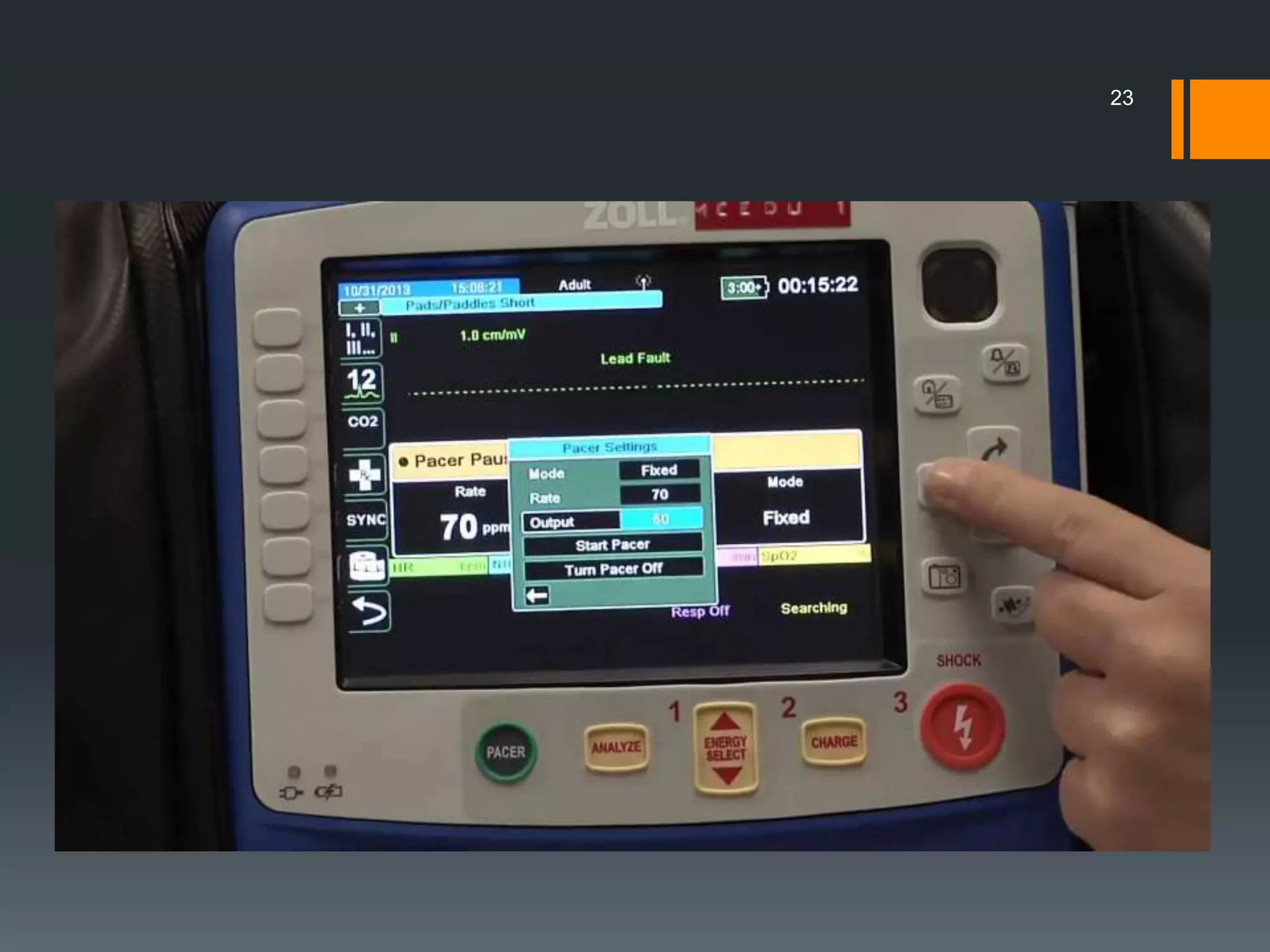
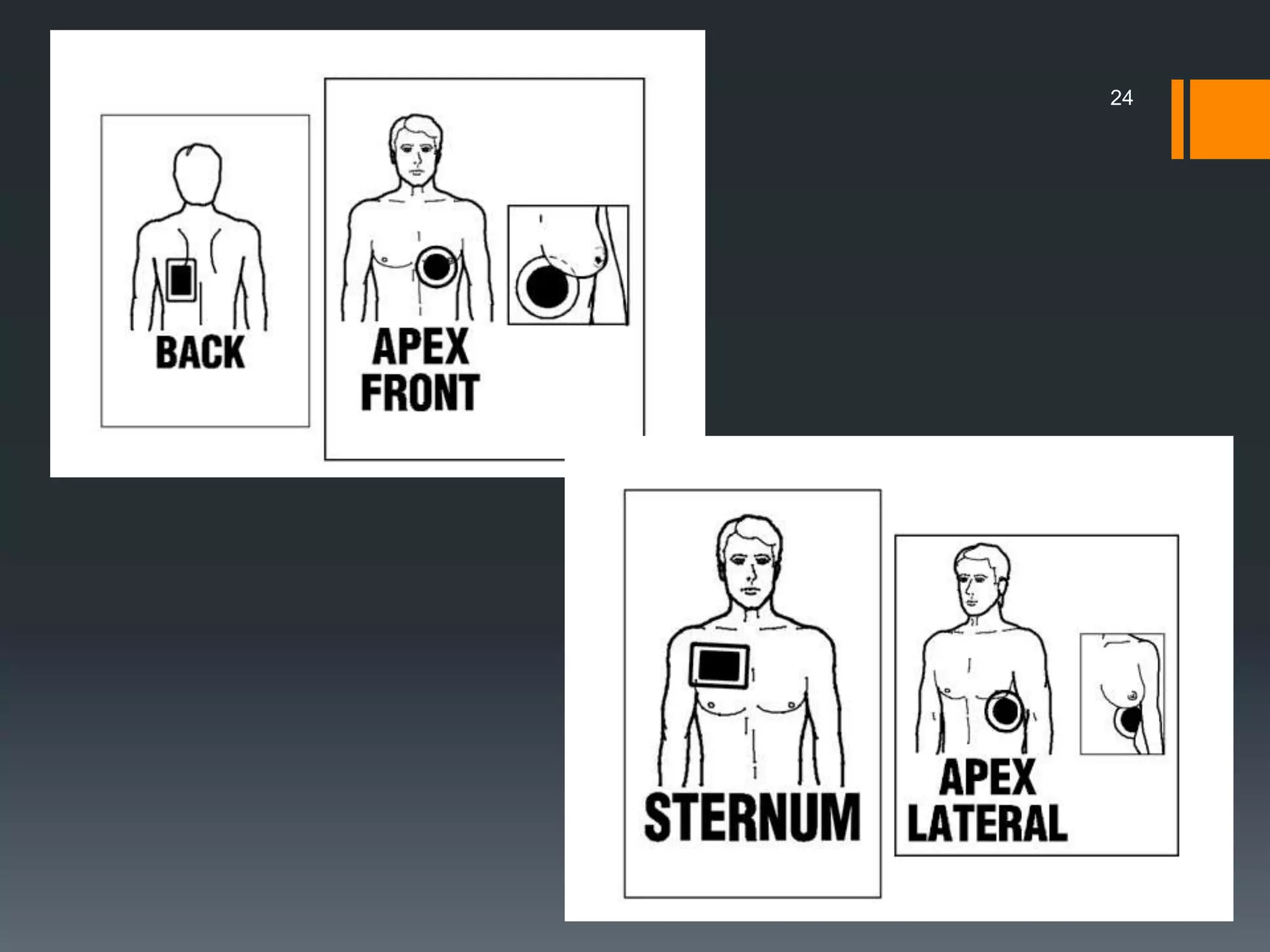

This document discusses defibrillation, cardioversion, and pacing. It provides: 1) A brief history of defibrillation and its use for ventricular fibrillation and pulseless ventricular tachycardia. 2) An overview of cardioversion for treating unstable tachyarrhythmias with signs of low cardiac output, excessive heart rates, or chest pain. Synchronized cardioversion times shock delivery to the QRS complex. 3) Information on pacing for unstable bradyarrhythmias and symptomatic bradycardia, including complete heart block and Mobitz type II second-degree heart block.























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)






